Article Text

Abstract
Aim: To determine the neurodevelopmental morbidity in the surviving twin after fetal or infant death of the co-twin.
Methods: Twin pregnancies with an antepartum or infant death delivered between 1981 and 1992 were identified from the Northern Perinatal Mortality Survey. Information on the neurodevelopmental morbidity of infant survivors of a deceased co-twin was obtained by a questionnaire sent to the community paediatrician or general practitioner.
Results: A total of 111 children who survived infancy after the fetal death of the co-twin (group 1) and 142 from liveborn twin pairs in which one twin died in infancy (group 2) were traced. Responses were received from 97 (87%) and 130 (92%) respectively. In group 1, the cerebral palsy prevalence was 93 (95% confidence interval (CI) 43 to 169) per 1000 infant survivors; it was more common in like-sex pairs (8/70) with a prevalence of 114 (95% CI 51 to 213) compared with 45 (95% CI 1 to 228) per 1000 infant survivors in unlike-sex pairs (1/22). The overall prevalence of neurodevelopmental morbidity (including developmental delay) was 175 (95% CI 106 to 266) per 1000. In group 2, the cerebral palsy prevalence was 154 (95% CI 84 to 223) per 1000 infant survivors in like-sex (16/104) and 77 (95% CI 9 to 251) in unlike-sex (2/26) survivors; the overall prevalence of neurodevelopmental morbidity was 246 (95% CI 172 to 320) per 1000.
Conclusions: The risk of cerebral palsy is increased in the surviving twin after a fetal or infant co-twin death compared with the general twin population. Like-sex twins are at greater risk than unlike-sex. The probable cause, in addition to the consequences of prematurity, is twin-twin transfusion problems associated with monochorionicity.
- cerebral palsy
- twins
- twin-twin transfusion
- gestational age
- PMS, Northern Perinatal Mortality Survey
- CI, confidence interval
Statistics from Altmetric.com
Twins are at a higher risk than singletons, not only for fetal and infant mortality, but also neurological morbidity. The prevalence of cerebral palsy ranges from 7–12 per 1000 infant survivors in twins compared with 1–2 in singletons.1–5 The higher relative risk of cerebral palsy for twins is not entirely attributable to the overrepresentation of low birthweight and preterm infants, as the risk is also higher for normal birthweight twins than for comparable singletons.2,5,6
Case reports and hospital based case series have found that the antenatal death of a twin is associated with severe morbidity in the co-twin.7–14 Over the last decade, population based studies have also shown that, among twin pregnancies with an antenatal loss of one twin, the surviving twin has an increased rate of cerebral palsy compared with twin pregnancies in which both twins survived.1,2,6,15,16 In the case reports it has been found that monochorionic twins are at particularly high risk.12,17–26 However, there is a lack of population based follow up studies of the surviving twin whose co-twin died in utero that include data on placentation and gestational age.
The aim of this population based follow up study was to determine the neurodevelopmental morbidity for the surviving twin of a co-twin fetal or infant death.
METHODS
Study sample
All twin pregnancies delivering between 1981 and 1992 with an antepartum or infant death were identified from the population based Northern Perinatal Mortality Survey (PMS). Since its inception in 1981, the PMS has collected data on all late fetal losses, stillbirths, and infant deaths occurring to mothers resident in the former Northern Region of England.27,28 Notifications of death are made by multiple sources. The years 1981–1992 were selected to complement a national study of the consequences of intrauterine death in twin pregnancies for the survivor, which covered the years 1993–1995.16
Infant survivors (children who survived beyond the first year of life) from twin pairs in which there has been a fetal death (group 1), and infant survivors from liveborn twin pairs in which one infant died in infancy (group 2), comprised two study groups.
Definitions
Fetal death was defined as a spontaneous (identifiable) intrauterine death which was delivered after 28 completed weeks gestation (the legal limit of fetal viability in the United Kingdom during the study period). Infant death was defined as a live birth that died within the first 365 days of life. The definition of cerebral palsy was that proposed by the members of the Little Club29 and updated by Bax.30 Postneonatally acquired cases were excluded. “Other cerebral impairment” is used for children with evidence of cerebral impairment other than cerebral palsy—for example, learning disability, epilepsy, sensory neural hearing loss, general developmental delay.
Ethical approval
Ethical approval was obtained from the multicentre research ethics committee and from all the local research ethics committees within the Northern Region.
Follow up
Infant survivors from both study groups were cross checked with a register of cerebral palsy, comprising children born in three health districts of the Northern Region (Newcastle, Northumberland, and North Tyneside) before 1991.31 For children born in 1991–1992, infant survivors were cross validated against the North of England Collaborative Cerebral Palsy Survey, which covers all births in the Northern Region from 1991. Using death notifications, deaths up to age 16 years were identified.
A questionnaire on the long term (minimum 7 years of age) disability was sent to the community paediatricians except for those children who were known to have cerebral palsy from the regional register or who had died in childhood. The community paediatricians identified children with moderate and severe disability using the local register of children with disability or the special needs register. For those districts where there was no special needs register or no clear information on the health status of the children during their first seven years of life, the same questionnaire was sent to the child's general practitioner. If the current registration with a general practitioner was unavailable from the local health authority because the family had moved, or the name of the child had been changed, the contact details of the general practitioner were obtained from the Office for National Statistics.
Questionnaire
The questionnaire comprised five questions: is the child known to have any disability—for example, hearing, vision, physical? Is the child known to have cerebral palsy—for example, diplegia, hemiplegia, quadriplegia, dyskinetic, mixed? Is the child known to have congenital abnormality—for example, neural tube defect, cleft palate, chromosomal abnormality? Is the child known to have developmental delay? Are there any other relevant observations? If the answer was positive to any of the questions, the general practitioner was asked to specify further details.
Chorionicity
Unlike-sex twins were assumed to be dizygotic and therefore dichorionic. Like-sex twins may be dizygotic (always dichorionic) or monozygotic (monochorionic or dichorionic). Data on chorionicity for like-sex twin pregnancies, based on clinical or pathological examination of placenta or evidence of twin-twin transfusion syndrome (polyhydramnios/oligohydramnios, birthweight discordancy, intertwin haemoglobin discrepancy, or anaemic/plethoric co-twins), were obtained from the PMS or hospital records.
Statistical analysis
Descriptive analysis was carried out using the Statistical Package for the Social Sciences (SPSS for Windows).32 Cerebral palsy prevalence among twin survivors was calculated per 1000 infant survivors. Cerebral palsy prevalence among singletons in North East England in 1985–1989 was calculated per 1000 neonatal survivors (P Drummond, personal communication). Confidence intervals were calculated using the Confidence Interval Analysis package.33 χ2 tests were used to test differences in proportions. Statistical significance was accepted at the p < 0.05 level.
RESULTS
Mortality in the liveborn co-twin of a fetal or infant death
In 1981–1992, there were approximately 9520 twin births (4760 pregnancies) (Office for National Statistics data. As the number of twin births for 1981 was unavailable, the number has been estimated assuming the same number of twin births in 1981 as in 1982.). In 34 pregnancies, both twins died in utero; in 130, one twin was a fetal death and the co-twin a live birth, and 11 of these live births died in infancy. Table 1 shows the certified causes of death of both the fetus and the liveborn infant in these 11 twin pairs. The majority (9/11) had monochorionic placentation (six had clinical evidence of twin-twin-transfusion syndrome, in two the fetal death was an acardiac twin, and in one there was histological evidence of monochorionicity).
Causes of death among live births whose co-twin was a fetal or infant death
There were 119 co-twins of a fetal death who survived infancy; these comprised group 1. One of these live births who survived infancy in whom the cause of death was certified as cerebral palsy, died aged 11 years (table 1).
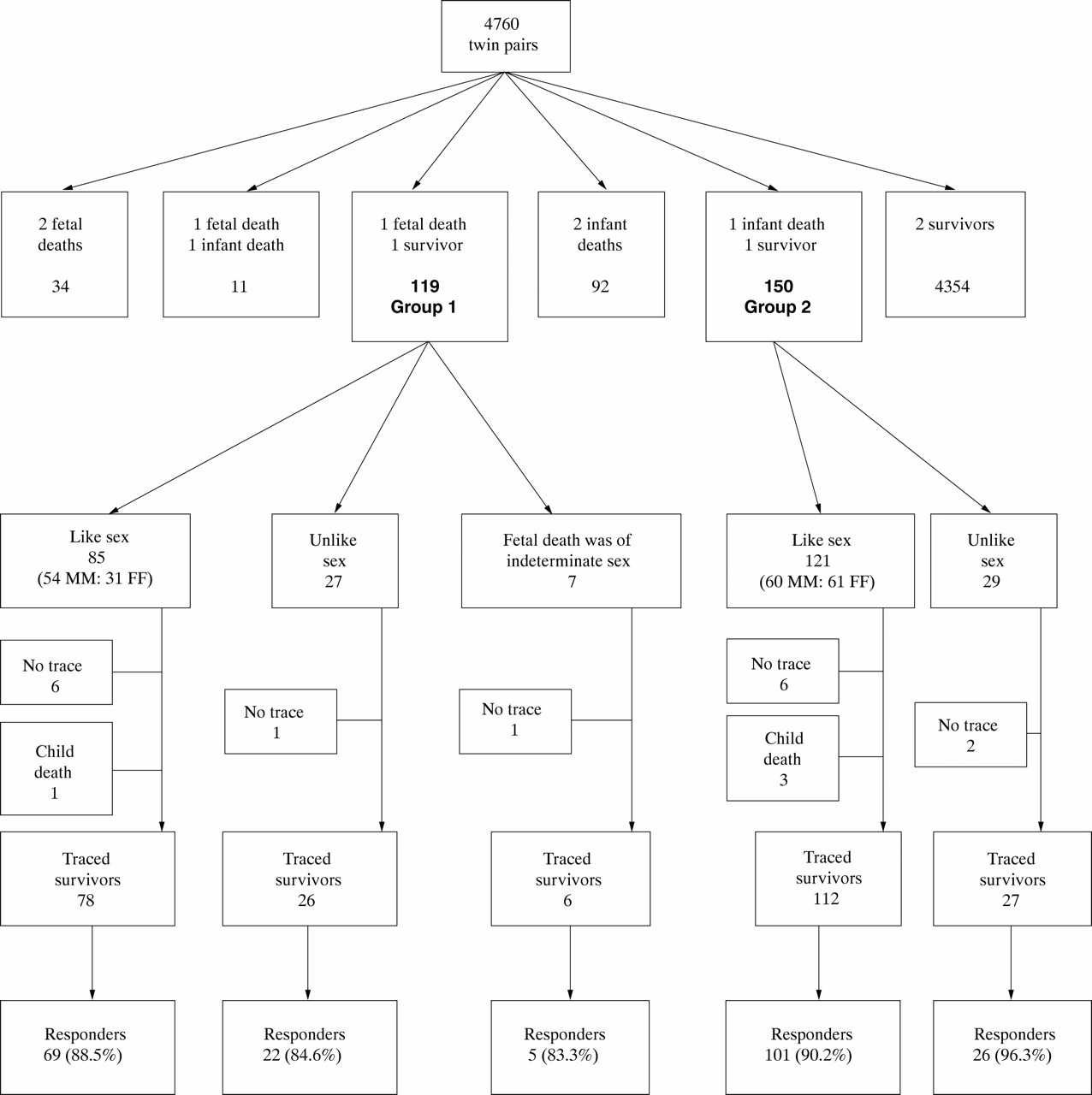
In 92 pregnancies both twins died in infancy. In 150 pregnancies, one twin died in infancy and the co-twin survived. These comprised group 2; of the 150 infant survivors, three died in childhood, one of whom had cerebral palsy as the certified cause of death (table 1). Figure 1 shows the derivation of the study sample.
{kind=link}
Number of twin pairs with different outcome born in 1981–1992, infant survivors of a co-twin fetal death (group 1) and a co-twin infant death (group 2), and the response rate for the survivors beyond 7 years of age.
The following analysis considers group 1 and group 2 infant survivors only.
Response rates
Figure 1 shows the response rates for the surviving co-twins of like-sex and unlike-sex pairs in groups 1 and 2. In seven cases, the sex of the fetal death was indeterminate, and there were eight children in each of groups 1 and 2 who could not be followed up because they were adopted, had migrated, or were not registered with a general practitioner. Non-response arose from the refusal of general practitioners to seek parental permission or the parents refusing consent to release information on the health status of their child.
Group 1: infant survivors of a co-twin fetal death
There were nine cerebral palsy cases out of the 97 (96 responders and one child death) infant survivors, a cerebral palsy prevalence of 93 (95% confidence (CI) 43 to 169) per 1000 infant survivors. Eight of the children with cerebral palsy were from 70 like-sex pairs, a prevalence of 114 (95% CI 51 to 213) per 1000 infant survivors. There was one case of cerebral palsy among 22 unlike-sex pairs, a cerebral palsy prevalence of 45 (95% CI 1 to 228) per 1000 infant survivors. Table 2 shows pregnancy and birth details for like-sex and unlike-sex fetal deaths and the surviving co-twins with cerebral palsy. It is worth noting that in the single case of cerebral palsy among unlike-sex twins, the twin who died in utero weighed only 500 g, and the death certificate specified that the fetus was severely macerated. In such circumstances, it is possible that the sex of the fetus was incorrectly assigned. In like-sex twins, placentation was predominantly monochorionic (at least five of the eight cases).
Cerebral palsy in the surviving twin of like-sex and unlike-sex fetal death co-twin (group 1)
In addition to those children with cerebral palsy, eight of the 97 survivors had evidence of other cerebral impairment (table 3). Six were from like-sex pairs, a prevalence of 86 (95% CI 32 to 177) per 1000 infant survivors, and two from unlike-sex pairs, a prevalence of 91 (95% CI 11 to 292) per 1000 survivors.
Other cerebral impairment in the surviving twin of like-sex and unlike-sex fetal death co-twin (group 1)
Combining the data in tables 2 and 3, the total cerebral impairment prevalence is 175 (95% CI 106 to 266) per 1000 infant survivors: 200 (95% CI 114 to 313) for like-sex and 136 (95% CI 29 to 349) for unlike-sex survivors.
Group 2: infant survivors of a co-twin infant death
There were 18 cerebral palsy cases among the 130 (127 responders and three child deaths) group 2 infant survivors, a cerebral palsy prevalence of 138 (95% CI 79 to 198) per 1000 infant survivors: 154 (95% CI 84 to 223) in like-sex (16/104) and 77 (95% CI 9 to 251) in unlike-sex (2/26) infant survivors (table 4).
Cerebral palsy in the surviving twin of like-sex and unlike-sex co-twin who died in infancy (group 2)
In addition to those with cerebral palsy, there were 14 children with evidence of other cerebral impairment; 13 were from like-sex pairs, a prevalence of 125 (95% CI 61 to 189) per 1000 infant survivors, and one from unlike-sex pairs, a prevalence of 38 (95% CI 1 to 196) (table 5).
Other cerebral impairment in the surviving twin of like-sex and unlike-sex co-twin who died in infancy (group 2)
Combining the data in tables 4 and 5, the total cerebral impairment prevalence is 246 (95% CI 172 to 320) per 1000 infant survivors: 279 (95% CI 193 to 365) for like-sex and 115 (95% CI 24 to 302) for unlike-sex survivors.
Gestational age specific cerebral palsy rates
Table 6 shows the gestational age specific cerebral palsy rates for like-sex and unlike-sex survivors. Group 2 survivors, compared with group 1, were more likely to be born very preterm (41% v 12% before 32 weeks of gestation). In both groups, gestational age specific cerebral palsy rates in the survivors were considerably higher than those in singletons. Differences in gestational age specific cerebral palsy rates between group 1 and group 2 survivors in corresponding gestational age groups were not statistically significant, partly because of the small numbers.
Gestational age specific cerebral palsy (CP) prevalence rates in surviving co-twin of a fetal (group 1) or infant (group 2) death per 1000 infant survivors
DISCUSSION
This population based regional study, following up twins born during 1981–1992, complements a national study of the consequences for the surviving twin of fetal or infant death of the co-twin born between 1993 and 1995.16,34 Although smaller than the national study, it has a number of advantages. Firstly, recording the sex of a fetal death is likely to be more accurate because it is based on the information derived from the hospital notes and reports of the postmortem examination. In the national birth registration system, there are problems in coding of the sex of a fetal death, especially if it was a fetus papyraceus.35 If the sex of a fetus papyraceus was indeterminate, it was always coded as male in the national statistics; furthermore, the parents may be allowed to decide which sex is recorded on the death certificate. Secondly, information on chorionicity was available in this study for most like-sex fetal death/survivor pairs (group 1) with cerebral palsy. Thirdly, there was a better response rate and a longer period of follow up. The longer follow up increased the likelihood of learning disability in the absence of motor disability being recognised.
The response rate was high, 87% for group 1 and 92% for group 2; nevertheless, non-response bias should be considered. Assuming that none of the untraced children and non-responders had cerebral palsy or other cerebral impairment, the disability rate would have been marginally lower at 143 per 1000 for group 1 and 213 per 1000 for group 2. These prevalences remain extremely high when compared with the generality of cerebral palsy prevalence in twins.3
We were unable to collect complete information on chorionicity, as there was no record of pathological examination of the placenta in many cases of like-sex twins in group 2.
Ideally, the prevalence of serious neurological morbidity among infant survivors of a fetal death should be compared with morbidity prevalence in liveborn twin pairs when both twins survived infancy. This was impractical as it would have entailed following up over 9000 twins born in 1981–1992.
The surviving twin of a co-twin fetal death (group 1) was found to be at high risk of either dying in infancy or having serious neurodevelopmental morbidity. The overall prevalence of serious neurodevelopmental morbidity was 175 per 1000 infant survivors. The cerebral palsy prevalence in like-sex twins was over twice that in unlike-sex twins, although this difference was not statistically significant. In the light of other reports, this is probably a consequence of vascular anastomoses that occur with monochorionic placentation.8,19,21,24–26 Twin-twin transfusion syndrome is limited to monochorionic twins, and the cerebral impairment probably has a haemodynamic cause. Indeed, the placentation was predominantly monochorionic in the like-sex group of cerebral palsy cases, providing further evidence that twin-twin transfusion problems are the underlying cause of the cerebral damage in this group.
The cerebral palsy rate in survivors of a co-twin fetal death in this study is in accordance with the findings of previously published population based studies,1–3,6,16 except one Swedish follow up study of a similar cohort of twin survivors after a fetal death of a co-twin.15 In that study (50% were lost to follow up), the disability rate at the age of 8 years was 46 per 1000 (3 of 65). This rate was about half of that found in this and other referred studies. The disparity in the disability rates may be due to differences in methodology (definitions, exclusions, denominators, etc).
In group 2 survivors, the proportion of infants born before 32 weeks gestation was disproportionately high. Three possible pathways leading to cerebral impairment in very preterm infants have been proposed.36 Prematurity per se may predispose to hypoxic-ischaemic and haemorrhagic cerebral damage; an antenatal factor may cause both the cerebral impairment and lead to preterm delivery; an antenatal factor may cause the cerebral impairment that predisposes to preterm delivery. When both twins are live births and one dies in infancy (group 2), the cause of death is prematurity in the vast majority. The surviving co-twin in each case therefore is liable to the complications of prematurity. Very preterm birth—that is, birth before 32 completed weeks of gestation, as defined by the WHO37—is considered the strongest predictor of later cerebral palsy, with a higher risk associated with a lower gestational age at delivery.36 A prospective population based study of extremely preterm infants (22–25 completed weeks of gestation) in the United Kingdom and Ireland showed that 49% of the survivors had disability at 30 months of corrected age, with nearly half of them being severely disabled.38 Our study found a high cerebral palsy prevalence in group 2 infant survivors. Among disabled survivors in this group, the proportion of those born before 32 weeks gestation was 83% (15/18). In this group, prematurity is likely to be the leading factor in the development of cerebral palsy. The cerebral palsy and other cerebral impairment attributable to the prematurity per se, the first pathway, will account for some of the neurological morbidity in both like-sex and unlike-sex twins. However, in addition to the consequences of prematurity, there is an excess morbidity in like-sex twins. In such cases, the two other pathways mentioned above, with twin-twin transfusion as an antenatal factor, may contribute to both the cerebral impairment and the preterm delivery.
Given the importance of chorionicity, both for the management of twin pregnancies and research into the causes of cerebral palsy, it needs to be emphasised again that the accurate antenatal determination of chorionicity with postnatal confirmation is crucial.
Only about 10% of cases of cerebral palsy are of intrapartum origin,39 and research into the causes of cerebral palsy needs to focus on antepartum events.40 In multiple pregnancies, the effect of the timing of an intrauterine death on the outcome and prognosis for the surviving co-twin is still controversial. The current study did not address the effects of fetal loss in the first trimester of pregnancy (the vanishing twin), which would in theory have an adverse consequence for the survivor. Studies addressing this have so far produced conflicting evidence,13,18,41,42 and a prospective study of survivors from twin pregnancies with a confirmed co-twin loss in the first trimester of pregnancy should determine the significance of this event for the surviving co-twin.
Acknowledgments
We thank the district convenors of the North of England Collaborative Cerebral Palsy Survey, general practitioners, health authority medical records personnel, and staff at the Office for National Statistics who enabled the study to be carried out. We are also grateful to those parents who gave their consent for information on the health status of their child to be released. The dedication of Mrs Marjorie Renwick and staff at the Regional Maternity Surveys Office in maintaining the PMS was crucial to the study. We thank the PMS Steering Group for access to the PMS data, and Dr Paula Drummond for providing the data on gestational age specific cerebral palsy rates in singletons. SG is funded by the Newcastle University Hospitals Special Trustees.