Article Text

Statistics from Altmetric.com
Studies report that ECG measures newborns’ heart rate (HR) more quickly1 ,2 and accurately3 than pulse oximetry (PO) in the delivery room (DR). In these studies, separate ECG and PO monitors were applied. The Philips IntelliVue X2 monitor (Philips, Eindhoven, Netherlands) incorporates ECG and Masimo PO technology (Masimo, Irvine, California, USA) and has a portable unit that may be used in the DR. This monitor displays HR faster when the ECG leads are connected to the machine before application to the infant.4 We wished to determine whether the order of application of ECG and PO affected how quickly the ECG HR is displayed and how quickly the ECG HR is displayed compared with a portable PO.
We compared the IntelliVue to the Nellcor Portable SpO2 PM10N pulse oximeter (Covidien, Boulder, Colorado, USA) in stable infants in our neonatal unit with the approval of our ethics committee and parental consent.
The monitors were applied as follows:
IntelliVue, ECG applied first;
IntelliVue, PO applied first; and
Nellcor PO.
The order of application was allocated randomly. For each infant, one investigator was chosen by coin toss to apply the monitors. Another investigator recorded the times taken to (1) apply ECG leads, (2) display ECG HR, (3) display ECG HR in total for the IntelliVue and (4) apply and connect PO sensor, (5) display PO HR and (6) display PO HR in total for the IntelliVue and the Nellcor. We recorded the time for each monitor to display an HR value, not merely the ECG or plethysmographic waveform. We analysed data with SPSS V.20 and compared median values with the Wilcoxon signed-rank test.
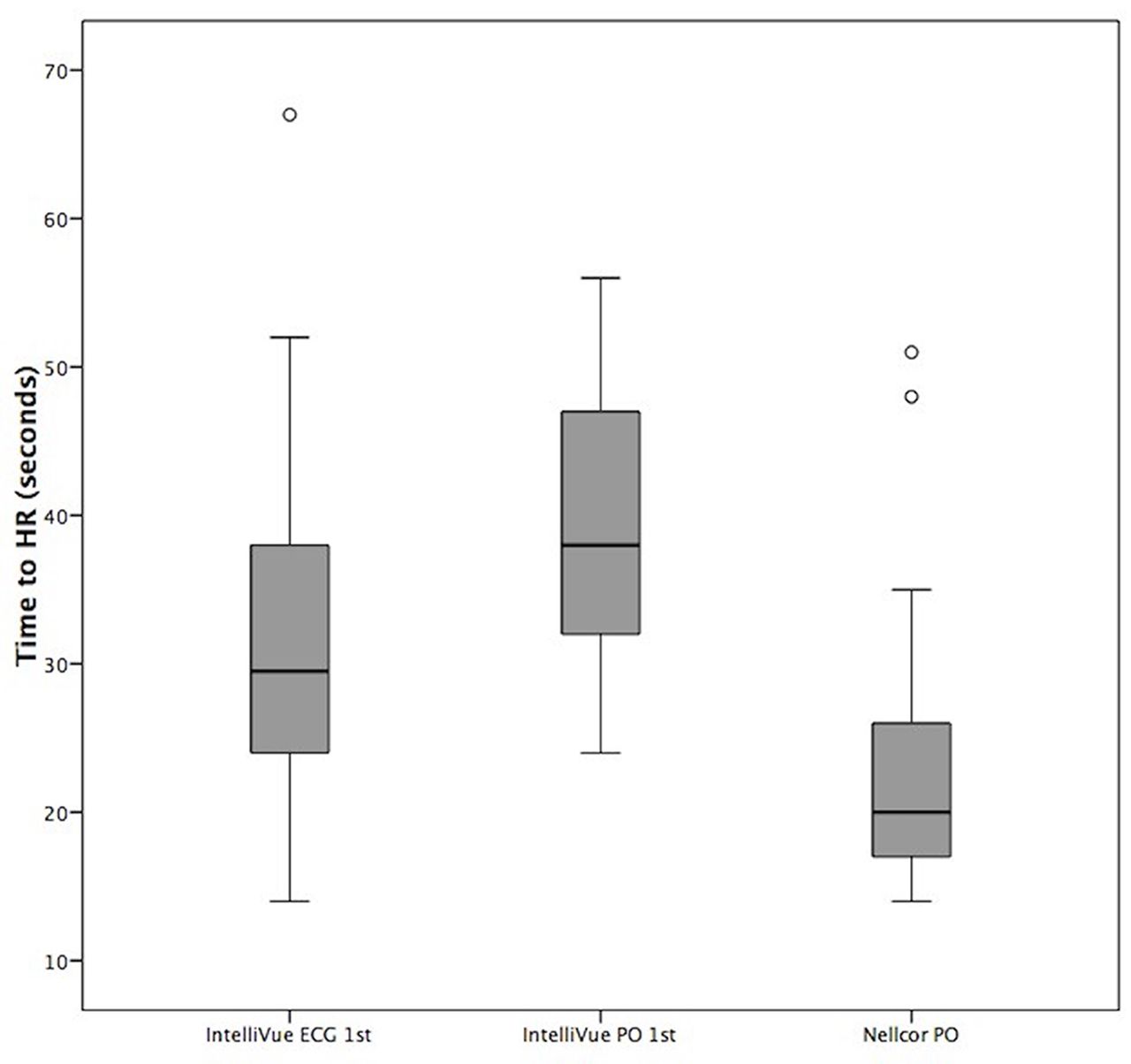
We studied 30 infants (median (IQR) gestational age 37 (30–40) weeks and birth weight 3.04 (1.42–3.52) kg) at a median (IQR) of 4 (2–12) days. ECG HR was displayed faster when the ECG was applied first (median (IQR) 30 (24–38) s vs 38 (32–47) s, p=0.004) (table 1). The IntelliVue displayed the HR more slowly than the Nellcor (median (IQR) 30 (24–38) s vs 20 (17–26) s, p=0.002) (figure 1).

{kind=link}
Box plots displaying median, IQR and outliers of time to display ECG heart rate (HR) (s) for the IntelliVue ECG applied first and IntelliVue pulse oximeter (PO) applied first and time to display PO HR by Nellcor.
Introducing ECG monitoring in the DR requires resources, in terms of machines, consumables and staff to apply them. To better judge whether it is worthwhile, further study is required to determine whether ECG displays HR more reliably and/or more quickly than PO in the DR.
Median (IQR) time (s) to apply and connect monitors and display heart rate data for IntelliVue and Nellcor
Footnotes
Contributors MM and COD participated in study design, protocol development, submission to research ethics committee, data collection and entry, data analysis and interpretation and drafting the manuscript. LD and EF contributed to data collection. LMC contributed to study design, supervision and review prior to submission.
Competing interests None declared.
Ethics approval Research Ethics Committee, National Maternity Hospital, Dublin, Ireland.
Provenance and peer review Not commissioned; internally peer reviewed.