Article Text

Abstract
Objective Neonatal resuscitation is often retrospectively documented, which can lead to inaccuracy and incomplete recording of delivery room management. In this study, we assessed the accuracy and completeness of neonatal resuscitation documentation in our neonatal intensive care unit.
Methods Recordings of physiological parameters and video data were performed in the delivery room and used to deduct the clinical condition of the infant, the interventions done and their effect on the infant's condition. The data from the recordings were compared with the documentation on neonatal stabilisation in the medical records (paper or digital).
Results Recordings of 54 infants were compared with the documentation in their medical records. In 93% of the medical records delivery room management was documented. The clinical condition of the infant at birth was documented in 76% and 1 min Apgar scores in 98%. Respiratory support was correctly documented in 83%, heart rate in 37% and oxygen saturation in 13%. In 57% use of supplemental oxygen and its indication were correctly reported. Seven infants were intubated and this was correctly documented in 57%. Apgar scores were compared between the recordings and the medical records. At 1 min, 5 min and 10 min after birth the Apgar score, given by the researcher using the recordings, was similar to the scores in the medical records in 33%, 44% and 53%, respectively.
Conclusions Accurate and complete documentation of neonatal resuscitation continues to be a challenge. Recordings of physiological parameters and video imaging can improve documentation by providing detailed information.
- Neonatology
- Resuscitation
- Audit
- Monitoring
Statistics from Altmetric.com
What is known about this topic?
-
Accurate documentation is valuable for audit, research and legal purposes and thorough documentation will thereby contribute to the improvement of the quality of care.
-
It is difficult to obtain complete and accurate documentation of neonatal resuscitation.
What this study adds?
-
Documentation of the condition of an infant and the procedures in the delivery room often do not correspond with data from delivery room recordings of physiological parameters and video imaging.
-
Preprinted resuscitation sheets in the charts ask for few details and, therefore, little information is documented.
-
Recording of physiological parameters and video imaging during neonatal resuscitation is easy to use and can provide the extra details necessary for auditing and educational or research purposes.
-
The data from neonatal resuscitation recordings should be integrated into the infant's medical records.
Introduction
Approximately 10% of newborns require some form of resuscitation after birth.1 National and international guidelines are available with step-by-step flow charts on how to perform optimal resuscitation, with the intention to improve neonatal resuscitation and outcome. The resuscitation procedure, performed interventions and their effect are documented in the infant's medical record. Accurate documentation, reflecting what actually happened in the delivery room, is valuable for audit, research and legal purposes and thorough documentation will, thereby, contribute to the improvement of the quality of care.2 ,2–4 However, various studies have shown that it is difficult to obtain complete and accurate documentation of neonatal resuscitation.4–8 The clinical condition of the infant and the interventions performed are often retrospectively documented, which can lead to inaccuracy.4–8
In the delivery rooms of the Leiden University Medical Center, Leiden, the Netherlands, physiological parameters are recorded simultaneously with video imaging during neonatal resuscitation. Video imaging of resuscitation is considered useful for audit and teaching purposes.9–12 Review of these videos is helpful in detecting bottlenecks during the resuscitation procedure and supports the interpretation of physiological parameters recorded.9 ,11 This approach allows for more objective evaluation of resuscitation and makes all details available for documentation of the event. Usually, recordings are performed when time is available to set up the equipment and parental consent to use the recordings for training, audit and research purposes is sought after the resuscitation.13
We recently reported the usefulness of delivery room recordings for auditing our current resuscitation practices and observed that caregivers often deviate from resuscitation guidelines.14 In this study, we used the recordings to assess the accuracy of documentation of neonatal resuscitation in the delivery room. We hypothesised that delivery room recordings would be more accurate for documentation, and would be helpful to complete the documentation by adding details about interventions to the medical records.
Methods
This retrospective observational study was performed in the neonatal intensive care unit (NICU) of the Leiden University Medical Center, a tertiary level perinatal care centre in Leiden, the Netherlands, with an average of 150 infants <32 weeks gestational age admitted per year.
The resuscitations were recorded by an independent researcher, who did not take part in the resuscitation. Only resuscitations of infants <32 weeks of gestation were recorded for audit, research and teaching purposes. Recordings were performed if time allowed us to set up the equipment and the researcher was available. Written parental consent to use the recording was obtained after birth.
The resuscitations were performed by neonatologists, neonatal fellows or paediatric registrars supervised by a neonatologist or neonatal fellow. In Leiden, a T-piece infant resuscitator (Neopuff, Fisher and Paykel Healthcare, Auckland, New Zealand) is used in combination with a Laerdal silicone round mask (Laerdal, Stavanger, Norway) or a nasopharyngeal tube (endotracheal tube cut at 7 cm) to deliver non-invasive ventilation. When intubation was required, an appropriate sized endotracheal tube was inserted nasally. Local guidelines for neonatal resuscitation have been described previously.14
Recording equipment
The use of a respiratory monitor (Acutronic Medical Systems AG, Hirzel, Switzerland), a Masimo SET pulse oximeter (Masimo Radical, Masimo Corporation, Irvine, California, USA), oxylog (Teledyne, Poway, California, USA) in combination with simultaneous video image recording has been described in detail previously.14 Signals for gas flow, ventilatory pressure, tidal volume, FiO2, oxygen saturation, heart rate, breathing and video images were digitised and recorded at 200 Hz using Spectra Physiological software (Grove Medical, London, UK). Interventions were recorded using a webcam. The video images showed only the hands of caregivers. Parents, obstetric procedures and faces of caregivers were not visible. The Ethics Review Committee of our university hospital approved recording for audit, teaching and research purposes. Parental consent to use the data from the recordings was obtained as soon as possible after birth.
Documentation
Delivery room management is documented on preprinted pages in our medical records. On these pages, information about ventilation, oxygen therapy, intubation, cardiac resuscitation and medication can be specified. Apgar scores, mode of ventilation or the interface used can be ticked in boxes or chosen from pull down menus (in the electronic records). The forms have not substantially changed when moving from paper to electronic medical records. The delivery room evaluation forms used in our unit at the time of the study are similar to the forms recommended by the Neonatal Life Support (NLS).15
Scoring of documentation
Recordings of resuscitations between December 2009 and May 2012 and the corresponding resuscitation sheets in the infant's medical records (paper or electronic) were evaluated for documentation of delivery room management. The complete medical record was reviewed to make sure no misplaced information was missed. Information from the medical records was scored on accuracy and completeness and compared with the data obtained from the recordings. We scored the medical records and recordings on clinical condition of the infant, interventions (such as respiratory support, oxygen delivery and intubation) and the effect of the resuscitation on the infant's clinical condition (eg, heart rate and oxygen saturation). We also reviewed whether subjective or non-medical terms were used. Apgar scores16 given by the caregiver were compared with the researcher's scores after reviewing the recordings. The complete list of scored items can be found in box 1.
Scored items
General
▸ Umbilical cord pH
▸ Time of birth
▸ Caregivers present
First impression
▸ Clinical condition
▸ Apgar score at 1 min after birth
▸ Heart rate during initial evaluation
▸ Oxygen saturation during initial evaluation
▸ Quality of breathing during initial evaluation
Respiratory support
▸ Starting time respiratory support
▸ Indication for respiratory support
▸ Type of respiratory support given
▸ Sustained inflations given
▸ Consecutive inflations given
▸ Pressures used
▸ Pressures adjusted
▸ Effect of respiratory support on heart rate
▸ Effect of respiratory support on oxygen saturation
▸ Duration of respiratory support
Oxygen delivery
▸ Oxygen used
▸ Time of start of oxygen therapy
▸ Indication for oxygen therapy
▸ FiO2
▸ Effect of oxygen therapy
▸ Duration of oxygen therapy
▸ FiO2 titrated during resuscitation
Intubation
▸ Indication for intubation
▸ Tube size
▸ Fixation depth
▸ Number of tries before successful intubation
▸ Difficulty of intubation mentioned
Cardiac resuscitation
▸ Indication for chest compressions
▸ Time of start of chest compressions
▸ Duration of cardiac compressions
▸ Medication given
▸ Indication for medication
▸ Time of medication administration
Transport to NICU
▸ Time of transport to NICU
▸ Type of respiratory support during transport
▸ Ventilatory pressures during transport
▸ FiO2 during transport
Quality of documentation
▸ Use of subjective language* versus objective language in medical record
▸ Use of medical terms versus non-medical terms† in medical record
▸ Apgar scores given by caregiver versus researcher after reviewing video recordings‡
*Subjective language was, for example, good, much, mildly, somewhat, etc.
†Non-medical terms were defined as the usage of non-medical words when a medical synonym or medical description is available.
‡To test the subjectivity of the Apgar score our researcher gave all neonates Apgar scores after reviewing the video recordings (before having seen the Apgar scores given by the caregivers after resuscitation).
NICU, neonatal intensive care unit.
All items were scored as being correctly or incorrectly documented. When correctly documented there were two possibilities: (A) an event occurred and was documented (‘correctly documented’) or (B) an event did not happen and was correctly not documented (‘correctly not documented’), when confirmed by the recording. When incorrectly documented, there were three possibilities: (A) not documented but observed on the recording (‘incorrectly not documented’), (B) documented but not confirmed on the recording (‘incorrectly documented’) and (C) documented but time indication was incorrect. The Apgar score documented by the caregivers after resuscitation was compared with the Apgar score given by the researcher after reviewing the videos, using the standard Apgar score definition. The researcher reviewed the recording before reviewing the medical record and used objective data to score an item if possible (eg, heart rate was scored using the data from the pulse oximetry recording and breathing was evaluated using data from the respiratory function monitor).
Some items could not be observed on the video recordings, for example, umbilical cord pH, time of birth (for anonymity reasons), time of transport to NICU, etc. These items were only scored as being documented or not documented in the medical record.
Statistical analyses
Data were analysed using SPSS (SPSS for Windows, V.20, Chicago, Illinois, USA). Results are presented in frequencies.
Results
During the study period we performed 88 recordings during resuscitation of preterm infants at birth. In 18 recordings, no video was recorded by mistake; parents of two infants were not approached for consent to use the recordings. Thus, 68 recordings were reviewed, but 14 had to be excluded because of poor quality. Recordings of 54 infants could be compared with the medical record, which documented delivery room management in 51 out of 54 (93%). In the other four (7%) delivery room management was not documented. Median (IQR) gestational age was 29 (27–31) weeks and birth weight was 1170 (947–1441) grams, 56% of the included infants were male and 54% were delivered by caesarean section. Time of birth was documented in 25 (46%) medical records. In 23 (43%) infants, an umbilical cord blood gas sample was taken and this was correctly documented in 15/23 (65%) of the medical records.
First impression/evaluation
The clinical condition of the infant upon arrival on the resuscitation table was documented in 41/54 (76%) of the medical records and the 1 min Apgar score in 53/54 (98%) (figure 1). Heart rate was correctly documented in 20/54 (37%) of the medical records, oxygen saturation in 7/54 (13%) and quality of breathing in 33/54 (61%); in most other records numbers or items were not mentioned at all.

First impression of the infant. Quality of documentation of heart rate, oxygen saturation and breathing. Results given as number of medical records (frequencies).
Respiratory support
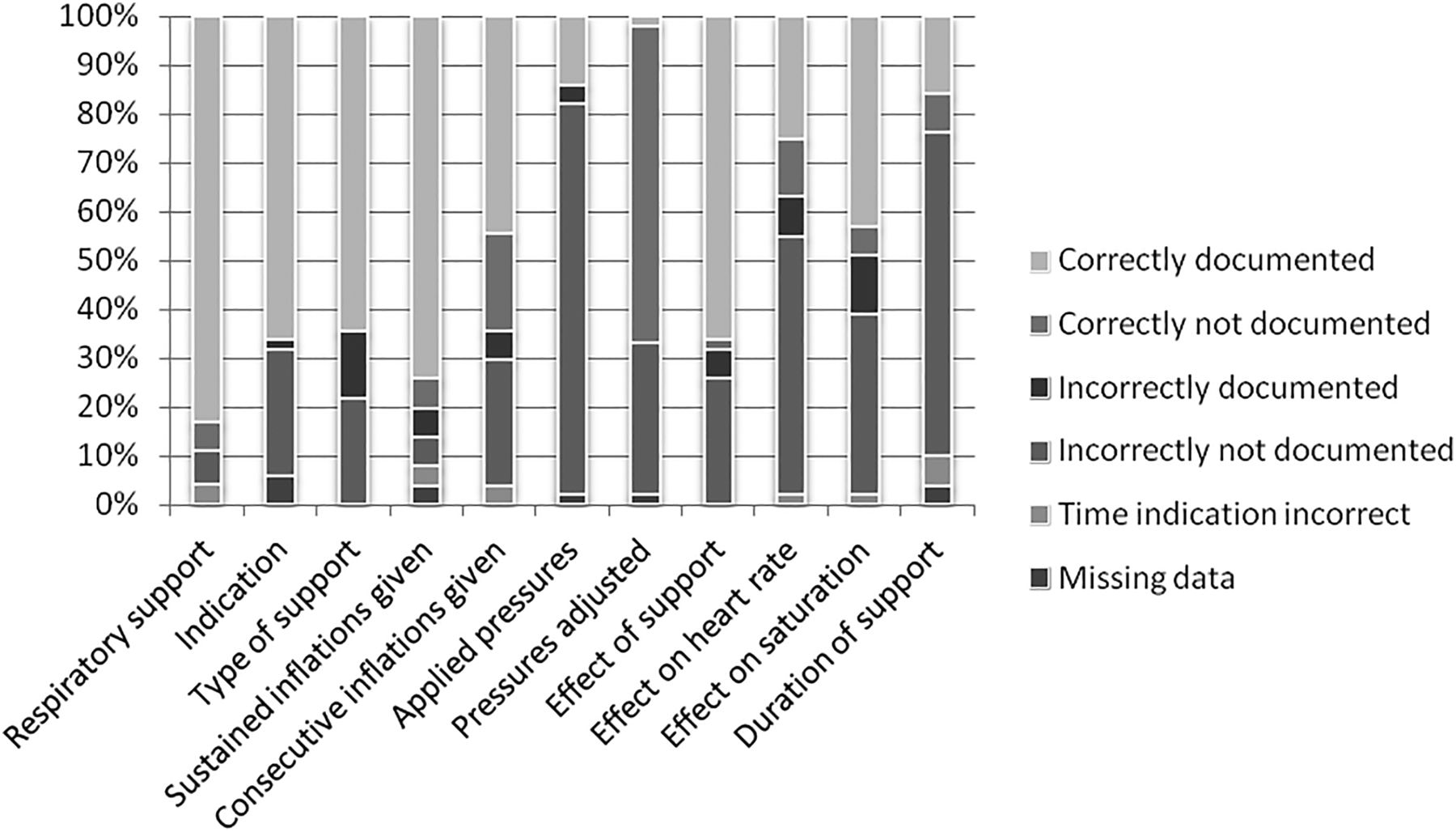
Respiratory support was correctly documented in 45/54 (83%) of the medical records (figure 2). Fifty-one out of 54 patients received respiratory support. The reason for respiratory support was correctly documented in 34/51 (67%) records, the type of respiratory support in 33/51 (65%), whether sustained inflations were given in 38/51 (75%), which pressures were given in 7/51 (14%) and duration of ventilation in 8/51 (16%). The effect of respiratory support was correctly documented in 34/51 (67%) records, the effect on heart rate and oxygen saturation in 13/51 (25%) and 22/51 (43%), respectively.

Respiratory support. Quality of documentation. Results given as number of medical records (frequencies).
Oxygen therapy
In 24 of the 54 recordings, a FiO2 sensor was used and this data could be compared with the documentation in the medical records (figure 3). Twenty-one of these 24 patients received oxygen. In 12/21 (57%) of the records, the use of supplemental oxygen and indication were correctly documented. In 10/21 (48%) records, the maximum level of FiO2 was documented. The starting point of supplemental oxygen delivery was correctly documented in 1/21 (5%), the effect of supplemental oxygen in 6/21 (29%), the duration of supplemental oxygen in 2/21 (10%) and whether FiO2 was titrated in 6/21 (29%).

{kind=link}
{kind=link}
{kind=link}
Oxygen therapy: Quality of documentation. Results given as number of medical records (frequencies).
Intubation
Seven infants were intubated. This was correctly documented in four out of seven (57%) medical records. In one out of seven (14%) the intubation was correctly documented, but the time indication was incorrect. Intubation was not documented in two out of seven (29%) infants. Intubation was documented in one medical record, but this intubation was not observed in the recordings (incorrectly documented). The indication for intubation and tube size and depth were documented in two out of seven (29%) of the medical records. Further details on the procedure (number of attempts, difficulties, etc) were not documented.
Cardiac resuscitation
One infant received cardiac resuscitation and this was correctly documented, including the indication and time indication. The duration of cardiac resuscitation was not documented.
Quality of documentation
One or more subjective medical terms (eg, ‘low heart rate’, ‘pink’) in the documentation of the delivery room management were found in 19/54 (35%) of medical records. One or more non-medical terms (eg, ‘looking bad’) were used in 4/54 (7%). Apgar scores at 1 min, 5 min and 10 min could be scored by the researcher using the recordings of 49, 48 and 34 infants, respectively. At 1 min, 5 min and 10 min the Apgar scores given by the researcher using the recordings were similar to those in the medical records in 33%, 44% and 53% of the infants, respectively. Using the recordings, a higher Apgar score was given by the researcher than the caregivers in 35%, 23% and 6% of the infants with a median (IQR) difference of 2 (1–2), 1 (1–1) and 1 (1–1) points, respectively. A lower Apgar score using the recordings was given in 33%, 33% and 41% of the infants with a median (IQR) difference of 1.5 (−2 to −1), −1 (−2 to −1) and −1 (−1.3 to −1), respectively.
Discussion
Stabilisation or resuscitation of infants at birth is a major part of the daily work of a clinical neonatologist. We observed that documentation of the initial condition of an infant and the procedures in the delivery room often did not correspond with the data from delivery room recordings of physiological parameters and video imaging. The information in the medical records was often incomplete or limited and details were lacking. The anticipated focus of delivery room management is ventilation and we found that the mode of respiratory support was the most accurately documented procedure. However, details about the support provided (applied pressures, duration of ventilation, oxygen therapy) and their efficacy were often lacking or not correct. Medical records are often completed retrospectively and it is difficult to recall all details about the clinical condition of the infant, procedures and their timing. Memories of a stressful past event can be inaccurate.17–19 Stress experienced by caregivers during resuscitation can be a cause of this inaccuracy. It is also possible that a busy workload in the unit often demands concise documentation. However, the observed lacunae in documentation in the medical records make it difficult to evaluate delivery room management.
Previous studies have suggested that resuscitation documentation needs to be improved.4–8 One important reason is to enable accurate and reliable evaluation of neonatal resuscitation practice,6 ,7 but it is also important for legal review of records and to ensure postresuscitation quality of care.4 Thorough documentation is valuable for audit purposes and will, thereby, contribute to the improvement of quality of care.2 ,3 An extra person present during a resuscitation for observing and taking notes could also improve documentation of neonatal resuscitation. However, this would considerably increase the work load of available staff and in most NICUs it is not possible to ensure the 24/7 availability of an extra caregiver for this purpose. In contrast, a recording system that can be switched on whenever needed could make it possible to reach similar quality improvement. Indeed, current available software makes it easy for a caregiver to record physiological parameters concurrent with video imaging.13
In our centre, we use simple preprinted pages to document resuscitation, because studies have shown that this improves documentation in the medical records.8 ,20 In most patients (91%), the preprinted pages were used to document the resuscitation. However, the disadvantages of these preprinted pages are that they ask for general information without details and that there is little space available to write down details. This may have caused the information given to be considered incomplete or limited (table 1). However, the fact that the currently used preprinted pages are filled incompletely, raises the question whether caregivers will provide more details on more elaborate pages.
Information to be documented on the preprinted resuscitation sheets in paper and digital medical records
We have shown in previous studies that recording of physiological parameters and video imaging during neonatal resuscitation can provide the extra details necessary for auditing and educational or research purposes.13 ,14 Here, we have shown that these recordings can be helpful for completing or even correcting the documentation of delivery room management. The recordings do not replace standard documentation, but can be considered complementary. For this purpose, the recordings should become a standard part of the infant's medical records. However, until now the recordings are, after obtaining parental consent, stored anonymously and no copies are made to guarantee the privacy of the patient, parents and caregivers. The video images show only the hands or forearms of the caregivers, the infant and the performed interventions. Due to the anonymous character of the recordings, it is not possible to integrate them into the infant's medical records. A common concern with these kinds of recordings is the potential for recordings to be used for medicolegal purposes. However, we are performing recordings since 4 years and so far there have been no medicolegal issues. Our findings are similar to a previous study reporting that so far no centre has reported such problems.9 On the contrary, we usually offer parents an opportunity to review the recording with us and this has been met with positive responses. Recent studies emphasise the importance of the family being present during procedures.21 ,22 The American Academy of Pediatrics recommends family centred care.23 In the era of family centred care, where the father is present during the resuscitation, we should perhaps aspire that the recordings are identifiable and part of the infants medical record.
In our study, we observed large differences in the Apgar scores given by the caregiver, mostly afterwards, and the Apgar scores given by the researcher when reviewing the recordings. Our findings are in line with previous studies showing that Apgar scores are very subjective parameters with poor interobserver variability.24–27 The researcher could more objectively calculate the Apgar score by using the video and parameters shown on the recordings. In addition, when interventions are needed the given Apgar score also reflects the performance of the caregiver, which could lead to a bias. The researcher was also able to observe the recording more than once and pause the recording to assess the items of the Apgar scores more thoroughly. Only one researcher reviewed the data in our study, which made it impossible to assess interobserver reliability. A future study could be performed with more than one researcher rating the Apgar scores.
This was a retrospective study and bias could have occurred. However, the chances for this are very little as caregivers completed the documentation before the study was formalised and the researcher who evaluated the recordings was not involved in any of the resuscitations. Recordings were performed when a researcher was available and there was time to set up the recording equipment. Although it is possible that a selection bias occurred, it was then by chance that a recording was performed or not. New equipment is now available that is easier to set up and allow all resuscitations to be recorded. Recording equipment always has a small margin of error in their measurements, however, this did not influence the results of this study, because the aim of this study was to report whether events were documented or not.
Conclusion
This study showed that documentation of neonatal resuscitation in the infant's medical records often provides few details on the events that occurred and the performed interventions. High quality documentation is difficult to realise because preprinted resuscitation pages in the medical records ask for few details and the events that occurred during resuscitation are documented in retrospect. Thorough documentation could contribute to the improvement of quality of care. Recording of physiological parameters and video images during neonatal resuscitation can improve documentation as it provides detailed information on neonatal resuscitation. The data from these recordings should therefore be integrated into the infant's medical records.
References
Footnotes
-
Competing interests None.
-
Ethics approval Ethics Review Committee of the Leiden University Medical Center.
-
Provenance and peer review Not commissioned; externally peer reviewed.