Article Text

Statistics from Altmetric.com
Editor—The results of Sinha and colleagues’ study, showing that volume controlled ventilation was better than time cycled pressure limited ventilation (TCPL), are, at first sight, difficult to explain.1 In both modes, delivered by Bird VIP, the tidal volume was 5–8 ml/kg. Furthermore, the figures indicated almost identical volume and pressure delivery, despite strikingly different flow traces. We therefore investigated this further, using a lung model, by comparing the two ventilation modes via the Bird VIP to TCPL using the SLE 2000 ventilator.
To mimic the illustration in Sinha et al’s study, we used an I:E ratio of 1:1, a rate of 74 breaths per minute, and an inspiratory time of 0.4 seconds. The minimum, weight of infants recruited by Sinha et al was 1200 g, and we would ideally have used a delivered volume of about 7 ml (6 ml/kg).2 Unfortunately, the manufacturer specifies Bird’s minimum volume delivery to be 20 ml; on measurement it was actually 15 ml, and this was therefore the volume that we used.
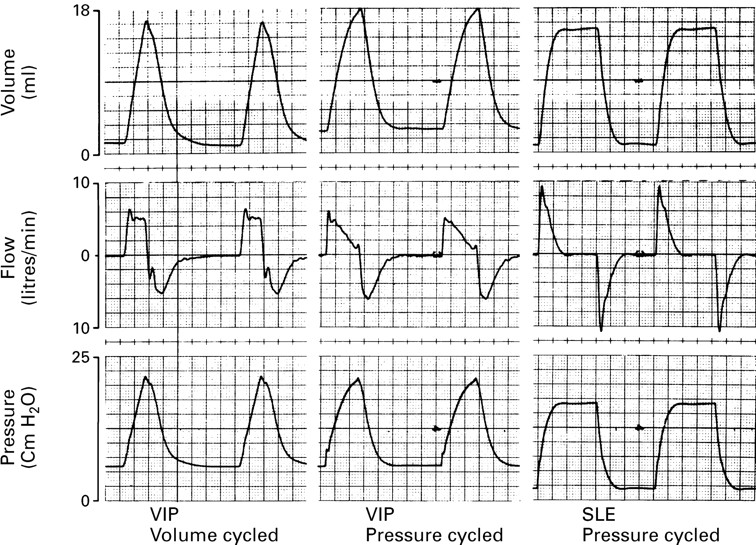
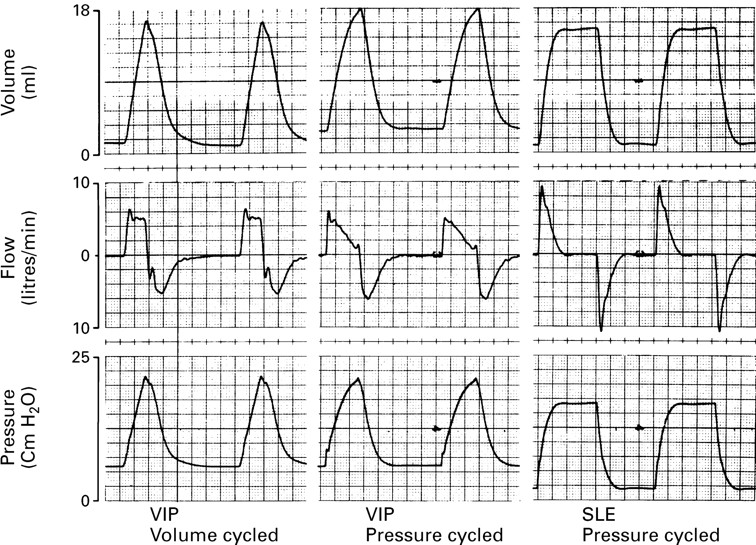
Flow, volume, and pressure signals were recorded simultaneously. The flow signal, from a pneumatograph placed between the lung model and ventilator circuit, was integrated to give volume. Airway pressure changes were measured from a side port on the pneumatograph. The volume and pressure waveforms of the Bird VIP were similar in volume controlled (VC) and TCPL modes (fig 1), but in the VC mode flow was constant over the latter part of inflation, producing a linear volume trace that was different from that produced in the study of Sinhaet al.1 At the same ventilator settings, TCPL via the SLE incorporates a positive pressure plateau, which is therefore lower, and potentially less damaging peak pressures could be used to achieve the same mean airway pressure. The pressure waveform also has a sharper upstroke—that is, the peak pressure is achieved more rapidly—and a sharper downstroke—that is, less “inadvertent” PEEP which impairs carbon monoxide elimination.3
{kind=link}
Comparison of VC (left) and TCPL (middle) ventilation delivered by the Bird VIP and TCPL by the SLE (right). Volume (upper), flow (middle), and pressure (lower) trace for each ventilation mode.
These results suggest that the TCPL mode of the Bird VIP, as reported by Sinha et al, may be inferior to the TCPL produced by a standard neonatal ventilator. Therefore, the latter should be compared with VC using the Bird VIP before it can be assumed that VC is more effective than TCPL ventilation.
Dr Sinha and Professor Donn respond:
Editor—The study by Greenough and Milner attempted to duplicate the conditions of our clinical trial in a comparison of two different devices that provide neonatal time cycled, pressure limited, ventilation. However, direct comparisons are flawed by some assumptions made in the design of their test lung trial.
First, no information is provided about the flow rates used. This may seem trivial, but the inspiratory time during volume controlled ventilation is determined by the flow rate. Furthermore, because flow synchronisation was used in our clinical trial, inspiratory times for patients in the pressure limited group would fluctuate from breath to breath according to the patient’s own breathing cycle.1-1 1-2 Second, the settings chosen for this bench trial—rate of 74 breaths per minute and inspiratory time of 0.4 seconds—would almost assuredly lead to gas trapping and inadvertent peak expiratory end pressure in a clinical trial in which patients like ours exhibited altered compliance. Third, the figures generated for our publication were schematic, not actual, and were intended to display the differences in how flow is delivered by the two modes.1-1
There also seems to be some confusion regarding the minimal tidal volume delivery from the VIP BIRD infant/paediatric ventilator. This refers only to the volume controlled mode and is the minimal volume which leaves the machine and enters the patient circuit and is indeed 20 ml. However, the amount of volume which actually reaches the patient and is measured at the proximal endotracheal tube is less as a consequence of compressible volume loss and tiny leaks. Much smaller tidal volumes can be delivered in the pressure limited mode, and thus it was not necessary for the investigators to have arbitrarily chosen the volume they did.
The conclusion that “lower and potentially less damaging peak pressure” might reduce lung injury remains speculative and ignores the impact of the duration of positive pressure to which the alveoli are exposed in generating overdistension. We agree that this would be a worthwhile parameter to study using a well designed clinical trial with a sufficient sample size to achieve reasonable statistical power.