Article Text

Abstract
Objective To assess whether defined reference ranges of oxygen saturation (SpO2) and heart rate (HR) of term infants after birth also apply for infants born after midwifery supervised uncomplicated vaginal birth, where delayed cord clamping (DCC) and immediate skin to skin contact (ISSC) is routine management.
Design Prospective observational study.
Setting and patients Infants born vaginally after uncomplicated birth, that is, no augmentation, maternal pain relief or instrumental delivery.
Interventions Midwives supervising uncomplicated birth at home or in hospital in the Leiden region (The Netherlands) used an oximeter and recorded SpO2 and HR in the first 10 min after birth.
Main outcome measures SpO2 and HR values were compared to the international defined reference ranges.
Results In Leiden, values of 109 infants were obtained and are comparable with previously defined reference ranges, except for a higher SpO2 (p<0.05) combined with a slower increase in the first 3 min. The Leiden cohort also had a lower HR (p<0.05) during the first 10 min with a slower increase in the first 3 min. In the first minutes after birth, tachycardia (HR>180 bpm) occurred less often, and a bradycardia (<80 bpm) more often (p<0.05).
Conclusions Defined reference ranges can be used in infants born after uncomplicated vaginal birth with DCC and ISSC, but higher SpO2 and lower HR were observed in the first minutes.
- pulse oximetry
- umbilical cord clamping
- midwifery
- skin-to-skin contact
Statistics from Altmetric.com
What is already known on this topic
-
Reference ranges of oxygen saturation and heart rate of healthy infants after birth have been defined.
-
For developing the ranges, infants were included where physiological birth was disrupted by augmented labour, analgesia, instrumental vaginal birth or caesarean section.
-
Delayed cord clamping (DCC) and immediate skin to skin contact (ISSC) was not routine management
What this study adds
-
Defined reference ranges can be used for evaluating infants born after uncomplicated birth, but higher SpO2 and lower HR were observed in the first minutes.
-
DCC, ISSC and the absence of medical interventions could explain the differences.
-
Caution should be taken in what we define ‘healthy’, normal transition.
Introduction
Immediately after birth, assessing an infant's condition based on colour is very subjective and not related to oxygen saturation (SpO2) levels.1 Additionally, heart rate is often underestimated by auscultation or palpation.2 The use of pulse oximetry (PO) is recommended in guidelines for evaluating the condition of infants as this offers objective and accurate SpO2 and heart rate (HR) values.3 ,4 Several studies have investigated the normal values of SpO2 and HR of uncompromised term infants receiving no resuscitation.5–10 Recently, Dawson et al6 combined larger observational studies and defined the reference ranges.
The studies used to define the current SpO2 and HR reference ranges included infants where immediate cord clamping was standard policy. However, recent studies indicate that this markedly influences the haemodynamic transition at birth and could have had an effect on the SpO2 and HR levels in the first minutes.6 ,11 Specifically, compared with cord clamping after ventilation onset, immediate cord clamping causes a reduction in HR and cardiac output. Immediate skin to skin contact (ISSC) was also not performed routinely which could have influenced the values as ISSC has been shown to lower stress responses and heart rates in infants.12–16 Also in previous studies, infants were included where physiological birth was disrupted by obstetric interventions such as induced or augmented labour, pain relief (opiates, regional anaesthesia), instrumental delivery or caesarean section.5 ,17 ,18 These interventions could also have caused a delay in transition after birth. It is possible that the defined reference ranges might not reflect the uncomplicated physiological transitional process.
In The Netherlands, almost one-third of women (32.9%) give birth supervised by a community-based midwife. In accordance with the Dutch obstetric indication list, midwives supervise uncomplicated vaginal births at home, in birthing facilities or in hospital.19 In midwifery practice, delayed cord clamping (DCC) and immediate skin to skin contact (ISSC) has been standard care for decades.
Although the benefits of oximetry have been acknowledged by the Royal Dutch College of Midwives, it is undetermined whether the reference ranges are applicable for evaluating term infants after uncomplicated physiological birth where DCC and ISSC is routine management.
In order to assess if previously defined PO reference values are appropriate for evaluating infants born after uncomplicated vaginal births with DCC and ISSC, we compared the SpO2 and HR data from infants born after midwifery-supervised uncomplicated vaginal births (Leiden cohort) with published data from infants born at The Royal Women Hospital, Melbourne, Australia, and at the University Hospital of La Fe, Valencia, Spain (defined reference ranges cohort).6
Methods
A prospective observational study was performed in all seven community-based midwifery practices (27 midwives) in the Leiden region supervising low-risk births at home, birthing facilities or in hospital. Birth occurs without interventions such as induced or augmented labour, pain relief (opiates, regional anesthesia), instrumental delivery or caesarean section. In midwifery practices, DCC is standard care, the cord is clamped after at least 1 min or when pulsations have ceased. Also, immediate skin to skin contact (ISSC) is routine management.
From April 2011 to February 2012, midwives used PO directly after birth for 10 consecutive minutes. We allocated a PO (Masimo RAD- 8, Masimo, Irvine, California) to each midwifery practice; the midwife ‘on call’ had a device at her disposal. The device contained Signal Extraction Technology, SET V.7.8.0.1 software and set to read measurements with 2-second intervals and maximal sensitivity.6 We provided all midwives with a timer, synchronised with the PO to record time of birth and initiation of PO measurements. Midwives were instructed to start the timer at the moment the infant had completely left the mother's body, similar to the defined reference ranges group. By using this timer we could calculate at what time after birth the first measurements were recorded. Midwives were instructed to place a disposable sensor (Masimo Low Noise Cable Sensor (LNCS) New-born Sensor) around the infant's right wrist and then connect the sensor to the pulse oximeter.20 Measurements were obtained for a minimum of 10 consecutive minutes. Midwives were instructed not to let the device interfere with normal procedures, such as DCC and ISSC. Midwives were requested to note basic characteristics, interventions (if needed) and cord clamping time on a prepared evaluation form. We did not specifically ask the midwives to use the provided timer, also a clock present in the room or a watch could be used for timing the cord clamping. Only uncomplicated vaginal births, as previously defined were included.
The PO data were downloaded using Trend com software, providing data points for every two seconds. (http://www.masimo.com) Data with alarm messages (low perfusion, sensor off, ambient light and low signal) were excluded. If in one infant >90% alarm messages were recorded, this particular infant was excluded for analysis. Although we emphasised during training the importance of starting the timer as accurate as possible, it is not possible for the midwives to start the timer exactly at the time of birth. Therefore, for comparison of SpO2 and HR for each minute, we calculated median (IQR) for each minute by using data points –5 s and +5 s around each minute. To calculate percentiles, all valid data points were used, comparable to the LMS-method (the skewness-median coefficient of variation) used for the defined reference ranges.6 ,21 For this reason the median and IQR in the reference ranges figure could be a different number than the calculated median (IQR) using the data points –5 s and +5 s around each minute. Data were imported into IBM SPSS Statistics (V.20.0; IBM Corporation, Armonk, New York, USA). Infant characteristics are presented as numbers and proportions for categorical variables, means and SD for normally distributed continuous variables, and medians and IQR for variables with skewed distribution.6
Differences in minute values of SpO2 and HR between groups were analysed using independent samples t test, data that was not normally distributed was analysed using a 2-tailed Mann–Whitney U test. Statistical significance was considered if p<0.05.
Midwives obtained verbal parental consent prior to the onset of birth. Wall posters and flyers were distributed; midwives informed and subsequently asked parents to participate in the study. Ethical approval was obtained by the medical ethics committee of the Leiden University Medical Center, Leiden, The Netherlands (P.13.155).
Results
During the study period, PO was used on 153 infants. Recordings of 44/153 infants (29%) were excluded for analyses: in 23 infants, no data were stored on the device; in 10 infants, measurements were not obtained during the first 10 min; in eight infants, alarm messages exceeded 90% of the data; and in one infant, the sensor was accidentally placed on the left wrist. In two infants, the midwife in charge felt respiratory support was needed.
Thus, a total of 109/153, (71%) infants were included for analysis. Characteristics are shown in table 1. DCC was applied in all infants, in 45 infants, the time was recorded (table 1).
Infant characteristics of Leiden and defined reference ranges
The amount of data points with alarm message that needed to be excluded was similar in the Leiden group when compared with the defined reference ranges group (SpO2 45% vs 47% data points; HR 46% vs 44% data points). Thus, the final dataset of the first 10 min after birth in the Leiden group contained 14 511 individual infant SpO2 observations and 9686 HR observations from 109 infants, and in the defined reference ranges group 33 119 infant SpO2 observations and 20 318 HR observations from 308 infants. For Spo2 at 1 min, the 10th, 50th, 90th and 95th percentiles were 60, 68, 86 and 86 and for HR 41, 65, 170 and 170 bpm, respectively. At 2 min, 70, 81, 89, and 95 for Spo2 and 54, 81, 184 and 188 bpm for HR, respectively. At 5 min for Spo2 75, 91, 98 and 99, and 129, 152, 168 and 173 for HR, respectively.
Oxygen saturation (SpO2)
The Leiden percentile chart is characterised by higher SpO2, slower rate of rise and a smaller range in the first minutes when compared to the defined reference ranges chart as previously published (figure 1).6 The median SpO2 of the Leiden group was 11, 7 and 4% higher at minute 1, 2 and 3 respectively, but 5, 4, 4, 5, 5, 4 and 2% lower at 4–10 min after birth when compared with the defined reference ranges group (all statistically significant different except at 4 min; table 2). The 10th and 90th percentiles are shown in table 3.
Median (IQR) SpO2 at 1–10 min after birth for Leiden versus defined reference ranges
The 10th and 90th percentiles of SpO2 per minute after birth

Oxygen saturation percentiles of the defined reference range and Leiden cohort.
Heart rate
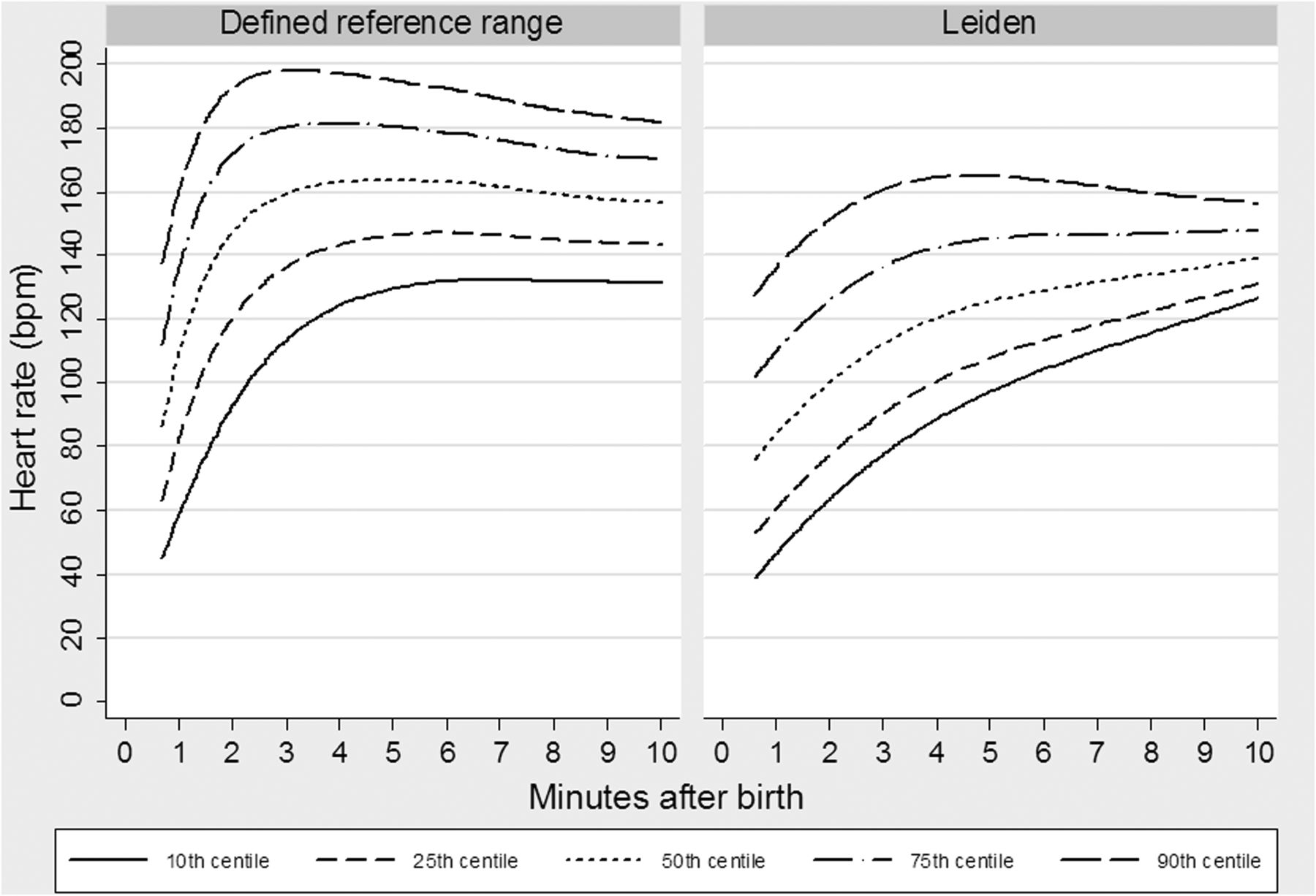
Our findings are characterised by slower rate of rise in the first minutes and a lower HR at all minutes, when compared with the defined reference ranges chart as previously published (figure 2).22 Tachycardia (HR>180 bpm/min) occurred less often in the Leiden group (2.6%) than in the defined reference ranges group (19.3%; p<0.001). For minute 1–10 the percentages of tachycardia were 0, 9, 3, 2, 4, 4, 2, 0, 0, 0% in the Leiden group,and 2, 14, 31, 29, 22, 22, 18, 14, 12, 14% in the defined reference ranges group (all p<0.05 except at 1 min). Bradycardia (HR<80 bpm/min) occurred more frequently in the Leiden group (6.5%) than in the defined reference ranges group (4.8%; p<0.001). For minute 1–10, the percentages were 70, 47, 13, 3, 2, 3, 1, 1, 0, 0% in the Leiden group, and 50, 21, 6, 2, 1, 1, 2, 1, 0, 0% in the defined reference ranges group (not significant, except at 1, 2, 3 and 6 min p<0.05).
The median HR of the Leiden group was 19, 75, 10, 18, 17, 14, 10, 13, 7, 12 bpm lower for 1–10 min after birth when compared to the defined reference ranges group (all p<0.001, except at 1 min; table 4). The 10th and 90th percentiles are shown in table 5.
Median (IQR) heart rate (HR) per minute after birth of Leiden versus defined reference ranges
The 10th and 90th percentiles of heart rate (HR) per minute

{kind=link}
{kind=link}
Heart rate percentiles of the defined reference range and Leiden cohort.
Discussion
In this study, we collected SpO2 and HR values from infants after uncomplicated vaginal birth with DCC and ISSC, and compared the measurements with the cohort of infants who were used to define the current reference ranges. However, this cohort of infants included infants who received medical intervention, immediate clamping and ISSC was not routine.6 Median SpO2 values in the Leiden group were higher in the very first minutes, but median HRs were lower at all time-points compared to the defined ranges. Considering the fact that it has been recommended to accept values down to the 10th percentile, the differences in the 10th percentile in the first 3 min (higher in SpO2 and lower in HR) is noteworthy.18 These observations could imply that caution should be taken in accepting lower levels of SpO2 and HR as ‘normal transition’ of healthy term infants.
Several studies report SpO2 values in term infants after birth.5 ,9 ,10 ,12 ,20 ,23 This is the first study solely describing infants born after uncomplicated birth with DCC and ISSC. Although the SpO2 in our group was within the range of acceptable levels, the large amount of data points led to significant differences at almost all time points. The largest difference was observed within the first 3 min with a higher SpO2 in the Leiden group, followed by smaller differences in SpO2 that were lower than the previously defined range. This resulted in a lower rate of rise in SpO2 in our group compared with the defined ranges.
By contrast with the defined reference ranges cohort, DCC is common practice for midwives in The Netherlands. A recent study in preterm lambs showed that DCC is beneficial for the cardiovascular transition, which leads to greater cardiovascular stability.11 DCC allows time for infants to breathe and increase their pulmonary blood flow so that when the cord is cut, the source of preload for the left ventricle can immediately switch from placental venous return to pulmonary venous return, thereby maintaining left ventricular output. By contrast, cutting the cord before pulmonary transition has started, leads to a sudden loss in preload and a decrease in left ventricular output until ventilation commences.11 It is likely that cardiovascular stability leads to an improved tissue perfusion, which plays an important part in the benefits of delayed cord clamping (lower incidence of NEC and IVH)24 and could also explain the observed higher SpO2 levels in the first minutes after birth in our cohort. Additionally, the fact that the Leiden group was more homogenous could contribute to the observed differences as the defined reference ranges are based on a heterogeneous group (augmented labour; eg, pain relief, instrumental delivery or caesarean section). Interventions during birth could have induced a response within the infant that altered its transition during the very first minutes, even though these infants did not require additional support. Indeed, studies have shown lower SpO2 levels in the first 5 min after caesarean section, compared to vaginal delivery.5 ,6 ,9 ,17 ,25–28 Although medical obstetric pain relief (combined spinal epidural, inhaled analgesia and opioids) showed no adverse effect on the Apgar score and NICU admission, these interventions could alter the physiological transition at birth, thereby influencing the SpO2 and HR after birth.29–31
Other different physiological processes may be involved as well. Seventy-five percent of women in The Netherlands initiate breastfeeding after birth.32 Although we did not record this, it is likely that a substantial number of infants were breastfed at time of pulse oximetry measurements, which is known to influence HR and SpO2 levels.16 ,33 Indeed, feeding (bottle and breast) is acknowledged to interrupt ventilation and increase oxygen consumption, so the lower SpO2 levels during the latter part of the study period may simply reflect the fact that more of these infants were feeding. These practices were not common in infants included in the defined reference ranges group.
The lower HR in vigorous infants in the first minutes after birth is not a new finding, and has been described before.6 ,22 However, the lower heart rate in our cohort when compared with the cohort of the defined ranges was in contrast to what we expected when considering the effect of DCC. In a recent animal study, a reduction in HR (40%) was observed when the cord was clamped before ventilation, while in the lambs that were ventilated before cord clamping had a smaller decrease in HR.11 Although other factors (see below) could explain the observed lower HR, it is still possible that DCC could have contributed. DCC prevents a sudden loss in preload and decrease in left ventricular stroke volume and, therefore, there is less need to compensate this with HR to maintain left ventricular output.11 Further studies are needed, but we speculate that, in the Leiden group, DCC contributed to the lower incidence of tachycardia and the lower rate of HR rise compared with the defined reference ranges group.
Another possible explanation for the lower heart rates in the first minutes, lower rate of rise and less frequent tachycardia is that all infants in the Leiden group were subjected to ISSC. Various studies report positive effects of ISSC; it reduces the amount of crying and infants maintain higher skin temperature.13 ,33 Also, infants exposed to ISSC have a lower mean HR and respiratory rate after birth compared to those not subjected to ISSC.12 ,14 ,15 Similarly, lower cortisol levels at 60 min after birth were found in newborn infants immediately placed prone on the mother's bare chest. A lower cortisol level likely reflects a reduced stress response and an associated reduced sympathetic drive for increased HR.14–16
Interestingly, the median Apgar score at 1 min was higher and in discrepancy to the recorded median heart rate and oxygen saturation at 1 min. The midwives did not use the measured values for calculating the Apgar score, but only used their clinical evaluation and in vigorous infants the heart rate is often not counted Our study group was smaller when compared with the study group on which the defined ranges were based (109 vs 308 infants), and consequently, less data points could have influenced the observed variation. However, the amount of data points per infant was similar in both groups as well as the percentage of validated data points.6
More than half the infants (54%) in our study were born at home, and in this setting the midwife operates alone. Although we emphasised the importance of starting the timer as accurately as possible, and the midwives were dedicated, it is possible that the time of birth was not recorded to the precise second. For the percentiles, all data points were used (figures 1–2). The possibility that in the Leiden group the time of birth was earlier than recorded could explain the higher SpO2 levels in the first minutes, but the observed lower heart rates makes this unlikely. It can be difficult to get reliable recordings in the very first minutes, and fewer infants were included for analysis. However, the percentage of infants included in our cohort was similar to the cohort of the defined reference ranges.
In conclusion, the reference values can be used for evaluating term infants after uncomplicated birth with DCC and ISSC. Caution, however, should be taken in what we define ‘healthy’, normal transition and which lower levels we find acceptable. DCC, ISSC and the absence of medical interventions could explain the observed differences. Future studies are needed to identify which ranges in heart rate and oxygen saturation can be considered normal and how the different factors influence these parameters.
Acknowledgments
We would like to thank the midwives in Leiden region for participating in this study and providing us with the necessary data. We are very grateful to all parents who allowed the midwife to take measurements on their newborn. We thank Raul Bénis of Masimo Corporation for his technical support during the study period.
References
Footnotes
-
Contributors MS conceptualised and designed the study, performed statistical analyses, and wrote the manuscript. JAD shared her experience on performing pulse oximetry studies, advised on the design, performed analyses and critically reviewed the manuscript and approved the final manuscript as submitted. AG codesigned the study, enrolled the pulse oximeter measurement strategy, collected data from the devices, performed initial analyses and critically reviewed the manuscript. BH critically reviewed the manuscript and advised on physiological theories. JvR and SBH critically reviewed the manuscript. ABtP conceptualised and designed the study, has written the study protocol and obtained permission by the medical ethics committee. ABtP supervised the analysis and writing of the manuscript, critically reviewed the manuscript.
-
Competing interests ABtP is recipient of a Veni-grant, The Netherlands organisation for Health Research and Development (ZonMw), part of the Innovational Research Incentives Scheme Veni-Vidi-Vici, project number 91612027. Masimo Corporation (Masimo, Irvine, California, USA) supplied pulse oximeter devices for the length of this study.
-
Ethics approval Leiden Medical Ethics Board, Leiden, The Netherlands
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Fantoms