Article Text

Statistics from Altmetric.com
We read the article by Reece et al1 and followed the subsequent correspondence with interest. In the light of the recent review commissioned by The Chief Medical Officer for England, physicians must be aware of potential complications of peripherally inserted central catheters (PICCs).2 Although the true incidence of such events will only be known with prospective data collection, retrospective studies suggest a complication rate (pleural/pericardial effusions) of 0.5% per line insertion.3 The Department of Health (DoH) paper in response to this review recommends placement of central venous lines outwith the cardiac chambers.4 However, complications related to central lines are not only confined to the thorax. We report three cases of delayed detection of peritoneal extravasation related to central venous catheters.
Case 1. An 8 week old malnourished infant was intubated and ventilated for acute onset severe respiratory distress after a brief flu-like illness. His endotracheal secretions were positive for respiratory synotial virus, and a previously undetected myopathy was suspected and investigated. He required prolonged ventilation and received blood transfusions through a triple lumen right femoral venous catheter for anaemia. On the fifth day after admission, he developed abdominal distension, and a diagnostic tap under ultrasound guidance showed haemorrhagic ascites. A contrast radiograph of the femoral catheter showed extravascular spillage of dye, in this case in the extraperitoneal space. In retrospect, the infant showed no rise in haemoglobin after two packed cell transfusions. Extravascular migration of the catheter tip was diagnosed and the catheter was promptly removed.
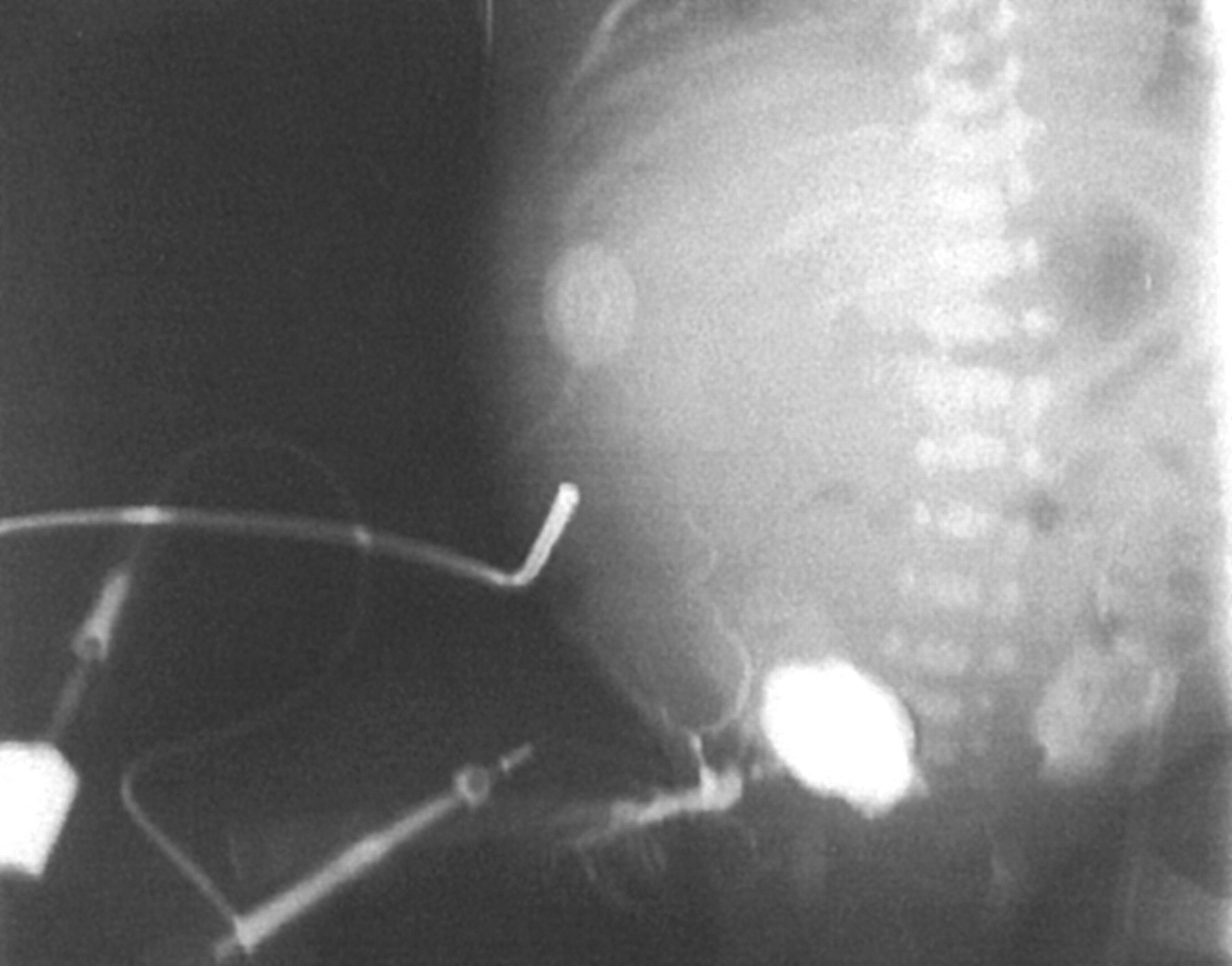
Case 2. A 24 week preterm female infant was admitted to the neonatal intensive care unit where she was ventilated and treated with surfactant. Severe respiratory distress of prematurity, patent ductus arteriosus, and sepsis complicated the initial course. The patent ductus arteriosus did not respond to two courses of indomethacin, and surgical ligation was scheduled on day 13 of life. A PICC was removed because of suspected catheter sepsis, and she was treated with intravenous antibiotics. She had a right femoral venous central single lumen catheter through which she received parenteral nutrition and blood transfusions on the unit. Her anaemia failed to respond to the three packed cell transfusions, and, when she developed abdominal distension with bluish discolouration in the groin, the femoral line was radiographically reviewed after injection of contrast material. Extravascular spillage of the dye was noted in the extraperitoneal space and the subcutaneous tissue of the lower abdominal wall (fig 1).
Case 3. A 28 week preterm infant with a PICC in the leg developed a skin abscess at the xyphisternum. An abdominal radiograph with contrast injected through the catheter showed retroperitoneal extravasation of the contrast (fig 2). The PICC was removed and the infant made a full recovery.
In each of these case reports, femoral catheter tip migration was detected after extravascular extravasation of blood or parenteral nutrition fluid. Haemoperitoneum has been reported in the past as a complication of central catheters but may not be widely recognised. In comparison with PICCs, these catheters are shorter and more rigid, hence more likely to perforate the vessel wall. Femoral venous access is readily obtained in infants and is commonly used in intensive care units for parenteral nutrition, maintenance fluids, blood transfusions, and other parenteral treatment. Although malpositioning of a femoral catheter is readily detected in most instances during placement, a spontaneous extravascular migration of a previously well placed catheter tip is possible in some cases. As opposed to frank rupture of the blood vessel and haemorrhage into the retroperitoneum, slow extravascular infusion of blood in the low resistance extraperitoneal space may not be promptly detected in the absence of a high index of suspicion. In preterm newborns and malnourished infants, the integrity of the vessel wall may be compromised, and migration of a previously normally positioned catheter tip may be more likely. Femoral venous catheter tip positions must be reviewed in all cases of unexplained ascites and abdominal distension. Contrast radiography, digitalised image inversion, and ultrasonography have a role in determining catheter tip position and diagnosing malpositioned intravascular catheters.5
We agree with the DoH recommendation that there should be a prospective national audit of such cases.

Malpositioned femoral catheter with retroperitoneal extravasation of dye.

{kind=link}
{kind=link}
Radiograph showing spillage of dye in the extraperitoneal space.