Article Text

Abstract
Background Preterm birth is a major global public health issue due to its prevalence, impact upon morbidity and mortality, and subsequent cost implications. Yet, policy analysis has not been undertaken to understand the different approaches across Europe to treatment decisions, and parental involvement in these decisions.
Methods A European survey and national guidance documentation analysis was undertaken with national neonatal or paediatric societies in Europe, exploring treatment decisions and parental involvement in decision-making for babies born at 22 to 25 completed weeks of gestation.
Results Responses were obtained from 19 European countries of 28 contacted. At 25 weeks of gestation there was universal initiation of active care at birth. At 24 weeks policy varied from initiating interventions (9), interventions dependent upon infant condition (8) and resuscitation restrictions (2). At 23 weeks and below, policy varied from no active intervention (7), individualised decision-making (8), parental permission required (3) and universal initiation of interventions (1). There were significant variations in the involvement of parents in the development of policy and in 16 countries the final decision regarding interventions rested with the attending doctor.
Implications There was little consensus as to how active intervention after birth at 22 to 25 weeks of gestation is managed, nor were parents included in the development of policy in many countries. At extremely low gestational ages, the criteria for or against active intervention at birth vary widely between different health systems in Europe
- Neonatology
- Resuscitation
- Intensive Care
- Health Service
Statistics from Altmetric.com
What is already known on this topic
-
Preterm birth is a major public health issue due to its prevalence, impact upon morbidity and society and subsequent cost implications.
-
Variation exists between countries regarding treatment guidelines for infants born at extremely preterm gestations, and parental involvement in these decisions.
-
Policy analysis has not been undertaken to understand the range of different approaches used throughout Europe.
What this study adds
-
Throughout Europe there was little consensus as to how active intervention after birth at 22 to 25 weeks of gestation is managed.
-
Parents were not included in the development of policy surrounding parental involvement in decision-making in many European countries.
-
Country is the biggest contributor towards whether or not active care is undertaken at extremely preterm gestations.
Objective
Preterm birth is a global public health issue: 14.9 million babies were estimated to be born at <37 weeks’ gestational age in 20101 and about 1% of all births are extremely preterm, defined by the WHO as less than 28 completed weeks of gestation.2 Major advances in medical technology have resulted in improvements in outcomes for these high risk infants in high income settings, but extremely preterm birth, particularly before 26 weeks of gestation,3 ,4 remains a primary determinant of neonatal mortality and morbidity,5 ,6 and the second leading cause of childhood death under 5 years of age.7 Population-based studies of infants born before 26 weeks have indicated that serious cognitive, neuromotor or sensory morbidity occurs in 50% of children in early adolescence.8
In parallel with advances in neonatal medicine, there has been increasing emphasis on involving parents in decision-making for their preterm baby.9 Due to the paradox between treatment decisions and the precision of outcome estimates at extremely low gestations, exact information on which to refine difficult decisions concerning the continuance of life-sustaining treatment is often lacking in the individual clinical context. Healthcare professionals must present parents with complex statistical information portraying risk and uncertainty of mortality and morbidity10; this results in decisions that are potentially biased by the perceptions and attitudes of parents and healthcare professionals towards potential disability and the infant's future quality of life.11 Furthermore, parents and healthcare professionals do not always agree on the perceived impact of disability,12 and attitudes to the continuation of life-sustaining treatment for extremely preterm infants may differ between parents, doctors and nurses.13 ,14 Dealing with uncertainty and conflicting interpretations is one of the most difficult aspects of neonatal care that parents have to deal with.10
As the extremely preterm infant cannot communicate a preference for treatment, decisions are made by proxy.15 The balance between the wishes of healthcare professionals and parents, usually based on the ethical principle of ‘best interest’, must be determined to make decisions for the infant. Due to the complexity of decision-making, many countries have developed guidelines for the perinatal care of women at high risk of extremely preterm delivery. In this paper, we explore the spectrum of European guidance on treatment decisions for infants born at extremely preterm gestations, and the involvement of parents in these decisions, to determine whether there is a shared European perspective. We have evaluated guidance for births from 22 to 25 completed weeks of gestation, where outcomes surrounding mortality and morbidity are most uncertain.
Design
In order to gather European data on guidelines for treatment at extremely preterm gestations, a standard letter was sent to all of the neonatal associations in EU Member States and associated countries in November 2010. Contact details for all societies within Europe were gathered in collaboration with the European Foundation for the Care of Newborn Infants or through the Internet if unknown. Presidents or other senior officials of each association were asked to provide data relating to: treatment recommendations by gestational week, the role of the parents in decision-making, methods for resolution of divergent views, ultimate decision-maker in cases of divergent views and the management of non-viable infants. All countries were asked to send the national policies or guidelines within their country which underpinned their responses to ensure physician bias was reduced. A response chart was sent to each association to allow for ease of data collection. Two reminder emails were sent to all societies, along with an individual verification email in 2012 to confirm the results sent by that particular society. Data were collated by MK and HB.
Results
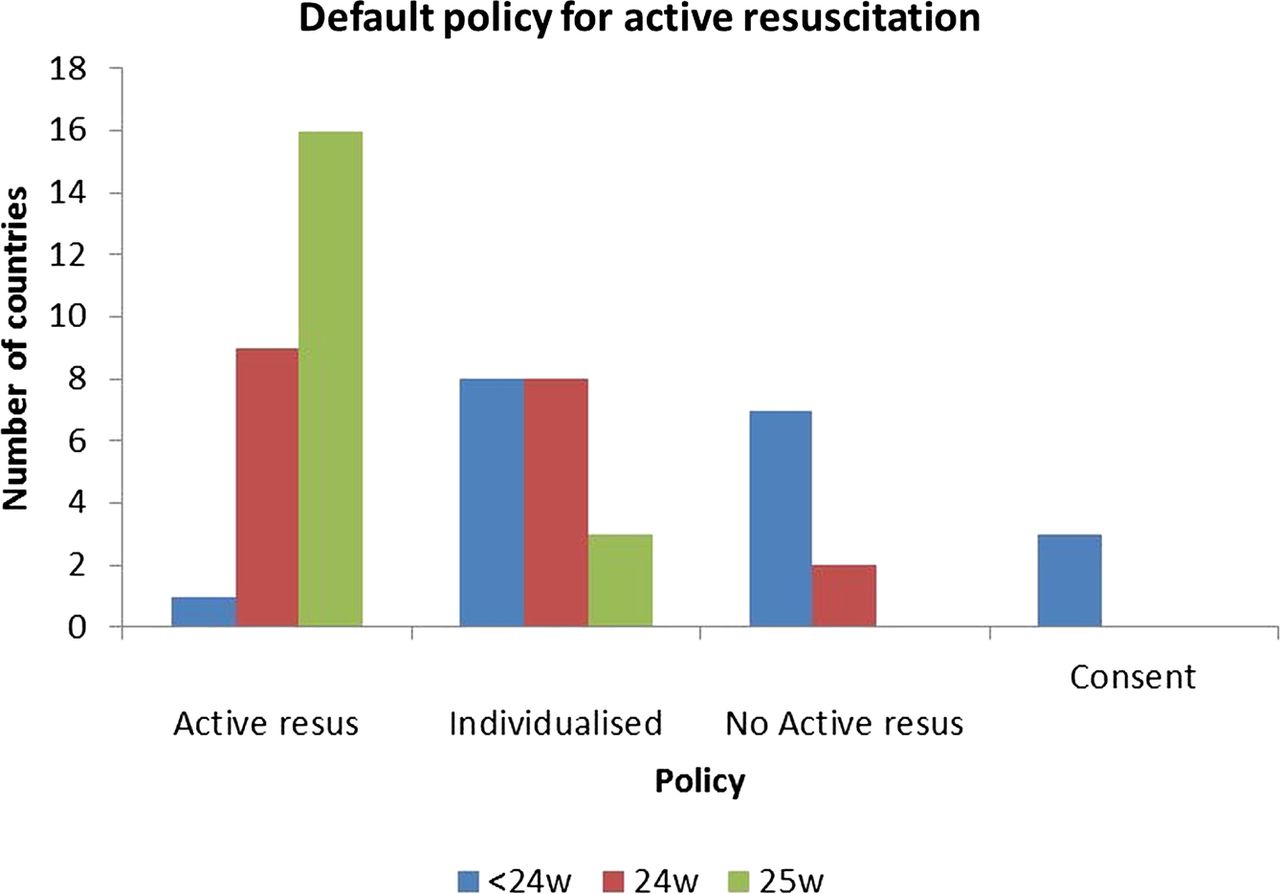
Responses were received from 19 of 28 Countries contacted and are collated in table 1. There did not appear to be any relationship between countries who responded and those who did not; countries representing different economic, religious and demographic status were among both categories respectively. Among the 19 responding countries, practice was most variable at less than 24 weeks of gestation: seven responses (37%) indicated that no active resuscitation would be undertaken and in three (16%) that parental permission was required to proceed. In contrast to 8 countries (42%) assessment was made on an individual basis and in one guideline all babies were to be offered active care. At 24 weeks of gestation 9 countries (47%) reported that resuscitation would be started, while in a further eight countries (42%) individual assessment of the infant's condition at birth would be used to guide action. Two countries (11%) reported minimal interventions at this point, for example no cardiac compressions or drugs would be used. At 25 weeks of gestation, resuscitation was common practice in 16 out of the 19 countries (84%) with individual assessment of the infant's condition reported in a further 3 (16%) (figure 1).
National guidelines of resuscitation at 22 to 25 weeks’ gestation reported in each country responding to the information request

{kind=link}
Summary of default action at birth between 22 and 25 weeks of gestation in 18 EU countries.
Most countries (17 of 19) indicated that they offered comfort or palliative care to babies who were not actively resuscitated after birth. For babies born at 23 weeks or less, parental inclusion in the decision-making process was reported by 12 (63%) respondents and in 3 countries consent or assent was required before undertaking active intervention. In contrast, when a divergence of views towards resuscitation occurred between the parents and the healthcare professionals, the ultimate decision was taken by the attending doctor in 16 (84%) countries, in two it was said to be a ‘team decision’, including parents and doctors, and in one the final arbiter was the High Court. No response indicated that parents were responsible for the ultimate decision. In only 3 (16%) countries parents or representative groups had been involved in the development of official guidance, in 13 (68%) parents had not been included and in 3 countries no official guideline was available.
Within the respondent countries there was no relationship between population, health expenditure or rates of preterm birth on whether or not active intervention was offered at 23 weeks or less.
Conclusions
The aim of this paper was to determine the extent to which there is a shared European consensus towards parental involvement in decision-making for extremely preterm infants. Through our exploration of national guidelines we found much variation in approaches to active intervention after birth across the EU, which appears to reflect local philosophy and practice rather than economic or demographic markers, individual variations in health expenditure or rates of preterm birth. This reflects work undertaken by Cuttini et al in 200016 who reported in their European survey of neonatologists individual decision-making practices that country appeared to be the strongest variable in predicting physician counselling practices. In all respondent countries care was offered for babies born at 25 weeks of gestation but below much variation was apparent. The approach to management of infants born at 23 weeks of gestation or less shows the most divergence from resuscitation to no resuscitation, indicating other potential influencing factors in the decision-making process than the outcomes of the infants themselves. There is equal variation in the involvement of parents in decisions but in essence a professional makes the final decision to intervene or not in the majority of situations. Similarly parents are only infrequently involved in the development of guidance as to how to manage this difficult area. Thus the country where a mother gives birth will highly influence the chance of her infant being resuscitated at less than 25 weeks’ gestation. The role of national guidelines in this situation is therefore of vital importance. The involvement of parents in this decision-making process also varies from informed, involved and consent bearers to an essentially passive role, emphasised by there being little evidence that parents are involved in the development of recommendations around their own involvement in decision-making in most settings. This directly questions commitment to the role of parents in this process. The juxtaposition between stated parental involvements in decision-making, when the healthcare team ultimately make the decision in the majority of countries surveyed, would also suggest an underlying belief in precedence of the decisions of the healthcare professionals over and above those of the parents.
What this study has achieved is to highlight the different approaches to decision-making in a variety of European countries, although further exploration of these findings outside of Europe would provide more contexts to the question of how decisions are made for extremely preterm infants on a global scale. Exploration is also required in light of the economic implications of the results. Although there is little evidence of variation by economic status, the cost of looking after babies at such low gestations is substantial. Markov modelling using data from the UK to determine total societal costs over the first 18 years after birth estimated the mean incremental cost per survivor born ≤28 weeks of gestation to be £94 740. The mean increment rises steeply within the extremely preterm population from £92 447 at 25 weeks, £169 928 at 24 weeks and £234 497 at 23 weeks of gestation.17 There are significant educational costs later in childhood that are often not considered in economic studies and up to 2/3 of teenage extremely preterm children will have special educational needs.8 The increasing survival of children at low gestations4 and an increasing willingness to admit babies for ongoing care places major pressure on scarce neonatal and paediatric resources available in countries of differing economic status.
The belief that parents should be actively involved in decision-making has led to a wealth of research around how to help parents understand the complex information which is presented to them antenatally and postnatally. Guillen and colleagues9 explored the use of a decision aid, developed with parents and physicians, to convey complex statistical outcome information during counselling of parents facing extremely premature delivery. The tool used pictorial cards to help convey information around outcomes including mortality and morbidity, exploring the effect upon parents who had experienced preterm birth and those who had not. Results showed that both sets of parents found the information useful and that the discussion initiated by the cards themselves was beneficial for the subjects. A recent Cochrane review confirms that people facing health choices or screening options who used decision aids were statistically better informed and less passive in decision-making than those who did not.18 However, we have not established whether the outcomes are affected by the decisions which the patients (or in this case parents) make. If a parent uses a hypothetical decision aid exploring risk of mortality and morbidity for their infant born at 24 weeks’ gestation and decides that they would like to withhold treatment, are we as neonatal healthcare professionals happy to accept that parents understand this risk and withhold treatment if we felt the infant would respond to treatment? Or are we more likely, as de Leeuw and colleagues14 found in their exploration of European physicians’ attitudes towards treatment choices for extremely preterm infants, to follow the wishes of parents ‘when they ask for treatment to be continued, rather than limited or withdrawn’ (p.614)?
The literature surrounding parental involvement in decision-making centres on the belief that all decisions are made in the best interest of the infant. What it does not question is the parent's ability to make a difficult decision when placed under extreme stress. A recent systematic review exploring the risk factors for the 1–2% of women who postnatally develop Post Traumatic Stress Disorder (PTSD) reported 3 predisposing factors including previous psychological dispositions, traumatising events in childbirth (including infant complications) and the perception of childbirth being traumatic.19 Further research is required to determine whether modifying the decision-making process around delivery has any impact on later psychological outcomes of PTSD in either parents. Psychological literature has begun to explore the relationship between the decision-making context and a person's ability to make a decision. A recent selective review concluded that an individual's decision-making capacity was impacted by the decision itself and by the external stress of the situation.20 Decisions made by parents within the delivery suite are arguably made under extreme distress. Compounding this factor is the complexity of the information required to make an informed decision about their infant, when research has clearly shown that the information needs of parents about neonatal treatment and outcomes are great.21 The expectation placed upon parents to make a logical decision at this point can therefore be questioned and may lead to decisions which do not ultimately reflect the best interests of the infant.
An understanding of the impact of the situation and the decision-making task raises the question of whether healthcare professionals should be assessing the decisional capacity of the parents to make such decisions. What must remain central to the decision at all times is the best interests of the infant for whom the decision is being made, and it is the duty of the healthcare professional to uphold these best interests. An appreciation of the parent's emotional capacity may result in decisions being upheld or overridden as the healthcare professionals deem appropriate for the infant and may therefore be an underlying reason of conflict in decision-making between parents and healthcare professionals. This highlights the importance of specifically designed tools as discussed by Guillen and colleagues9 to present complex information to parents to aid their stressful decision-making task in the already stressful situation. While more evidence regarding the impact on and support for parents making critical decisions is required, what is vital is that we include parents in developing the research and the recommendations at national and European levels around parental involvement in decision-making for their infants to ensure their position is not assumed. Furthermore, such engagement and evidence should help to shape our understanding of neonatal palliative care, and the two concepts need to be considered together to optimise the delivery of palliative care within this context.
The guidelines explored for this study suggest a nationalistic and paternalistic approach to the management of preterm birth; however, what is not known is how accurately these guidelines reflect reality at the cost side. Such emotional discussions are challenging for parents and healthcare professionals, and the amount of direction given to parents may vary from unit to unit throughout each country depending upon the individual neonatal teams involved. Previous research exploring decision-making throughout the Pacific Rim has identified that physician counselling practices are often shaped by cultural differences and local medical practices22; this echoes the findings of this study, along with those previously highlighted by Cuttini et al suggesting further exploration of individual country cultural factors require exploration to determine how they shape and reflect (if at all) national policies. A recent study undertaken in the south east of England exploring neonatologist decision-making practices during preterm birth highlights this point, as findings reported attitudes which were often in direct contrast with the national recommended practices.23 Some of the reported practices were also in direct conflict with maternity recommendations around resuscitation at extremely preterm gestations, indicating a potential for conflict in the delivery suite between healthcare professionals. Further research is required to determine how these difficult decisions are navigated in practice and in relation to national guidelines, and how precisely parents are affected by this cultural approach towards decision-making by healthcare professionals. This would be further enhanced through a more a more detailed understanding of infant outcomes following decision-making, including survival, to ensure guidelines are based upon appropriate evidence.
This study suggests that there is no shared European consensus for practice in this difficult area, creating a dilemma for parents and clinicians within the European community. Such a difference towards the treatment of infants born at the margins of prematurity and the involvement of their parents in difficult decision-making questions this ‘European citizenship’24 and raises the ethical debate over what is best practice. This question requires exploration from the European perspective to determine the impact of variations in treatments available in different countries, and also in relation to the ever emerging evidence documenting long term outcomes of preterm infants, to determine how policy is shaped by evidence. The European Foundation for the Care of Newborn Infants highlights this in the recent White Paper ‘Caring for Tomorrow’25 promoting collaboration between EU member states to improve standards of care across Europe. All countries should begin to take ownership of the outcomes of parents and follow these up routinely to determine whether active involvement versus informed involvement impacts upon psychological coping in parents, and thus whether parents are able to make informed decisions about their infants. Parental involvement at all stages of the discussion is vital to ensure that their opinions inform and shape the debate of who should have the decisional capacity to make exceptionally difficult decisions about extremely preterm infants in Europe.9
Acknowledgments
We are grateful to Helen Brewer and the European Critical Care Foundation for contacting individual perinatal societies. Neil Marlow receives part funding from the Department of Health's NIHR Biomedical Research Centre's funding scheme at UCLH/UCL. KG was part funded through an NIHR PDG award. The views and opinions expressed in this article do not necessarily reflect those of the DH/HIHR.
References
Footnotes
-
Contributors NM and JM conceived this study following a colloquium on ethical aspects of care at extremely low gestational ages held in Copenhagen, Denmark, in October 2010. KG collated the data and wrote the first draft. NM, JM and MK all contributed to the draft and have approved the final version of the manuscript. KG is the guarantor for the paper.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.