Article Text

Abstract
Objective To assess ductus arteriosus (DA) blood flow directly after birth in healthy term infants after elective caesarean section.
Design In healthy term newborns, echocardiography was performed at 2, 5 and 10 min after birth to monitor cardiac output and DA blood flow. Heart rate (HR) was assessed using ECG.
Setting The delivery rooms of the Leiden University Medical Center.
Patients 24 healthy term infants born after a caesarean section were included in this study.
Results Mean (SD) HR did not change (158 (18) beats per minute (bpm), 5 min (159 (23) bpm) and 10 min (156 (19) bpm). DA diameter decreased from 5.2 (1.3) mm at 2 min to 4.6 (1.3) mm at 5 min (p=0.01) to (3.9 (1.2) mm) (p=0.01) at 10 min. Right-to-left DA shunting was unaltered (median (IQR) 95 (64–154) mL/kg/min to 90 (56–168) mL/kg/min and 80 (64–120) mL/kg/min, respectively (ns)), whereas left-to-right shunting significantly increased between 2 and 5 min (41 (31–70) mL/kg/min vs 67 (37–102) mL/kg/min (p=0.01)) and increased significantly between 2 and 10 min (93 (67–125)) mL/kg/min (p<0.001). Right-to-left/left-to-right shunting ratio decreased significantly from 2.1 (1.4–3.1) at 2 min to 1.4 (1.0–1.8) at 5 min (p<0.0001) and to 0.9 (0.6–1.1) at 10 min (p<0.0001).
Conclusions DA shunting changes swiftly from predominantly right-to-left shunting to predominantly left-to-right shunting at 10 min after birth, reflecting differential changes in pulmonary and systemic vascular resistance.
- Neonatology
- neonatal transition
- ductus arteriosus
- left ventricular output
- right ventricular output
Statistics from Altmetric.com
What is already known on this topic
-
Ductus arteriosus flow is known to change from right to left to left to right after birth.
-
Ductus arteriosus flow is dependent on the pressure gradient between the pulmonary and systemic circulations.
What this study adds
-
Ductus arteriosus blood flow changes already within the first 10 min to a predominantly left to right shunt in healthy infants.
-
Ductal flow ratio reflects pulmonary and haemodynamic transition and can be used to monitor neonatal transition.
Introduction
Directly after birth, major changes in the respiratory and cardiovascular systems are required for postnatal survival.1 ,2 This includes ductus arteriosus (DA) closure, a major vascular shunt between the pulmonary and systemic circulation. This closure is preceded by changes in the amount and direction of blood flow through the DA. DA Blood flow is determined by the pressure difference between the pulmonary artery and aorta.3–5 Before birth, high pulmonary vascular resistance (PVR) ensures that blood flows from the right ventricle through the DA and into the systemic circulation (right-to-left (RtoL) shunting) throughout the cardiac cycle. Although blood flows into the lungs briefly during systole, during late systole and throughout diastole blood reflects off the highly resistant pulmonary vasculature and exits the pulmonary circulation across the DA.3–6 This retrograde pulmonary arterial flow causes high diastolic flow through DA in the fetus, as flow in the main pulmonary trunk is zero throughout much of diastole.5 Approximately 90% of right ventricular output (RVO) in the fetus bypasses the lungs and flows across the DA.3
After birth, lung aeration initiates a sudden decrease in PVR, causing the majority of RVO to enter the pulmonary circulation resulting in a large increase in pulmonary blood flow (PBF).3 ,7 ,8 In contrast to PVR, systemic vascular resistance (SVR) increases due to cord clamping.9 With the increase in SVR and decrease in PVR, the pressure gradient across the DA reverses and blood begins to flow from the systemic into the pulmonary circulation (left-to-right (LtoR) shunting).6 ,10 ,11 In lambs, increase in LtoR shunt is responsible for up to 50% of PBF shortly after birth, depending on gestational age.3 However, LtoR flow across the DA is not continuous throughout the cardiac cycle, as RtoL flow occurs briefly during systole and becomes LtoR throughout most of diastole.3
Although in ventilated lambs DA blood flow directly after birth has been described and several studies evaluated ductal flow in neonates during the first hours to days after birth,12–17 little is known about the immediate changes in DA flow in spontaneously breathing infants at birth. Therefore, we aimed to assess DA flow by repeated measurements using Doppler imaging in the first 10 min of life after an elective caesarean section.
Methods
Healthy term infants (≥37 weeks of gestation) delivered by elective caesarean section were included from October 2012 until December 2013. Infants were included after completing enrolment for a previous study that focused on changes in left ventricular dimensions and function directly after birth.18 Parents were approached during preoperation visit or by telephone at least one day before the caesarean section took place. Consent was obtained both verbally en in writing for all patients before the procedure.
For logistical reasons, only infants born after elective caesarean sections were included, as equipment could be prepared in time. Only infants with an uncomplicated transition at birth (eg, no respiratory support necessary) and without congenital malformations were included. A stopwatch was started as soon as the infant was born (ie, when the shoulders were delivered). In accordance with local guidelines, the umbilical cord was clamped 30–60 s after birth and cut by the obstetrician. Therefore, most infants commenced breathing before cord clamping. Thereafter, the baby was placed under a radiant heater and the neonatal caregiver provided standard care (drying, keeping warm, evaluation of the infant's condition). Stimulation, positioning and suctioning only took place when needed. All measurements were collected at three time points after birth: as soon as the infant was placed on the resuscitation table and at 5 and 10 min after birth. During this period, the infant remained on the resuscitation table.
Heart rate (HR) was determined using ECG electrodes (Neotrode II, Conmed, Utica, New York, USA) during the echocardiographic examination. Electrodes were placed as soon as the infant reached the resuscitation table. Oxygen saturation (SpO2) was measured continuously using a Masimo Radical 7 pulse oximeter (Masimo, Irvine, California) with a LCNS Neo-3 sensor (Masimo, Irvine, California) placed preductally.
To assess immediate changes in cardiac output and DA flow after birth, an echocardiographic examination was performed using a Vivid I Cardiovascular Ultrasound system equipped with a 7.0 MHz transducer (GE Healthcare, Waukesha, Wisconsin, USA). Standard two-dimensional (2D) grey-scale images were acquired from the suprasternal, parasternal and apical views and stored in digital format.18 To assess the velocity time integral (VTI), Doppler pulsed wave measurements were obtained in the apical ‘five-chamber’ parasternal long-axis view at the level of the aortic annulus for left ventricular output (LVO) and in the parasternal short-axis view at the level of the pulmonary annulus for RVO. Aortic diameter was measured at the level of the aortic annulus in the parasternal long axis, pulmonary diameter was measured at the level of the pulmonary annulus in the parasternal short axis and diameter of the aortic and pulmonary annulus were measured at each time point.18 The DA was visualised in its long axis from the pulmonary artery and the descending aorta in the suprasternal view. DA diameter (DaDiam) and VTI were assessed using 2D echocardiography and Doppler continuous wave measurements (figure 1). DaDiam was assessed at its smallest part at the pulmonary junction and measured at each time point. Using the continuous wave Doppler measurements, the peak velocity of the RtoL and LtoR shunt was assessed. VTI evaluation of DA flow included analysis of three consecutive flow profiles, providing a mean VTI at each time point for each patient (figure 1).

Examples of ductus arteriosus (DA) blood flow collected using continuous wave Doppler imaging (A and B) showing the left pulmonary artery, right pulmonary artery and DA marked with arrows. (C) DA shunt at 2 min, 5 min and 10 min after birth.
LVO, RVO and DA shunt volume were calculated using the formula (((π × Ann2)/4) × VTI × HR)/birth weight).19 To assess relative differences between RtoL versus LtoR shunting, DA flow ratio was calculated based on VTI measurements (RtoL flow VTI/LtoR flow VTI) for each time point. Also, duration of LtoR and RtoL shunting over the DA was measured and the flow time ratio was calculated.
The study was approved by the Institutional Review Board of the Leiden University Medical Center.
Statistics
Data were analysed using SPSS (IBM, V.20.0.0, Chicago, Illinois, USA). Results are presented as mean (SD), median (range) or median (IQR) where appropriate. Individual data of the three time points were compared using a paired sample t-test for normally distributed data or a Mann–Witney U test for non-normally distributed data. To account for multiple comparisons between the time points, tests were performed using the Bonferroni corrected level (p=0.05/3=0.017). A two-sided p value of <0.05 was regarded as statistically significant.
Results
In 26 newborn infant's, measurements were performed. In two infants, measurements were stopped as respiratory support was necessary and these infants were excluded from analysis. In total, 24 infants were included in this study (median (range) gestational age 39 (37–39) weeks, mean (SD) birth weight 3561 (713) g). Data were collected at 121 (42) s, 5 and 10 min after birth.
HR was not significantly different between 2 min (158 (18) beats per minute (bpm), 5 min (159 (23) bpm) and 10 min (156 (19) bpm). DA diameter decreased from 5.2 (1.3) mm at 2 min to 4.6 (1.3) mm at 5 min (p=0.01) and decreased further to 3.9 (1.2) mm) (p=0.01) at 10 min. Diameter of the aortic and pulmonary annulus did not change between time points. SpO2 increased significantly from 72 (10)% at 2 min to 82 (9) at 5 min (p=0.001) and increased further to 95 (6) at 10 min (p=0.0001).
Right and left ventricular output
No significant difference in RVO was observed within the first 10 min after birth (RVO was 311 (107) at 2 min vs 301 (80) mL/kg/min at 5 min (ns) and 343 (125) mL/kg/min at 10 min (ns)). LVO increased significantly from 165 (50) mL/kg/min to 191 (57) mL/kg (p=0.01) between 2 and 5 min after birth and then increased further to 212 (67) mL/kg/min (p=0.01). Also, LVO increase was significant from 2 to 10 min after birth (p<0.0001).
DA shunting
RtoL DA shunting flow was not significantly different at 2, 5 and 10 min after birth (median (IQR) 95 (64–154) mL/kg/min to 90 (56–168) mL/kg/min and 80 (64–120) mL/kg/min, respectively), although it tended to decrease with time. LtoR shunting increased significantly from 41 (31–70) mL/kg/min to 67 (37–102) mL/kg/min (p=0.01) between 2 and 5 min and then significantly increased to 93 (67–125) mL/kg/min (p<0.001 vs 2 min) at 10 min (figure 2).

Change of ductus arteriosus (DA) LtoR shunting volume (mL/kg/min) (grey) and change of DA RtoL shunting volume (mL/kg/min) (shaded) at 2, 5 and 10 min time points after birth. Box plots show median values (solid black bar), IQR (margins of box) and range of data. *p<0.01, **p<0.001.
Peak velocity was not significantly different between 2, 5 and 10 min for RtoL shunt (0.95 (0.84–1.16), 0.96 (0.89–1.26) and 1.06 (0.95–1.20) m/s, respectively). However, peak velocity of LtoR shunting was significantly different between 2 and 5 min (0.45 (0.37–0.57) vs 0.51 (0.41–0.70) m/s; p<0.05) and between 5 and 10 min (0.51 (0.41–0.70) vs 0.71 (0.62–0.95) m/s; p<0.01).
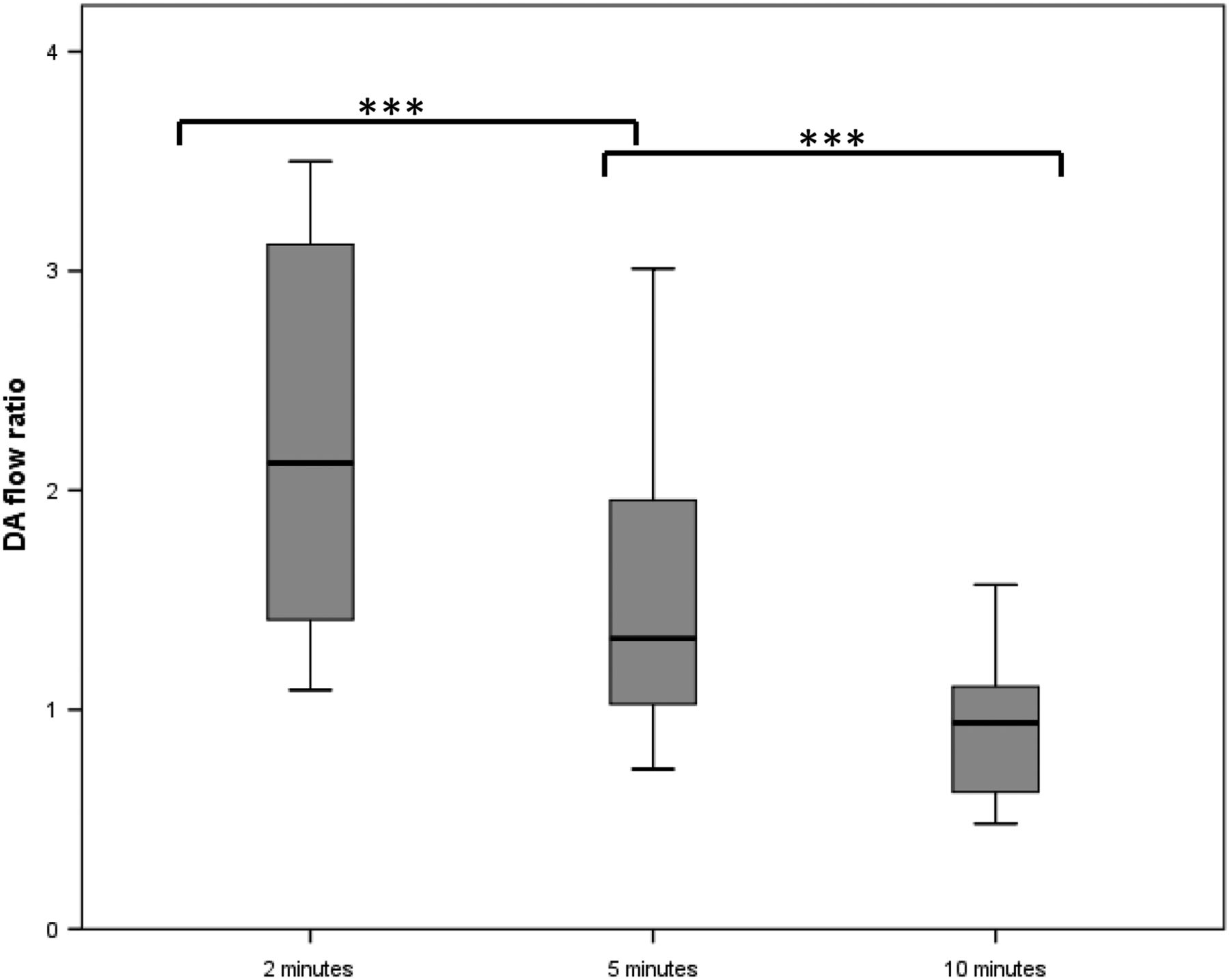
Net difference in DA shunting ((LtoR flow)-(RtoL flow)) increased significantly from −53 (−81 to −17) mL/kg/min at 2 min (ie, predominantly RtoL) to −21 (−45 to −1) mL/kg/min at 5 min (p=0.001) and increased further to 8 (−9 to 33) mL/kg/min (p<0.0001). As a result, flow through the DA at 10 min was predominantly LtoR. DA flow ratio decreased significantly from 2.1 (1.4–3.1) at 2 min to 1.4 (1.0–1.8) at 5 min (p<0.0001) and to 0.9 (0.6–1.1) at 10 min (p<0.0001) (figures 2 and 3). Within a single cardiac cycle, duration of RtoL shunting was similar at 2 and 5 min (159 (25) ms vs 162 (25) ms), but was significantly decreased to 152 (23) ms (p=0.02) at 10 min. LtoR shunting duration significantly increased from 167 (71) to 219 (63) ms (p<0.0001) between 2 and 5 min and increased further to 236 (40) ms (ns) at 10 min. DA flow time ratio significantly decreased from 0.92 (0.71–1.45) to 0.74 (0.59–0.93) (p<0.0001) between 2 and 5 min and then significantly decreased to 0.66 (0.53–0.72) at 10 min (p<0.0001).

{kind=link}
{kind=link}
{kind=link}
Change of ductus arteriosus (DA) flow ratio during 2, 5 and 10 min time points after birth. Box plots show median values (solid black bar), IQR (margins of box) and range of data. ***p<0.0001.
Discussion
This is the first study that presents data on temporal changes in DA blood flow in the first 10 min after birth in human infants. Doppler measurements of DA shunting demonstrated a large increase in LtoR shunting despite decrease in DA diameter. Furthermore, the ratio of RtoL versus LtoR DA flow decreased in a temporal manner after birth, reflecting an overall change from predominantly RtoL to predominantly LtoR shunting in the first minutes after birth. Observed changes in DA flow directly after birth are the expected combined consequences of the decrease in PVR due to lung aeration and increase in SVR due to cord clamping. Decrease in PVR will only occur during pulmonary aeration, and as a result, the ratio of RtoL versus LtoR DA flow could be regarded as an indicator for the cardiopulmonary transition after birth.
Immediately after birth, lung aeration stimulates a large decrease in PVR, which results in a large increase in PBF that, in addition to umbilical cord clamping, is largely responsible for the haemodynamic transition at birth.3 ,5 ,9 ,20–22 Decrease in PVR and increase in SVR reverses the pressure gradient between the pulmonary and systemic circulation,6 ,23 which promotes LtoR DA shunting.17 The increase in LtoR shunting most likely causes an increase in LVO by contributing to PBF and pulmonary venous return leading to increased left ventricular preload.17 The observation that RVO remains relatively unchanged, despite cord clamping, is consistent with findings in lambs when ventilation onset commences before cord clamping.9 Indeed, most infants commenced breathing before cord clamping in this study and therefore the loss in placental venous return is rapidly compensated for. While the mechanisms are unknown, a reversal in blood flow shunting through the foramen ovale (to become predominantly LtoR) after birth is the most likely explanation, although increased systemic venous return is also possible.24
In anaesthetised and ventilated animals, DA blood flow was measured directly after birth.3 ,9 ,22–25 In lambs, it was shown that ventilation resulted in predominantly LtoR DA shunt. Increased oxygenation and cord occlusion, which increases SVR, caused RtoL DA shunting to decrease to negligible levels.23 While net DA flow gradually becomes LtoR within 10 min of birth, the direction of blood flow throughout the cardiac cycle remains very dynamic.3 That is, the flow is RtoL during mid-systole because the pressure wave exiting the right ventricle reaches the pulmonary artery–DA junction before the pressure wave exiting the left ventricle reaches the DA–aorta junction.3 As a result, following the onset of systole, the pressure gradient across the DA is RtoL until the pressure wave from the left ventricle reaches the aortic end of the DA, at which point the pressure gradient reverses causing blood to flow LtoR.3 Our findings show that this also occurs in humans and begins rapidly after birth as significant LtoR flow was present within 2 min of birth. The gradual increase in LtoR DA flow between 2, 5 and 10 min after birth likely reflects both a temporal decrease in PVR and a similar time-related increase in LVO.
In several clinical studies, DA shunting was examined during the neonatal transitional period shortly after birth.12–17 Few have systematically reviewed DA shunting shortly after birth. Noori et al13 performed a prospective observational study and found that at 3–7 min after vaginal delivery, DA shunting is mostly bidirectional and DA flow time ratio was 0.8 (0.9) and net DA flow was 1 (46) mL/kg/min. Our study extends these findings and reports that the duration of LtoR shunting increases significantly from 2 to 10 min after birth, resulting in a significant decrease in DA flow time ratio.
Pulmonary aeration and subsequent decrease in PVR have a profound haemodynamic effect and clearly influence DA shunting.3 Currently parameters of lung aeration and changes in PVR during transition are lacking. DA flow ratio, which takes into account the duration, direction and amount of DA flow, could be useful as it relates pressure changes of the systemic circulation to changes in de pulmonary circulation. When lung aeration and pulmonary transition are disturbed and pulmonary pressure does not decrease, it is likely that DA flow ratio is influenced. Therefore, we speculate that assessment of DA flow ratio could be used for evaluation of the transition.
Limitations
These observations only include term newborns that were scheduled for elective caesarean section and experienced delayed cord clamping. Care should be taken to extrapolate our findings to vaginal deliveries (and preterm born infants), although similar to a study in vaginal births DA LtoR shunting duration increased over time compared with RtoL shunting.13 Our measurements could be influenced by delayed cord clamping9 as the delay of cord clamping could diminish the significant loss of venous return that accompanies cord clamping,3 influencing changes in DA shunt and LVO. Measurement of DA blood flow could vary due to flow turbulence, which lead to incorrect measurements and cause overestimation of blood flow.13 However, in the first minutes after birth, the DA is large and flow velocity is low as is demonstrated by the low-peak velocities reported.13
Conclusion
This study provides new data on haemodynamic changes directly after birth. DA shunting and DA flow ratio changes rapidly after birth, most likely as a consequence of pulmonary aeration and subsequent decrease in PVR along with the increase in SVR. DA blood flow ratio is a direct reflection of pulmonary and haemodynamic transition and could be used in future studies to assess the neonatal transition.
Acknowledgments
We thank MS Verhart for her help with inclusion.
References
Footnotes
-
Contributors JJvV was involved in the design of the study, the acquisition and analysis of data, drafting and writing and revising the manuscript and approving the final version of the manuscript as submitted. ABtP and AAWR were involved in conceptualising and the design of the study, the acquisition of data, drafting and writing and revising the manuscript and approving the final version of the manuscript as submitted. CK-B, JMvL, NAB and SBH were involved in the interpretation of data for the study, writing and revising the manuscript and approving the final version of the manuscript as submitted.
-
Funding ABtP is recipient of a Veni-grant, The Netherlands Organisation for Health Research and Development (ZonMw), part of the Innovational Research Incentives Scheme Veni-Vidi-Vici, project number 91612027. JJvV is recipient of a Willem-Alexander Children's Foundation scholarship.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Commissie Medische Ethiek Leids Universitair Medisch Centrum.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Fantoms