Article Text

Statistics from Altmetric.com
- CT, computed tomography
- fMRI, functional MR imaging
- HI, hypoxia-ischaemia
- MR, magnetic resonance
- NE, neonatal encephalopathy
- NMR, nuclear magnetic resonance
- PVL, periventricular leucomalacia
- US, ultrasonography
- WMD, white matter damage
Magnetic resonance imaging and spectroscopy techniques have huge medical and scientific potential in neonatal brain imaging
The magnetic resonance (MR) phenomenon was first described in 19461,2 but it was not until 1981 that the first transverse image through the human head was reported.3 In the last 20 years, MR technology has revolutionised medical and scientific neuroimaging, providing the richest source of information about the living brain available from any imaging technology and without the use of ionising radiation. MR techniques most commonly used in the neonate have been conventional MR imaging and 31P and 1H MR spectroscopy. MR imaging has allowed the observation of brain development and response to perinatal brain injury in vivo with an unprecedented sensitivity for assessment of changes in grey and white matter and an ability to differentiate unmyelinated from myelinated white matter. MR spectroscopy has provided a metabolic fingerprint of the brain during normal development and after perinatal brain injury (fig 1). Conventional MR imaging and MR spectroscopy, however, are only part of an array of methods that comprise the MR diagnostic armamentarium, which includes diffusion weighted MR imaging, diffusion tensor imaging, MR angiography, functional MR imaging (fMRI), magnetisation transfer imaging, and chemical shift imaging. These newer techniques have huge medical and scientific potential.

(A) Representative T2 weighted magnetic resonance (MR) images, (B) 1H MR spectra, and (C) 31P MR spectra from healthy infants at 30 weeks gestation, term, 6 months, and 1 year of age. (A) The MR images show an increase in volume, surface area, and sulcation of cerebral cortex and in volume and microstructural organisation of cerebral white matter with development. (B) The series of 1H MR spectra show a steady increase in N-acetyl aspartate (NAA; a marker of neuronal and axonal density and viability) and a decrease in brain lactate with maturation. (C) The series of 31P MR spectra show changing ratios of brain phospholipids and increasing energy state with maturation. PME, Phosphomonoesters; Pi, inorganic phosphate; PDE, phosphodiesters; PCr, phosphocreatine; ATP, adenosine triphosphate; Cho, choline; Cr, creatine; lac, lactate.
RATIONALE FOR THE USE OF MR IN THE NEONATAL BRAIN
In the last 20 years, we have seen major advances in obstetric and neonatal intensive care such as the introduction of new treatments and evolving modes of ventilatory support. Despite these advances, perinatal hypoxia-ischaemia (HI) is experienced by about 4/1000 live term births, and disability rates among very low birthweight (birth weight < 1500 g) infants remain high, with 5–15% showing major spastic abnormalities and an additional 25–50% or more having deficits in cognition and behaviour.4–6 Neuroimaging is needed in at risk infants, as clinical evaluation may not provide adequate diagnostic or prognostic information and has two principal functions: (a) early diagnosis of brain injury so that appropriate medical management can be provided; (b) detection of lesions associated with long term neurodevelopmental disability. Currently, cranial ultrasonography (US), computed tomography (CT), and MR imaging are the most widely used techniques. MR imaging has a unique power as a diagnostic neuroimaging tool in neonatology.
MR IMAGING IN NEONATOLOGY: BEST PRACTICE RECOMMENDATIONS
Neonatal encephalopathy (NE)
In the encephalopathic term infant, a conventional MR image provides the most specific means to predict the pattern of neuromotor outcome. The pattern of tissue injury is related to the type and severity of insult, and a close correlation exists between the pattern of abnormality on MR images and neurodevelopmental outcome.7,8 The most predictive finding on MR for abnormal outcome is a change in the signal intensity of the posterior limb of the internal capsule,8 and detailed descriptions of precise MR findings and their relation to later neurological outcome are available.9 In particular, MR imaging has refined the differentiation between global and focal injury in which the outcome is significantly different (fig 2). In addition, MR imaging enables the diagnosis of a range of cerebral developmental abnormalities, which may be confused with acute perinatal HI. MR imaging and spectroscopy also aid in the diagnosis of congenital metabolic disorders, which may present with acute NE. MR is particularly good at visualising posterior fossa structures and diagnosing cerebellar malformations compared with US.10

T1 weighted magnetic resonance images of (A) focal injury in an infant with Sarnat stage II neonatal encephalopathy (NE) aged 11 days and (B) global injury in an infant with Sarnat stage III NE aged 12 days. (A) Focal high signal intensity lesions are visible in the lentiform nuclei and thalami, and there is loss of the normal high signal intensity from myelin in the posterior limb of the internal capsule. (B) There are extensive high signal intensity lesions in the lentiform nuclei and thalami, loss of the normal high signal intensity from myelin in the posterior limb of the internal capsule, and abnormal low signal intensity in the white matter with loss of the normal grey/white matter differentiation.
US has the advantage of being mobile and easily used on the neonatal unit. It is therefore ideal for sequential scans to follow the evolution of brain lesions, defining normal cerebral anatomy, detecting large established basal ganglia lesions (from 1–3 days after birth),11 abnormal cerebral blood flow velocity (from 24 hours from birth),12 and major intracerebral haemorrhage. However, US has very limited accuracy in defining the site and extent of ischaemic tissue injury after perinatal HI. CT involves exposure to a considerable amount of radiation, making it unsuitable for serial scans. However, it is an effective technique for the detection of intracranial haemorrhage and may detect some basal ganglia and thalamic lesions.
In our opinion, there is now sufficient evidence to recommend that a conventional MR image should be performed to provide precise predictive information in all term infants with moderate or severe NE. A similar recommendation has been made recently by the American Academy of Neurology quality standards committee and endorsed by the American Academy of Pediatrics in 2002.13 The optimal timing appears to be toward the end of the first week after birth (and certainly within the neonatal period before atrophy becomes obvious). Very early scans performed in the first 24 hours can be misleading, as they may appear almost normal even when there is severe HI injury.
It is unlikely that MR will have a role in screening infants for entry into trials of neuroprotective interventions such as hypothermia. As the therapeutic window for neuroprotective treatments appears to be less than six hours, a conventional MR image will not give prognostic information within this time frame before the onset of the cascade of irreversible injury. So far, diffusion weighted imaging has not been proven to be effective as a prognostic tool in NE.14 This is surprising, as diffusion weighted imaging in the adult brain15 and experimental models16 of stroke has revolutionised the possibility of early diagnosis and intervention, often revealing image abnormalities on water diffusion maps well before CT or conventional MR. 31P and 1H MR spectroscopy (giving quantitative information on brain energetics, intracellular pH (pHi) and lactate) can give early prognostic information on brain injury severity. However, for logistical reasons it is almost impossible to transport sick infants with NE to an MR system and perform an MR study within six hours of birth. The optimal method for selecting infants for neuroprotective trials of hypothermia is amplitude integrated electroencephalography (cerebral function monitoring), which has a high predictive value for neurological impairment in most,17 but not all,18 situations when performed as early as three hours after birth.
Neonatal cerebral infarction
As a consequence of the wider availability of MR brain imaging in the newborn infant, neonatal cerebral infarction has become increasingly recognised; cerebral arterial infarction occurs in about 1 in 4000 term infants who typically do not show signs of birth asphyxia, but present with seizures in the first few hours or days of life. The cause is usually unknown, although there is an association with inherited or acquired prothrombotic disorders.19 Early MR imaging is more sensitive than US in the detection of arterial infarcts,20 and diffusion weighted imaging is valuable in early grading of the lesion.21 MR imaging has allowed a more accurate prognosis to be assigned to infants with arterial infarction compared with US and CT. Generally only about 20% of infants develop a hemiplegia after neonatal cerebral arterial infarction; the likelihood of motor impairment depends on the overall extent of injury and involvement of cerebral hemispheres, basal ganglia, and posterior limb of the internal capsule and the background activity on neonatal electroencephalography.22 Wherever possible, MR imaging and cerebral function monitoring should become a standard investigation in infants with early neonatal seizures.
Preterm brain injury
Epidemiological studies have confirmed that the main correlate of major long term neurological deficits in the preterm infant is periventricular white matter damage (WMD).23 WMD encompasses at least three main groups: cystic periventricular leucomalacia (PVL), haemorrhagic parenchymal infarction, and diffuse WMD. US is the most appropriate safe and accessible bedside tool for assessing brain structure, intraventricular haemorrhage, germinal layer haemorrhage, haemorrhagic parenchymal infarction, cystic PVL, and ventriculomegaly. Sequential scans are now standard in the neonatal unit for monitoring evolving brain injury. Such frequent sequential scans are necessary to diagnose cystic PVL; an area of echodensity appears 24–48 hours after a known insult, but cysts are not visible on US for a further two to four weeks.
US has limitations in the diagnosis of subtle preterm WMD. Abnormal echogenicity on US is not lesion specific and, on the basis of pathological correlation studies, US has poor sensitivity and specificity in detecting subtle or diffuse brain injury.24 Several studies have suggested that conventional MR imaging is more sensitive for detecting WMD than US both early after birth25 and at a corrected age of term,26 but as yet there has been no correlation with neurodevelopmental outcome. MR imaging may be helpful in the early diagnosis of PVL: diffusion weighted imaging detected PVL in a 30 week gestation infant at a time when both US and conventional MR imaging were normal.27
The American Academy of Neurology quality standards committee have suggested that, so far, there is insufficient evidence for routine MR imaging of all preterm infants with WMD on US.13 Some European studies, however, suggest that a conventional MR image at a corrected age of term can give useful prognostic information. In particular, when there is unilateral parenchymal involvement from PVL or haemorrhagic parenchymal infarction, the likelihood of subsequent hemiplegia depends on whether there is asymmetrical myelination in the posterior limb of the internal capsule on conventional MR imaging.28,29
ROLE OF MR IN NEONATAL NETWORKS
In view of its growing clinical importance, it is arguable that neonatal networks should be planned to ensure that MR imaging is available for all infants who will benefit from it. However, universal access to high quality imaging will have enormous cost, resource, and planning implications for neonatal care in the United Kingdom. It is important that the limitations and logistical problems of MR techniques are carefully considered. MR is not and will never be a bedside procedure. Because of the potential attraction of ferromagnetic objects toward the magnet core, all equipment and implants must be non-magnetic. Infants must be stable enough to tolerate transfer to the MR facility, and require physiological monitoring during an MR study with at least one experienced neonatologist in attendance. Noise levels may be unacceptably high, and noise reduction devices such as earmuffs and/or ear plugs may be required. The quality of MR data is sensitive to movement, and sedation is often necessary. In our experience, a milk feed and 30–50 mg/kg chloral hydrate before the study is safe and effective. MR compatible ventilators and incubators are now commercially available; with careful consideration of the infant’s wellbeing, many groups have successfully performed MR studies in infants receiving full intensive care.30,31
Access to a suitable MR facility is just the start; standard sequences for the adult brain are not appropriate for imaging infants and sequences need to be adapted for neonatal brain imaging to accommodate the changes in T1 and T2 as physiological myelination and growth take place. MR imaging must become more infant friendly and imaging strategies developed to provide maximum information in minimum time. MR techniques must be standardised in terms of sequence parameter, region of brain evaluated, timing of evaluation, and reference to robust control data. Improved magnet technology is needed that will allow easy placement of MR systems adjacent to neonatal intensive care units. MR scans need to be interpreted by a radiologist who has experience of neonatal brain imaging because of unusual and idiosyncratic signal changes that occur with normal maturation and growth. Results of imaging studies must be available immediately for viewing by all involved specialties. With the advent of filmless radiology, it may be possible to distribute MR images throughout a network or between network centres using internet technology such as Digital Imaging and Communications in Medicine (DICOM) and Picture Archiving and Communication Systems (PACS).32 DICOM and PACS applications have recently become commercially available. Combined with appropriate software, these applications will allow images to be accessed through the internet and MR images reported from afar.
MR RESEARCH: PAST, PRESENT, AND FUTURE DIRECTIONS
MR has an increasingly important role in research. As we aim for the possibility of perinatal brain repair, MR will be able to improve our understanding of the response of the developing brain to injury, aid the development of new neuroprotective strategies, and monitor and assess intervention and prognosis. MR research is at the crossroads between medicine, physics, chemistry, and computer science; groups with strong interdisciplinary relations will be essential to take this goal forward.
MR spectroscopy and chemical shift imaging
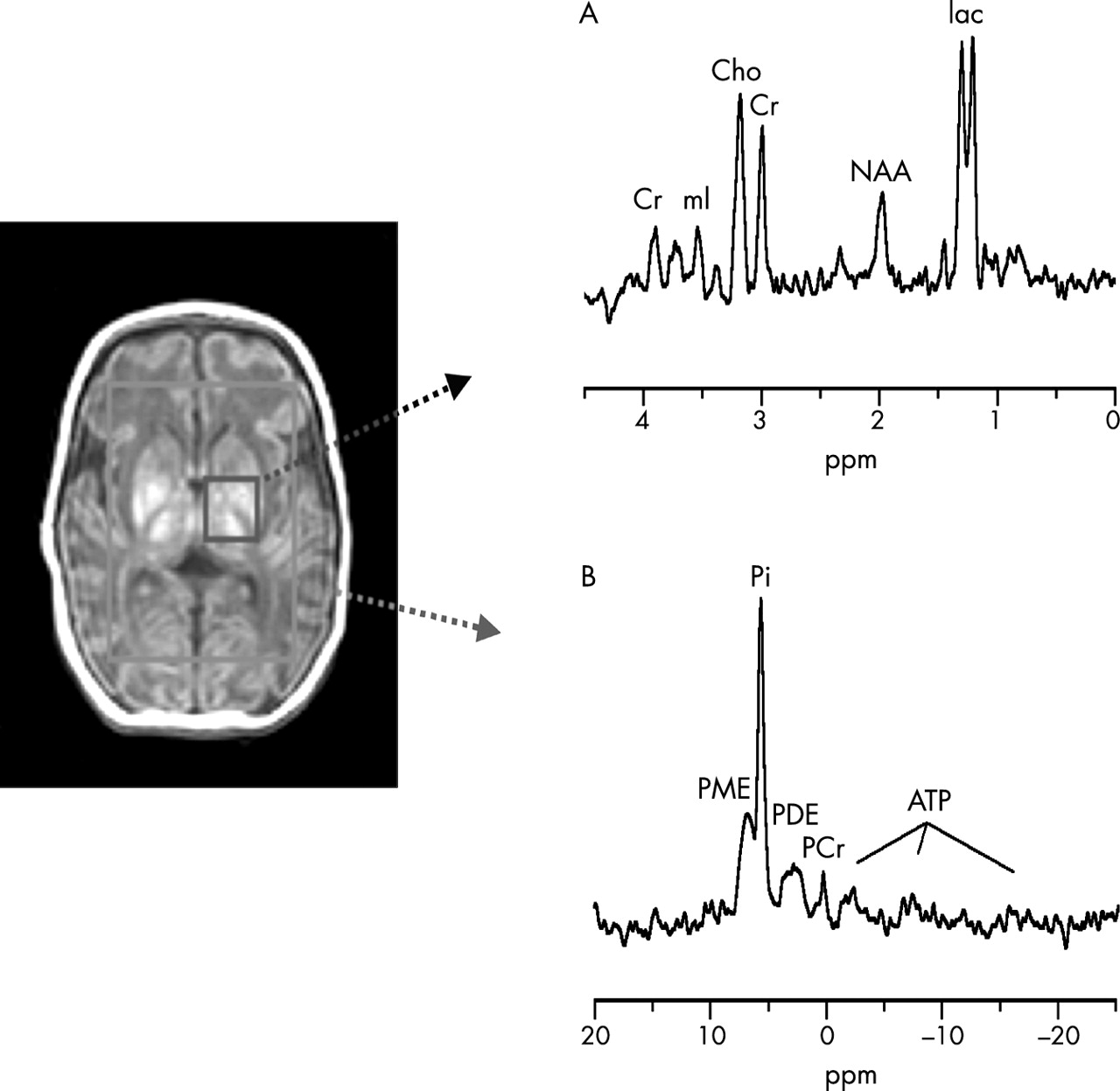
MR spectroscopy can provide early supplementary prognostic information in NE (fig 3) and aids diagnosis of metabolic disorders. However, MR systems capable of multinuclear MR spectroscopy are usually present only in research settings where its main role is investigating fundamental mechanisms of injury. Only through such detailed understanding of mechanism will advances in the care and treatment of the neonatal brain be possible. In the 1980s, experimental studies using 31P and 1H MR spectroscopy showed a biphasic pattern of energy failure after perinatal HI.33,34 This remarkable finding was the cornerstone behind the realisation that neuroprotective strategies may interrupt the cascade of irreversible injury if administered within hours of a perinatal insult and was an important catalyst in the development of current hypothermia trials.

(A) 1H MR spectrum from left basal ganglia showing appreciably raised lactate and reduced N-acetyl aspartate (NAA). (B) 31P MR spectrum from the whole brain showing severe secondary energy failure with phosphocreatine (PCr) and ATP depletion and increased inorganic phosphate (Pi). The brain pHi was alkaline (7.18). PME, Phosphomonoesters; PDE, phosphodiesters; Cho, choline; Cr, creatine; mI, myo-inositol; lac, lactate.
More recently MR spectroscopy has shown two further important concepts. Firstly, abnormal brain metabolism can persist for months to years in infants with a severe outcome after NE. This may indicate continuing cell death, which may be amenable to intervention for some considerable time after the insult.35 Secondly, brain pHi becomes alkaline after perinatal HI; in vitro studies show that such intracellular alkalosis is detrimental to cell survival after HI.36 This information may help to define optimal resuscitation techniques after perinatal HI to delay rebound brain alkalosis and minimise subsequent cellular injury.
Chemical shift imaging is an extension of single voxel MR spectroscopy. Instead of obtaining spectra from one or two large voxels in the brain, this technique can obtain spectra simultaneously from numerous voxels at about 1 cm3 resolution and results in a brain metabolite concentration map. When applied to the developing brain, the technique is likely to greatly enhance our understanding of regional biochemical development and assess biochemical response to injury. Further developmental effort is needed from manufacturers to make these techniques suitable for the neonatal brain. Future applications of MR spectroscopy will also benefit from the newest generation of high strength magnets operating at 3 and 4 T, allowing greater sensitivity in metabolite detection and increased chemical shift dispersion.
Quantitative MR measurements
Recently, a new MR era has emerged using more quantitative MR measures. Precise assessment of grey and white matter volumes has been achieved by segmentation of the imaged volume into tissue types followed by 3D rendering, and groups have begun to work on advanced segmentation techniques using atlas information to guide segmentation algorithms. This provides a powerful method of projecting atlas information into data sets of patients.37 New insights into the response of the preterm brain to injury have emerged from quantitative MR studies. Two studies from separate groups have shown that preterm infants with perinatal WMD scanned at term had a reduced volume of cortical grey matter compared with those without WMD.38,39
Diffusion weighted imaging, diffusion tensor imaging, and fibre tracking
The development of diffusion weighted imaging and diffusion tensor imaging has offered the possibility of going beyond anatomical imaging and studying tissue structure at a microscopic level in vivo. Diffusion weighted imaging measures the diffusivity of water molecules on MR imaging; an increase in signal intensity on diffusion weighted imaging is associated with the accumulation of diffusion restricted water in the intracellular space resulting from the breakdown of transmembrane pumps. White matter fibre tracts have been visualised using diffusion tensor imaging. These detailed techniques enable the assessment of the anatomical basis of the more subtle forms of preterm brain injury not detected with conventional MR imaging.
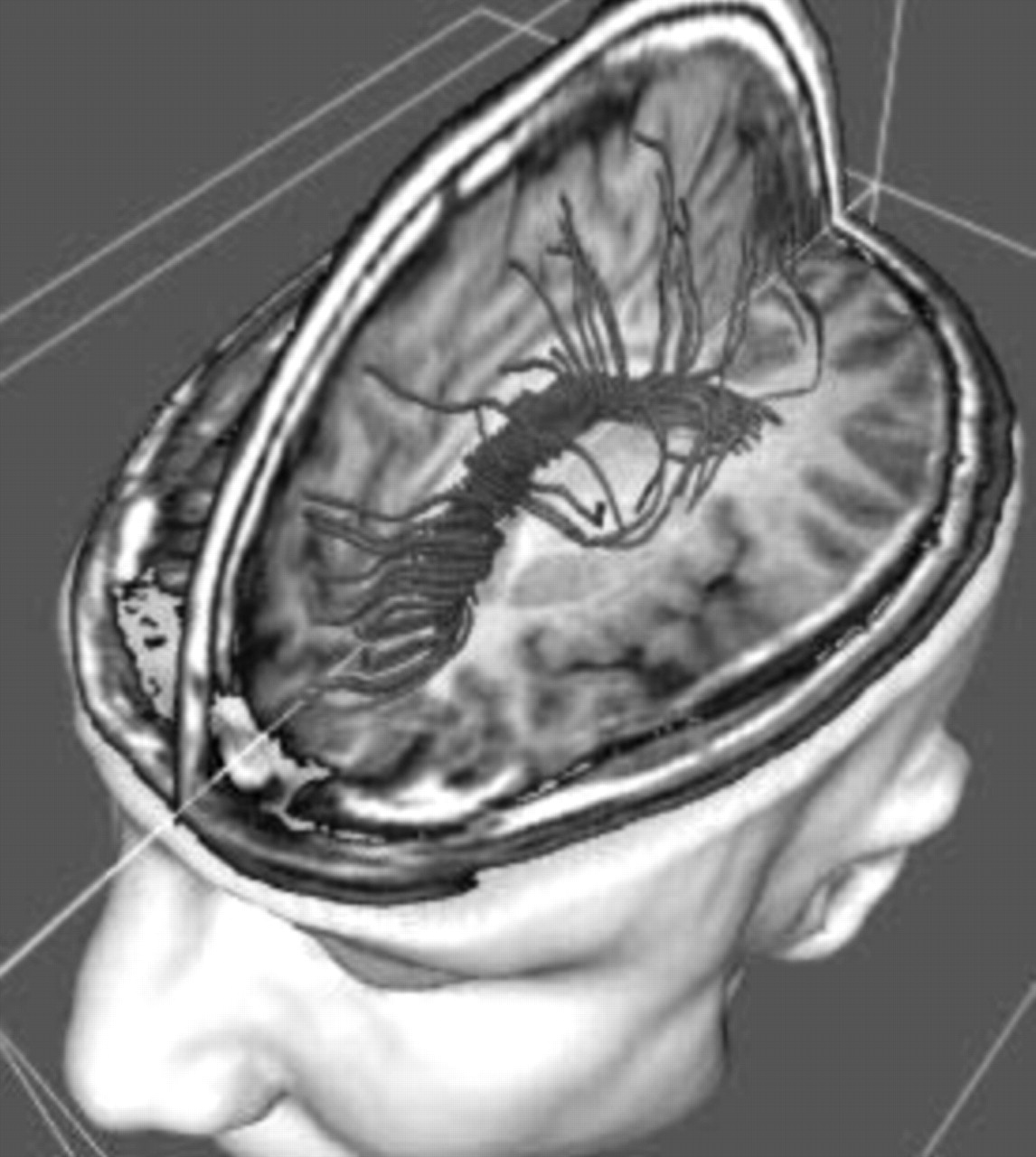
A recent study using diffusion tensor imaging in preterm infants with WMD showed that the WMD has a deleterious effect on subsequent development of white matter fibre tracts both in the area of original injury and in more distal parts of the brain containing fibres that descend from the injury such as the internal capsule.40 Such studies of neuronal connectivity hold much promise in furthering our understanding of the effect and response of injury in the preterm brain. In combination with fMRI, fibre tracking will be a powerful tool for studying neurocognitive networks and improving understanding of brain function (fig 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Fibre tracking which in the future may be possible using diffusion tensor imaging. If successful, this technique has huge potential in furthering our understanding of preterm white matter damage.
Functional magnetic resonance imaging (fMRI)
fMRI can detect regional changes in blood oxygenation associated with local metabolic activation of the brain. The technique has become a powerful tool for cognitive neuroscience research; visual, auditory, motor, and many neuropsychological tasks have been localised to specific brain regions using fMRI. Development of brain function and localisation of specific brain activity in the newborn and developing infants would be of great interest although the technical problems of movement artefact and stimulus presentation are formidable. Preliminary data on neonatal fMRI in term and preterm infants are becoming available.41
Magnetisation transfer imaging
Magnetisation transfer imaging detects changes in the properties of water protons and other magnetic nuclei—for example, macromolecules—as they move from one physical state or chemical configuration to another. The most productive medical application of this technique has been the application of magnetisation transfer contrast to the study of white matter disease, notably demyelination in multiple sclerosis. This technique holds some promise in following brain myelination in the injured preterm and term infant.
SUMMARY
The rapid increase in knowledge that is being obtained using MR has been compared with the giant leap of microscopic technology from Leeuwenhoek’s instrument of the 17th century to modern scanning electron microscopes. As the understanding of molecular mechanisms of disease has accelerated over the last decade, MR technology has kept pace by the development of molecular imaging aimed at exploiting specific molecules as the source of contrast. In the future, as well as observing relatively gross parameters of disease, MR will enable non-invasive exploration beyond the tissue to the cell or even molecular level.42 In the light of these developments, the full impact of MR on our understanding and treatment of the neonatal brain can only be guessed at. In the planning of future neonatal services it is important that access to MR facilities and expertise is considered to ensure that all babies at risk of brain injury will benefit from these developments.
Acknowledgments
We thank Roger Ordidge and David Gadian for helpful advice on the preparation of this article.
Magnetic resonance imaging and spectroscopy techniques have huge medical and scientific potential in neonatal brain imaging
REFERENCES
Linked Articles
- Fantoms