Article Text

Abstract
Objective Some researchers claim that the quality of informed consent of clinical research participants in developing countries is worse than in developed countries. To evaluate this assumption, we reviewed the available data on the quality of consent in both settings.
Methods We conducted a comprehensive PubMed search, examined bibliographies and literature reviews, and consulted with international experts on informed consent in order to identify studies published from 1966 to 2010 that used quantitative methods, surveyed participants or parents of paediatric participants in actual trials, assessed comprehension and/or voluntariness, and did not involve testing particular consent interventions. Forty-seven studies met these criteria. We compared data about participant comprehension and voluntariness. The paucity of data and variation in study methodology limit comparison and preclude statistical aggregation of the data.
Results and Discussion This review shows that the assertion that informed consent is worse in developing countries than in developed countries is a simplification of a complex picture. Despite the limitations of comparison, the data suggest that: (1) comprehension of study information varies among participants in both developed and developing countries, and comprehension of randomisation and placebo controlled designs is poorer than comprehension of other aspects of trials in both settings; and (2) participants in developing countries appear to be less likely than those in developed countries to say they can refuse participation in or withdraw from a trial, and are more likely to worry about the consequences of refusal or withdrawal.
- Informed consent
- clinical trials
- developing countries
- developed countries
- voluntariness
- comprehension
- research ethics
Statistics from Altmetric.com
- Informed consent
- clinical trials
- developing countries
- developed countries
- voluntariness
- comprehension
- research ethics
Introduction
Many prospective research participants in developing countries have little formal education, lack familiarity with biomedical research and consent procedures, and have limited access to healthcare services. Consequently, it is widely believed that they have more difficulty comprehending study information and providing voluntary consent than do their counterparts in developed countries.1–11 Such views are echoed in ethics guidelines such as those of the Council for International Organizations of Medical Sciences (CIOMS),12 in a report by the National Bioethics Advisory Commission,13 and in the popular press. For instance, a front-page New York Times article framed the problems with comprehension in a trial in the Ivory Coast as a matter of an impenetrable wall between scientific complexity and the ability of locals to understand it—one participant was described as “still not grasp[ing]—even after repeated questioning—what a placebo is or why she might have been given that instead of a real medicine”.14
But what do we know about the quality of informed consent in developing country research? Does available evidence demonstrate that the quality of informed consent from developing country participants is worse than the quality of informed consent from participants in developed nations?
To begin addressing these questions, we reviewed and compared available data on the quality of informed consent from research in both developing and developed countries. We identify similarities and differences between studies of consent in developed and developing countries, highlight gaps in the available data, and make recommendations for future research on the quality of informed consent.
Methods: search strategy and selection criteria
We conducted a comprehensive PubMed search using the Medical Subject Headings (MeSH) terms informed consent, comprehension and decision making in combination with clinical trials or randomized controlled trials (box 1). In addition, we examined bibliographies,15 literature reviews16 17 and reference lists from relevant papers, and consulted with international experts on informed consent to clinical research.
MeSH terms strategy
(informed consent[mh] AND (Comprehension[mh] OR decision-making[mh])
AND (randomized controlled trials as topic[mh] OR clinical trial as topic[mh])
AND (Humans[Mesh] AND English[lang]))
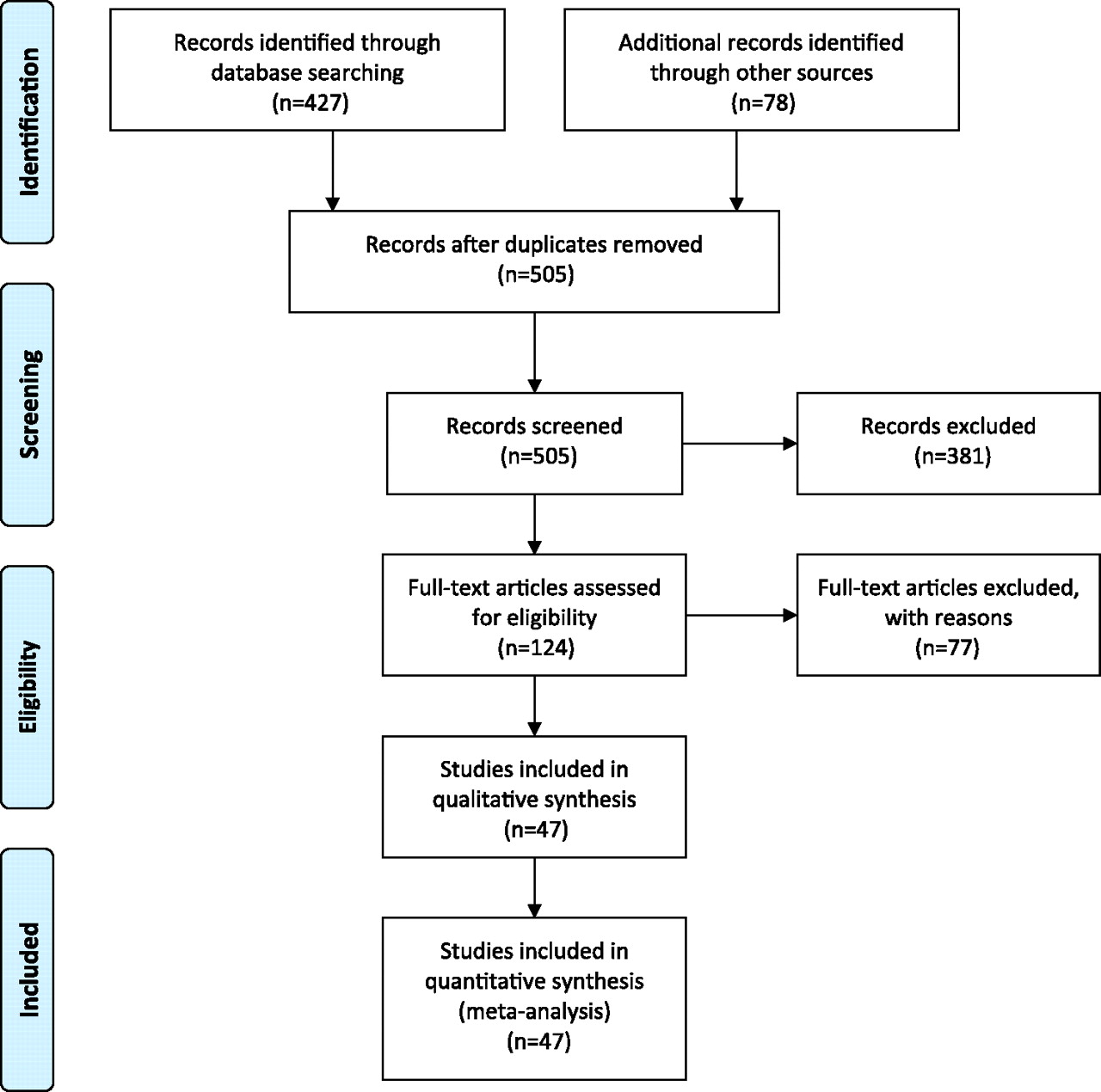
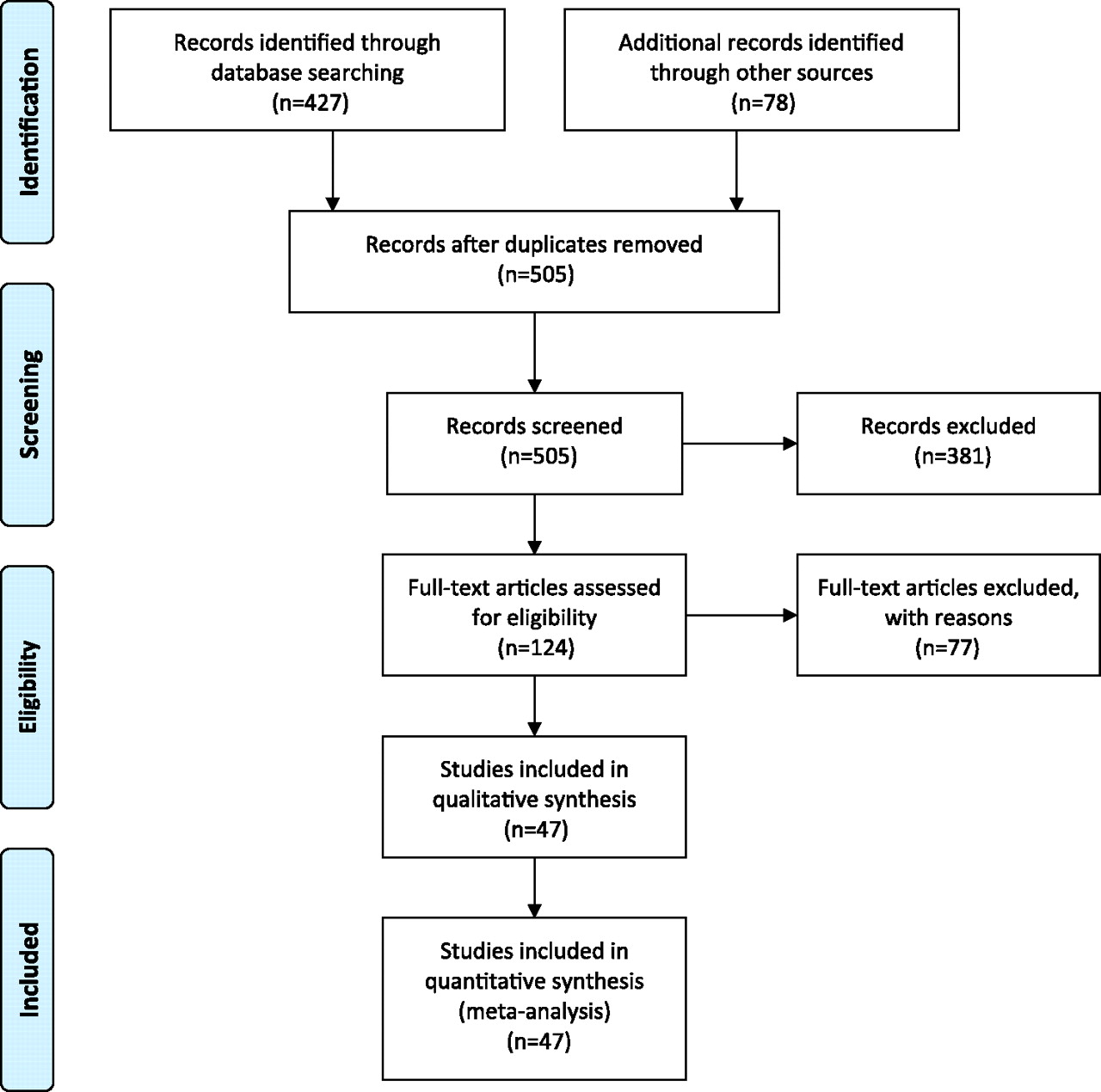
We included studies that met four criteria: (1) used quantitative methods to study informed consent (to allow for comparison of relatively similar data sets); (2) surveyed participants or paediatric participants' parents in actual clinical trials rather than hypothetical scenarios (as we are concerned with what participants understand and how they make decisions in real trials); (3) did not test informed consent interventions aimed at improving its quality (to avoid confounding results); and (4) assessed at least one of two domains critical to measuring the quality of informed consent: comprehension of study information and voluntariness of consent. While some published data on disclosure exist, there are little to no comparable data from non-intervention utilising trials that evaluate understanding and comprehension relative to the quality of disclosure. A total of 427 studies were identified through the PubMed search (figure 1) and 79 from bibliographies, literature reviews, reference lists and consultations with experts. Of those 506 studies, 47 met all four criteria: 18 studies evaluated the quality of informed consent in trials in developing countries and 32 studies evaluated the quality of informed consent in trials in developed countriesi (tables 1 and 2). Identified studies were reviewed by the authors and information extracted regarding the type and location of the clinical trial, the sample size, and the method and timing of assessing informed consent. Data about participants' comprehension of trial information and voluntariness were extracted, including understanding of the purpose and nature of the research, the risks and side effects, and randomisation and placebo controlled design (tables 3–5), as well as perceived pressure and participant knowledge of the right to refuse to enrol or withdraw from a trial (table 6). Direct comparison or meta-analysis of study data was not feasible, as the relevant studies did not employ a uniform methodology or study design.
{kind=link}
PRISMA 2009 flow diagram (adapted from Moher D, Liberati A, Tetziaff J, et al; The PRISMA Group. Preferred reporting items for systemic reviews and meta analyses: the PRISMA statement. PLoS Med 2009;6:e1000097. For more information, visit http://www.prisma-statement.org). This figure is produced in colour in the online journal—please visit the website to view the colour figure.
Developing country consent studies
Developed country consent studies
Understanding of research nature and purpose*
Understanding of risks and side effects*
Understanding of study design and randomisation*
Voluntariness: knew could withdraw or refuse*
Results
Study characteristics
Eighteen studies conducted in 11 different developing countries examined the consent of participants in clinical research on vaccines, nutritional supplements, HIV treatments, immune correlates in children, diarrhoeal disease in children, anti-malarial drugs and genetics (table 1). Sample sizes ranged from 33 to 700 research participants. Seven studies interviewed a parent of a participating child,18 21 22 24 26 29 33 and of those seven, three interviewed only the mothers.22 24 33 Thirteen studies19–21 23 26–33 35 used structured or semi-structured interviews, while five used questionnaires.18 22 24 25 34 In nine studies, participants were interviewed close to the time of consent18 23 24 26 28 29 33–35 and in eight others interviews were conducted 1–14 months or longer after the participant gave consent.19–22 25 27 30 31 In one study, the timing was not specified.32
Thirty-one studies, conducted in eight developed countries, examined the consent of participants involved in oncology, cardiology, gynaecology, HIV, analgesics/anaesthesia, neurological, antidepressant, antipsychotic, emergency management, arthritis, paediatric asthma, paediatric febrile convulsion, diabetes, malaria and genetics research (table 2). Sample sizes ranged from 21 to 570 research participants. Six studies surveyed the parents of children in paediatric trials.40 42 45 48 54 57 Sixteen studies used structured interviews,19 38 39 42 45 47 48 50 54 57 58 60–64 nine used mailed surveys,37 41 43 46 49 51–53 59 and six used questionnaires.18 36 40 44 55 56 In eight studies, questions were asked close in time to when consent was given, in each case within 48 h of consent18 39 40 42 48 55 60 64; the remaining 23 studies surveyed participants weeks to months after consent.19 36–38 41 43–47 49–54 56–59 61–63
Comprehension and recall of trial information
Participant understanding of research purpose, risks/side effects and design varied substantially across informed consent studies from both developing and developed countries. Across studies, comprehension of trial purpose or nature appeared to be better than comprehension of trial design and randomisation.
Trial purpose and nature
Available data show no substantial difference between participants in developing countries and those in developed countries with respect to their understanding of trial purpose, defined as the goal of a given clinical trial (table 3). In the developed country studies that measured it, understanding of trial purpose ranged from 10% of US males who understood the purpose of a variety of trials they were participating in62 to 100% of Canadian participants who understood the purpose of a neuro-oncology trial.45 Understanding of trial purpose in developing country studies also varied, ranging from 26% of Malian parents who understood the purpose of a malaria trial for their children26 to 90% of mothers with children in a paediatric influenza trial in The Gambia.33 Similarly, reported understanding of trial nature, assessed by participants' understanding that they were participating in research and of the investigational and experimental nature of research interventions, varied from 31% of participants in a US phase 1 oncology trial50 to almost 100% of participants in both a Swedish and a Finnish trial,51 59 and from 47% of women in a Bangladeshi nutritional trial for iron supplements32 to 100% of women in an HIV trial in Côte d'Ivoire.30
Risks/side effects
The percentage of participants who could recognise or name trial side effects and risks also ranged widely among the studies reviewed (table 4). Reported understanding of side effects varied depending on how the questions were framed—more participants were able to recognise side effects from a list than were able to name or explain them in response to open-ended questions. For example, 86% of participants in a US analgesic trial recognised at least one side effect from a list, but only 48% were able to name at least one without the help of a list.58 In a US rheumatoid arthritis trial, 30% responded that they knew the trial drugs were not completely safe, but were not asked to recognise or name the specific risks of the drugs.44
In consent studies of developing country trials, 79% of participants in a South African vaccine trial knew the risks involved22 and 97% of Thai participants recognised possible side effects of an experimental HIV vaccine,35 yet only 7% of Malian parents recognised that the investigational vaccine being given to their child might have side effects.26
Randomisation and placebo trial design
Understanding of randomisation also varied among participants in both developing and developed country trials, but across all studies, understanding of randomisation was low compared to understanding of other aspects of a trial (table 5). In developed country studies, understanding of randomisation appeared to vary according to how close to actual consent it was measured. For example, 68% of parents understood randomisation when asked within 48 h of consent in US paediatric oncology trials,48 and as many as 79% understood randomisation in an HIV vaccine trial when assessed immediately after disclosure.55 Yet fewer than half of the participants were reported to comprehend randomisation in six developed country studies in which understanding was assessed months or years after consent.44 46 47 51 53 63
Five developing country studies measured understanding of randomisation (table 5); four of those five measured it within 1 week of consent.18 20 26 28 29 Comprehension of randomisation ranged from as high as 90% of parents whose children were enrolled in a malaria vaccine trial in Mali18 to as low as 19% of parents whose children were enrolled in a malaria treatment trial in Uganda.29
Between 64% and 88% of participants understood the study design in six developed country trials,41 44 46 53 63 64 yet only 39% of the participants in a set of Canadian trials recalled their own chance of receiving placebo, and 29% of them “thought that the doctor [had known] what kind of medication they were taking”.46 Knowledge of placebo was measured in three developing country studies: 10% of mothers enrolling children in a Gambian trial understood the placebo control design,33 13% of Ghanaian trial participants knew that not all trial capsules were the same,23 and 49% of South African participants knew they had a 50% chance of receiving placebo.27
Although measured infrequently, individuals' understanding of research design diverges from their understanding of how it specifically applies to them. In one Thai HIV treatment trial, 31% correctly responded that half the participants would get the investigational drug, yet 48% said they had a 50/50 chance of receiving it.28 In a Ugandan malaria trial, 19% of parents knew that not all children would receive the same treatment, even though 84% recalled being told about treatment assignment.29 Similarly, in a US rheumatoid arthritis trial, 87% of participants said that some people in the trial would get placebo, but only 50% thought they personally could receive placebo.44
Voluntariness
Data on voluntariness is organised into two categories: (1) participants' perceptions of pressure (not reported in a table); and (2) participants' knowledge of the right to refuse or withdraw from participation (table 6).
Pressure
Questions assessing perceptions of pressure differed across informed consent studies—some focused on whether or not participants knew or felt that participation was voluntary, while others asked more specific questions about the source and amount of pressure felt by participants.
Most (90%–99%) participants in a US hypertension trial, a Canadian neuro-oncology trial and UK paediatric trials reported no pressure to participate19 38 40 or reported that participation was voluntary.52 At the same time, 31% of US oncology and cardiology trial participants said that they felt that they had little other choice than to participate,54 25% of parents in a Netherlands paediatric oncology trial indicated that they felt obliged to participate53 and 18% of Danish participants in an acute myocardial infarction trial reported feeling ‘under pressure’, although 70% said the decision was ‘fully theirs’.41
Five developing country informed consent studies measured general perceptions of pressure and voluntariness. Most mothers (95%) in a Ghanaian paediatric trial21 and most participants (99%) in a South African influenza vaccine trial27 said participation was voluntary. Similarly, most parents in an Indian paediatric trial (98%) reported that they joined the study freely without any pressure or compulsion.24 In contrast, in another South African trial, 84% of the evaluation group and 93% of the sensitisation group reported feeling that participation was compulsory.34
In consent studies that distinguished sources of pressure, more trial participants reported feeling pressure from their disease or circumstances than from other people. Although 29% of US phase I and phase II oncology trial participants said that their physician did not actively want them to make their own decision,61 only 14% in a Swedish gynaecology trial,59 7% in another US oncology trial62 and 6% in a set of varied US trials reported feeling pressure from a clinician.39 In the same oncology study in which 7% reported pressure from a clinician and 9% from their families, a full 75% reported pressure due to their progressive cancer.39 In another US paediatric oncology trial, 70% of the parents cited high levels of distress and ‘feeling overwhelmed’ during the consent process.45 Few participants in developed country trials reported pressure from anticipated consequences of withdrawing: 98% of UK anaesthesia trials participants,52 86% of Canadian neuro-oncology trial participants38 and 85% of Danish cardiology trial participants41 knew that refusal to participate would not compromise their care.
In developing country studies, reported pressure from others was also generally low, ranging from 6% of participants reporting pressure from spouses, family or the research team in a Ugandan paediatric malaria treatment trial29 to 26% reporting pressure from village elders in a Malian paediatric vaccine trial.26 Reported pressure came from various sources, for example, from village elders (26%), the research team (12%) and a spouse (7%) in the aforementioned Malian study,26 and from a close friend (15%), a family member (7%) or their doctor (2%) in an HIV treatment trial in Thailand.28 Similarly, in a Ugandan paediatric trial, 15% of parents reported feeling pressure from others, including spouses (6%), family or friends (6%) or the research team (6%), but 58% reported pressure because of their child's illness.29 However, in one Gambian trial, 9% of mothers offered spontaneously and 36% agreed when directly questioned that it would have been hard to refuse participation—some reported feeling group pressure after watching other mothers agree to participate.33
Participants in developing countries reported pressure from fear of the consequences of withdrawing. Although in one South African trial, 88% said their usual care would not be affected if they refused,27 87% of participants in a Bangladeshi trial felt that the trial offered such advantages that they couldn't refuse.32 Similarly, 32% of the evaluation study group and 23% of the sensitisation group in a South African perinatal HIV transmission trial thought that care would be compromised if they did not participate,34 and 44% of parents in a paediatric malaria vaccine trial in Mali said they would lose healthcare access if they withdrew.26
Knew they could refuse or withdraw
The clearest differences between respondents in developed and developing country informed consent studies were related to knowledge of the right to refuse to participate in research or to withdraw (table 6). In 15 of 18 developed country studies that measured this, more than 75% of trial participants knew they could withdraw or refuse,18 19 36 37 40 43 44 49 52–54 60–62 64 and in 10 of these studies, 90% or more said they could withdraw from research.18 19 36 37 40 43 44 49 53 60 In one US paediatric oncology trial, 90% of the majority race English speaking parents, 78% of the minority race English speaking parents and 60% of the minority race non-English speaking parents knew they had a right to withdraw their children from the trial.48
In contrast, in five of 15 developing country studies that measured it, less than half of respondents knew they could withdraw from research.22 26 30–32 As few as 10% of mothers in Mali knew they could withdraw their child from a malaria vaccine trial at any time,26 and 27% of participants in an HIV trial in Côte d'Ivoire knew they could withdraw at any time.30 However, in some developing country trials a higher percentage of participants knew they could withdraw or refuse, for example 50% of parents in a paediatric diarrhoeal trial21 knew they could leave the trial at any time, >90% of adults and parents of children in a Malian malaria vaccine trial18 knew they could withdraw from the trial and 88% of Thai vaccine participants knew they could ‘refuse to participate at any time’.35 One study of a South African HIV trial17 reported that 93% of the women knew they had the right to quit, but 98% said they believed the hospital would not allow them to quit.34
Discussion
This is the first comparison of quantitative studies of the quality of informed consent from individuals participating in clinical trials in both developed and developing countries. Our review shows that the assertion that research informed consent is worse in developing countries than in developed countries is an oversimplification of a complex picture of the quality of consent. The quality of informed consent depends on the type and amount of information disclosed, adequate comprehension of trial information, and a voluntary decision to enrol. The existing data, which use comprehension and voluntary decision-making as measures of the quality of consent, do not support a categorical difference between the quality of consent from individuals in developed countries and the quality of consent from individuals in developing countries.
A paucity of data, especially from participants from developing countries, as well as variations in trial type, study methodology, sample size, measures used and timing of data collection relative to obtaining consent, limits comparison and statistical aggregation. Nonetheless, these data suggest certain important trends and point to the need for further research.
Our review highlights the following: (1) comprehension of study information varies among trial participants in both developed and developing countries, and comprehension of randomisation and placebo controlled designs is generally lower than comprehension of other aspects of a trial; (2) research participants report different sources of pressure to enrol, and those in developing countries are less likely than those in developed countries to say they can refuse or withdraw from participation, and more likely to worry about the consequences of refusal or withdrawal.
Data show a range of understanding of trial information in both developed and developing country trials. Individuals across studies tended to know that they were involved in research and often responded correctly to questions about the nature and purpose of the research, yet participants everywhere had more difficulty understanding information about trial design, randomisation and placebo controls. Not only are these methods and concepts unfamiliar to many people, but such methods may be contrary to their expectations or hope for therapeutic benefit, making them more difficult to comprehend. Notably, some studies reveal discrepancies between participants' understanding of what will happen in a trial and how this information will affect them directly. Knowledge of facts and appreciation of those facts are different aspects of understanding, both of which are important to informed consent.65 This discrepancy is a challenge for informed consent everywhere, and although few studies attempted to measure it, the present data do not suggest a difference in appreciation between developed and developing country participants.
Second, the data on refusal and withdrawal indicate a troubling trend. Finding it difficult to refuse participation in or withdraw from a trial, feeling pressure to join or stay enrolled in a trial, or worrying about the consequences of withdrawing all relate to the voluntariness of an enrolment decision. Studies which used these measures of voluntariness show that a disquieting number of participants, and more in developing country trials than developed country trials, do not know or do not believe that they can refuse to participate or can withdraw from research. Few studies probed these responses further to explain why participants felt they could not refuse or withdraw. Possible explanations include deference to authority, cultural norms, or a founded or unfounded fear of not being able to access needed care.
Lastly, while investigations of the impact of pressure on voluntariness were limited, overall few research participants report feeling pressured to participate in research, and those that did often felt pressure from their circumstances–such as worsening illness or fear that care would be withdrawn—more than from other people. Participants in developing countries were more likely to report pressure from fear of the consequences of withdrawing, including decreased access to healthcare. These issues merit further study.
Recommendations for future research
These data reveal that there is much to be done to improve the quality of informed consent in both developed and developing countries and that additional research would facilitate definitive conclusions about the quality of informed consent around the world. Currently available evidence regarding the effectiveness of strategies to improve consent is limited.66–68 Variation in methodology, trial types and populations across studies reviewed raised challenges about how to accurately understand and measure the quality of informed consent. Design and implementation of improvement measures depends on careful attention to, and rigorous delineation of, what the quality of consent entails.
Studies of the quality of informed consent would be greatly enhanced by a core set of validated questions that measure the comprehension and voluntariness of participants at the time of decision-making, and by comparison of participants from similar medically defined groups participating in similar types of research. Studying the quality of consent in multi-national trials, such as was done in one multi-site hypertension study we reviewed,19 would allow for useful comparisons between developed and developing countries. Additionally, more detailed and comprehensive studies of voluntariness are needed, including investigation of sources of pressure to participate and fears about withdrawal or refusal. Future studies should include detailed investigation of associations between cultural norms and attitudes, and socio-demographic characteristics such as education, literacy and socioeconomic status to better understand the impact of these factors on informed consent in both developed and developing countries. Innovative strategies and rigorous studies are sorely needed to facilitate improvement in informed consent to better satisfy one of the fundamental requirements of ethical research.
References
Other content recommended for you
- Seven-step framework to enhance practitioner explanations and parental understandings of research without prior consent in paediatric emergency and critical care trials
- Non-static framework for understanding adaptive designs: an ethical justification in paediatric trials
- Parental attitudes towards and perceptions of their children's participation in clinical research: a developing-country perspective
- Informed consent and assent guide for paediatric clinical trials in Europe
- Fifteen-minute consultation: an evidence-based approach to research without prior consent (deferred consent) in neonatal and paediatric critical care trials
- StaR Child Health: developing evidence-based guidance for the design, conduct and reporting of paediatric trials
- How parents and practitioners experience research without prior consent (deferred consent) for emergency research involving children with life threatening conditions: a mixed method study
- Consent and recruitment: the reporting of paediatric trials published in 2012
- Designing clinical trials in paediatric inflammatory bowel diseases: a PIBDnet commentary
- Informed consent in pragmatic trials: results from a survey of trials published 2014–2019