Article Text

Abstract
Objective Neonatal organ donation does not occur in the UK. Unlike in other European countries, Australasia and the USA death verification/certification standards effectively prohibit use of neurological criteria for diagnosing death in infants between 37 weeks’ gestation and 2 months of age and therefore donation after neurological determination of death. Neonatal donation after circulatory definition of death is also possible but is not currently undertaken. There is currently no specific information about the potential neonatal organ donation in the UK; this study provides this in one tertiary children's hospital.
Design Retrospective mortality database, clinical document database and patient notes review.
Setting Neonatal and Paediatric Intensive Care in a tertiary children's hospital.
Patients Infants dying between 37 weeks’ gestation and 2 months of age between 1 January 2006 and 31 October 2012. Potential assessed using current UK guidelines for older children and neonatal criteria elsewhere.
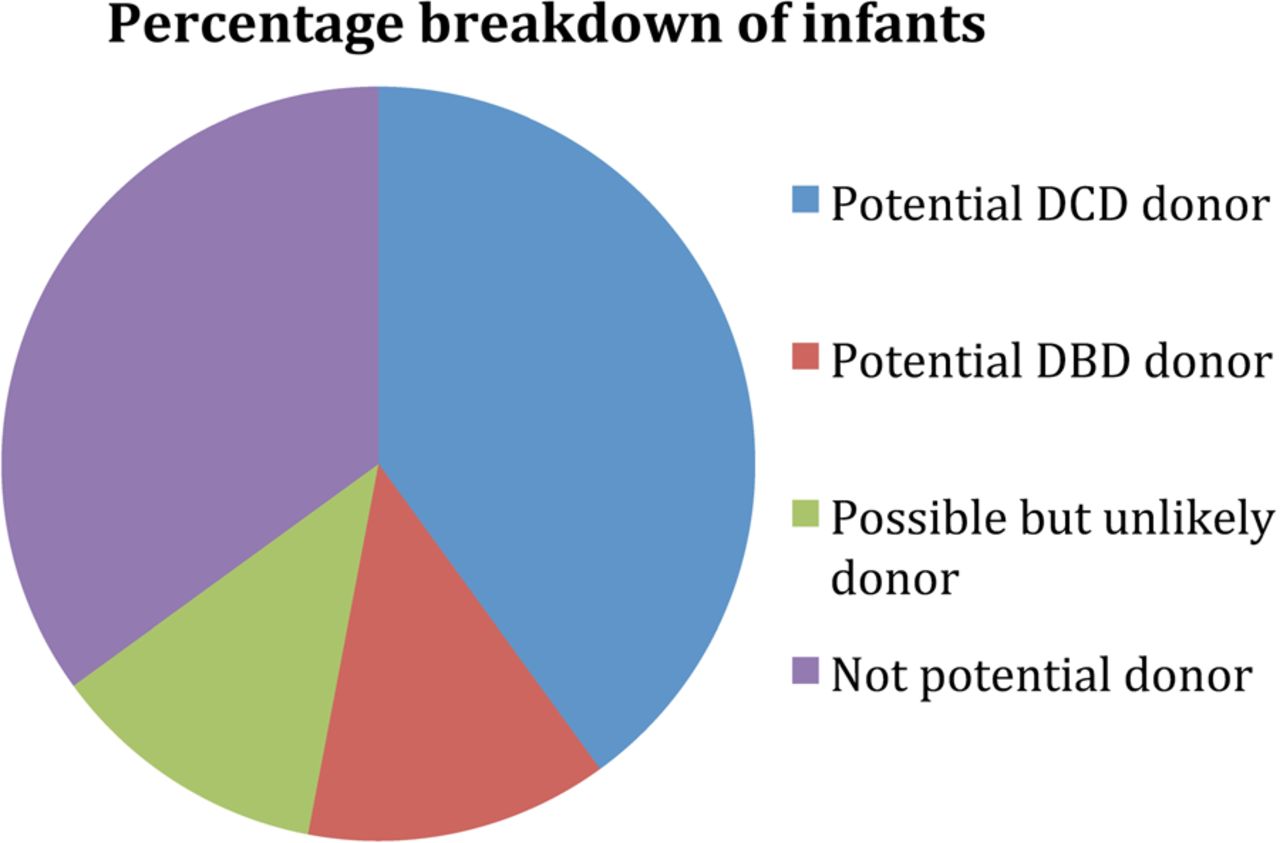
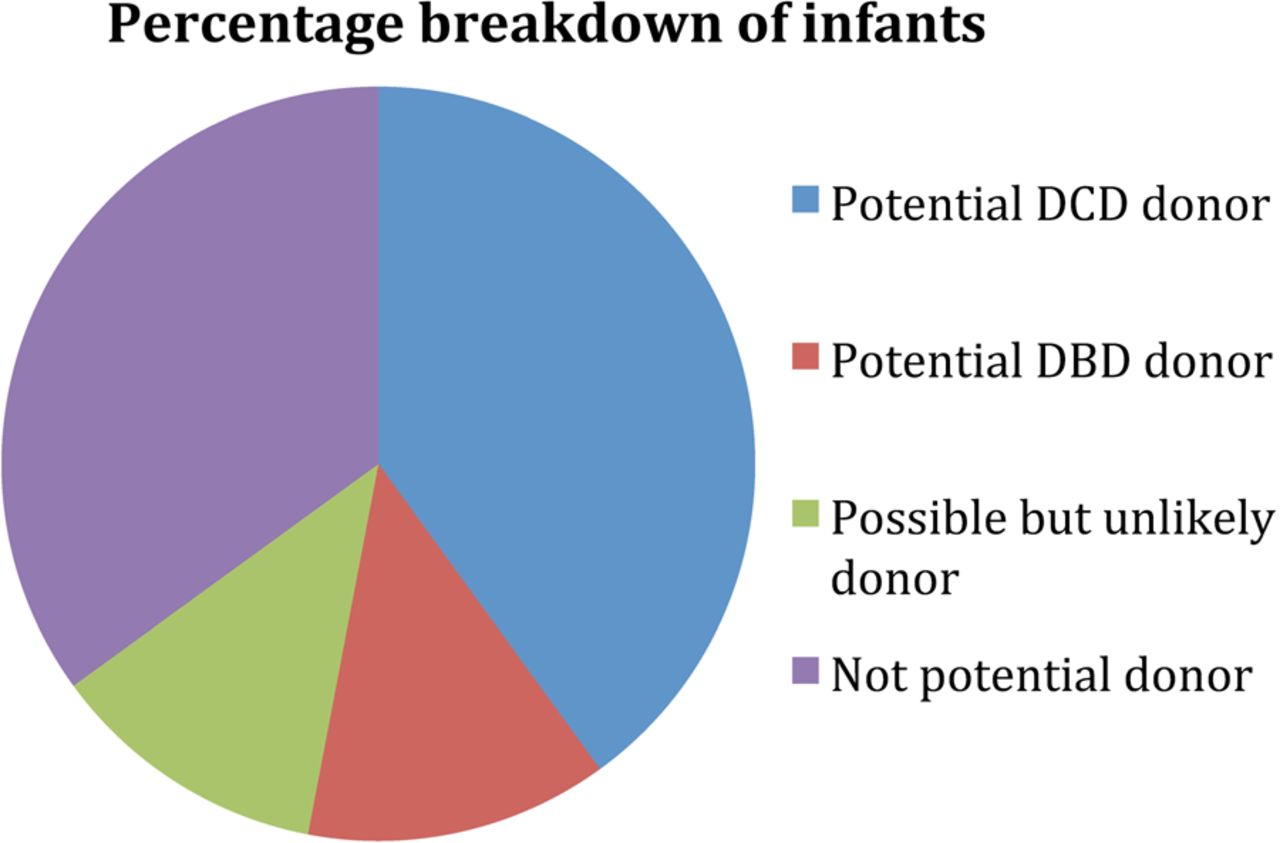
Results 84 infants died with 45 (54%) identified as potential donors. 34 (40%) were identified as potential donors after circulatory definition of death and 11 (13%) were identified as being theoretical potential donors after neurological determination of death. 10 (12%) were identified as unlikely donors due to relative contraindications and 39 (46%) were definitely not potential donors.
Conclusions With around 60 paediatric organ donors in the UK annually, there does appear significant potential for donation within the neonatal population. Reconsideration of current infant brain stem death guidelines is required to allow parents the opportunity of donation after neurological determination of death, together with mandatory training in organ donation for neonatal teams, which will also facilitate donation after circulatory definition of death.
- Neonatology
- Ethics
- Mortality
- Intensive Care
Statistics from Altmetric.com
What is already known
-
In the UK infants under 2 months of age have yet to donate organs.
-
Donation after circulatory determination of death (DCDD), while possible, has not occurred under 2 months of age.
-
Donation following neurological determination of death (DNDD) from UK infants less 2 months of age is precluded by guidelines on death certification, unlike in many other countries where bereaved families can donate.
What this study adds
-
There is significant potential for donation among the UK neonatal population that is not being realized.
-
This potential could be realised by review of current guidelines relating to neurological criteria for death certification, and training for those working in NICU.
Between 2001 and 2006, 414 children were organ donors in the UK and Ireland and 1104 children received transplanted organs.1 Excluding living donor transplants, some cadaveric adult organs donated are transplanted into children, either of larger size or after graft reduction/splitting. However, several of the organs donated by the approximately 60 children donors each year are transplanted into adult patients.
Although there are fewer infants and children on the waiting list compared to adults, there are also usually far fewer potential donors for any child. This is due to both differences in donor size and to the scarcity of paediatric donation.2 For an infant awaiting a heart transplant, only a small-sized infant organ can be used, whereas as children approach adolescence an adult organ becomes a viable option. For those neonates and infants that might benefit from transplantation, this size issue is an important limitation on the chance of transplantation, but in the UK it is sadly not the only restricting factor.
For the last 10 years 4–8% of UK organ donors have been under 18 years of age. However, infants under the age of 2 months have yet to donate organs in the UK.3 This is in contrast to other developed countries where donation in this age group can, and does, take place. In a situation in which organs are scarce and demand is high it is arguable that all potential sources of organ donation should be fully considered. The reasons behind this will be discussed, but it is useful to understand that the situation is so bizarre that occasionally donated organs from Europe are transplanted into UK infants, whereas no reciprocal transplantation is ever undertaken.4
Deceased organ donation can occur in two ways:
-
Donation following neurological determination of death (DNDD) occurs after the certification of death using neurological criteria on a fully supported intensive care patient, and has previously been termed donation after brain death.
-
Donation after circulatory determination of death (DCDD) occurs after the certification of death using cardiorespiratory criteria, usually following the withdrawal of intensive organ support and had previously been termed non-heart-beating donation and donation after circulatory death.
In both cases organ retrieval teams from transplant centres attend the hospital where the donor is, to retrieve organs back to their own centres for transplantation. There is, therefore, no need for specialist transplant expertise in donating units but every UK Trust does have a mandatory Specialist Nurse in Organ Donation (SNOD) and Clinical Lead in Organ Donation (CLOD), often an intensivist, whose role is to facilitate donation from the intensive care units (ICUs) and occasionally emergency departments of their Trust.
Traditionally most organs donated for transplantation, whether from adults or children, have been DNDD. However, the shortage of organs has recently resulted in an increase in DCDD, which is now standard practice in UK PICU.5
While DNDD organs have traditionally been preferred by transplant teams due to decreased ischaemic time—because organ harvest occurs from an intact circulation—recent DCDD transplant data suggest that there can sometimes be comparable long-term follow-up.6
DNDD in those under 2 months of age is basically precluded in the UK by AOMRC national guidelines,7 which suggest it is ‘rarely possible to confirm death using neurological criteria in infants under 2 months of age’, although this is practiced in the USA, Europe and Australia.
Although DCDD is possible in this age group, it does not happen currently. There are limited worldwide data on successful outcomes of infant DCDD transplantation; however, successful cardiac transplantation has been undertaken at one centre in the US,8 albeit with significant ethical debate.9 UK cardiac transplant teams are seeking to replicate this, and other transplant teams have shown interest in liver/hepatocyte donation and renal transplant.
Unlike in the adult population DCDD in children is currently limited to donation after death following elective withdrawal of life-sustaining therapy. For donation to be successful the warm ischaemic time undergone by the organs during the child's dying and the interval after death before retrieval needs to be compatible with successful transplantation. This varies by organ type, and the ischaemic time before cessation of circulation and can be up to 3 h postcirculatory arrest for successful kidney transplantation. The standard minimum time before organ harvest after circulatory arrest is 5 min, as per national guidelines for verification of death.7 Attempts in the US to reduce this time—to as little as 90 s, to facilitate cardiac retrieval from infants, caused controversy.9
Indeed, this entire area undoubtedly raises a number of ethical and emotive issues. In the US there has been a recent call for a full moratorium on DCDD in children;10 however, a recent American Academy of Paediatric Bioethics Policy Statement has supported the entire process, as long as it is undertaken in an ethically rigorous manner.11
It is suggested that one of the most significant barriers to consideration of donation among this age group is the fact that debates about the possibility of neonatal organ donation are currently hindered by a distinct lack of data. Indeed, it is very difficult to have proper discussion about organ donation in any age group without data that quantify in real numbers the potential for organ donation under discussion.
Although there are data that looks at the potential for DCDD in the UK paediatric population,12 there are currently little data on the potential contribution of infant donors. One study in the US looked at the potential contribution of infant DCDD donors and found that from 57 deaths included 11 were potential organ donors.13 While such research is promising, this is the only study of its kind and no such data exist in the UK.
The aim of this study was therefore to attempt to estimate the potential for organ donation specifically among infants in the UK with the hope that such data will promote and facilitate the consideration of infants as a potential source of organs. This will involve an estimate of the potential that is currently possible but not being achieved in terms of DCDD but also to give an estimate of the potential for DNDD that could in theory be possible if it was not for the guidelines mentioned above.
Design
Great Ormond Street Hospital is a tertiary/quaternary paediatric hospital. The Paediatric and Neonatal intensive care unit (PICU/NICU) is the lead centre for PICU in North Thames and the ICUs are part of a specialist neurosciences unit, which is relevant because infants are admitted for specialist neurovascular interventions and neurosurgery.
We identified all infants who died on the NICU or PICU between 1 January 2006 and 31 October 2012 inclusively and undertook a retrospective review of the neonatal and paediatric intensive care mortality database and the clinical document database to ascertain whether each patient may have been considered a potential DCDD donor and whether they could have, in theory, fulfilled the criteria for neurological death enabling them to be considered as potential DNDD donors. Evidence to suggest the later may have become possible included isoelectric EEG, apnoea when sedation discontinued and fixed and dilated pupils. However, no sustained or repeated examination was made as would be required in formal neurological determination of death as undertaken in countries permitting this in infants.14
Data collected included the infants’ age, sex, mode of death, contraindications to organ donation and fulfilment of neurological criteria for the determination of death as applied to children over 2 months age.
Our exclusion criteria were as follows:
-
Age <37 weeks’ gestation and >2 months. Premature infants ages were calculated based on corrected gestational age
-
Patients whose mode of death did not follow active withdrawal of treatment. This included infants dying as a result of failed cardiopulmonary resuscitation as donation is unlikely to be a viable option in these circumstances, as in older children.
-
Patients who had absolute contraindications to donation (haematological malignancy, multisystem disease such as a mitochondrial/metabolic condition)
-
Infants dying on the cardiac/congenital heart unit. These patients were excluded from NHS Blood and Transplant (NHSBT) potential donor audits, and the unit ran separately, at the time of the study.
Patients who had relative contraindications to donation (untreated systemic infection) were identified and separately classified as possible but unlikely donors.
Results
During the study period, 84 infants aged between 37 weeks’ gestation and 2 months died in the PICU/NICU at Great Ormond Street Hospital with 45 (54%) were identified as being potential overall donors. Thirty-four (40%) infants were identified as being potential DCDD donors all having intensive organ support withdrawn in their best interests with parental consent—usually with severe brain injury and additional ongoing irreversible organ system dysfunction. All died within 3 h and most within minutes of withdrawal. For 30 infants death was verified within 1 hour of the withdrawal of life-sustaining therapy, for the other four time of verification of death was unclear, but from prescription of drugs and infusions would appear to be within 3 h of withdrawal.
Eleven (13%) infants were categorised as potential DNDD donors. All these children had catastrophic brain injury with a specific diagnostic cause of coma, evidence of apnoea and brainstem dysfunction—for example, fixed and dilated pupils—but no formal examination compatible with neurological a determination of death was undertaken. All infants died within minutes of withdrawal of invasive organ support (table 1).
Infants identified as potential DNDD donors by Paediatric Specialist Nurse in Organ Donation (AS)
Ten (12%) infants were identified as being possible, but unlikely, potential donors due to relative contraindications. All of these infants were possible DCDD donors.
A further 29 (35%) were identified as not being potential donors either because they did not have intensive care withdrawn or because there were absolute contraindications to donation, such as malignancy or undiagnosed metabolic disease (figure 1).
{kind=link}
Pie chart showing percentage breakdown of infants as donors/non-donors.
Discussion
These results suggest a significant proportion of neonates who died in one children's hospital were potential organ donors. In the context of an annual total paediatric donor number of around 50–605 even with a conservative conversion rate of 50%, these organs would significantly increase the overall total of small-sized organs donated in the UK. This is especially important as for many potential recipients there are so few organs of this size being donated that they are not currently being listed for transplantation.
Clearly, further consideration of this age group as a source of organs for transplantation is warranted.
In our population infants classified as potential DNDD donors had suffered catastrophic brain injury and had clinical features, which suggested that their death might have been able to be certified using neurological criteria, if this were possible in the UK. Essentially all these infants had fixed and dilated pupils and were apnoeic when respiratory system assessment was made before withdrawal. However, no formal brain stem reflexes, or accessory tests that might be used to confirm brain death were undertaken—either for this purpose or for the purpose of the study. It is, however, reasonable to state that all of those in the DNDD group with complex intracranial vascular disease—for example, Vein of Galen anomaly—who underwent cerebral blood flow studies (n=4) in the form of CT/MR/interventional angiograms had absent blood flow/perfusion.
The infants classified as potential DCDD donors had intensive care organ support withdrawn in their best interests, in accordance with the Royal College of Child Health's Withdrawal and Withholding of Life-Sustaining Therapy guidance.15 In all cases there was consensus between medical teams and the family. All infants died within 3 h, with 30 dying within 1 h, of the withdrawal of life-sustaining therapy. However, there was no more specific information about the timing of death after withdrawal. ‘Terminal weaning’ is not the standard of care in PICU,16 and in most cases all invasive organ support—including invasive ventilation, inotropes, nitric oxide and occasionally renal replacement therapy—was stopped. All babies were maintained on sedation and analgesia. Those infants who died following a ‘one-way-wean’ of invasive support, considered to be no longer beneficial, also had sedation weaned to enable a period of assessment after extubation and possible survival, but were classified as not potential donors.
While the number of families who might have consented is impossible to know, even a 50% consent rate would transform infant organ transplantation in the UK.
Which organs could be donated?
Neonatal DNDD donation has traditionally provided a source for cardiac transplantation worldwide. However, other potential recipients for neonatal organ donation are emerging with interest in en bloc renal transplant into adults17 and children18 recipients being explored. Other DNDD infant organs successfully transplanted in the US include kidney alone, heart–lung, liver–kidney–pancreas–intestine, liver alone, lung alone and liver–intestine (United Network for Organ Sharing).
Successful cardiac transplantation from infants whose death has been certified using cardiorespiratory criteria has been undertaken recently in one US centre,8 but has yet to be replicated elsewhere. However, following UK Donation Ethics Committee meetings on this topic and subsequent meetings about ante-mortem interventions such as heparin administration to those donating, this might soon be feasible in the UK, though remains controversial.19 Clarification remains necessary about the legality of ante-mortem heparin administration to a donor—which transplant teams feel is necessary; however, an already anticoagulated infant might offer viable cardiac DCDD in the near future.
Hepatocyte and liver transplantation from neonatal donors is currently technically possible,20 as indeed is successful multivisceral neonatal donation.21
The proportion of potential donors in this study is higher than reported elsewhere. In a study of three Boston hospitals 16% of neonates were identified as potential donors in theory and this was then further reduced to 8% when real factors such as warm ischaemic time were taken into consideration.13 Our retrospective study could not specifically review warm ischaemic times, as UK practice is not to determine the specific time an infant becomes asystolic or indeed is potentially certifiable as having died, but to leave the infant with the family and to certify death which seems appropriate to those attending. Therefore it is possible that some infants might not have been able to donate due to prolonged warm ischaemic time—though as those infants undergoing a ‘one-way-wean’ of invasive support were excluded, this clinical group tend to be rapidly apnoeic and asystolic on withdrawal of aggressive life-sustaining treatment.
Thus, while the results of this study provide a broad estimate of the potential donation in the units, it is likely that in practice the figures would be lower when all factors were taken into consideration.
Despite this, there is clearly significant potential for organ donation that is currently not being considered in units such as that studied, and almost certainly potential within all NICUs. Expertise in redirecting care to excellent palliative treatments is available throughout the UK NICU community, and training with the local Specialist Nurses in Organ Donation present in every Trust –especially in level 3 units—together with the provision of standardised national pathways could facilitate donation in those rare instances where it might be offered to bereaved families.
Family grief and bereavement is improved in those who have donated a dying relative's organs,22 furthermore the majority of the UK population supports donation.23 It is surely time to consider offering families the opportunity of donating their dying infant's organs, where possible, during neonatal end of life care?
The fact that 13% of the neonates could have theoretically fulfilled the criteria for ‘brain stem death’ suggests that current guidelines are preventing consideration of suitable donors in the UK. These results call into question the validity of such guidelines, particularly when they are at odds with other modern healthcare systems such as those of the USA, France and Australia. Review of these guidelines could increase the donor numbers in the UK and remove the need to turn to Europe for the provision of neonatal hearts, as is the current practice.
Limitations
Seventeen infants were unable to be assessed because sufficient information could not be found to ascertain their suitability for donation. Furthermore, as this was retrospective non-interventional study no specific information about mode of death—other than that recorded for routine care in the data systems—was available. A prospective observational study of the actual mode of dying of infants in ICU would be necessary to give categorical information about donor potential.
This is single-centre study from a tertiary children's specialist neurosciences centre—and therefore the results are unlikely to be generalised across the UK. The unit in question is a National neurovascular centre admitting infants with a high risk of severe brain ischaemia, such as those with Vein of Galen malformation. Irrespective of this, this study identifies significant potential donors in an area in which transplantation only sporadically occurs.
Summary
While undertaken in a specialist neuroscience centre, this study has demonstrated significant potential organ donation in a UK neonatal unit. Clearly there is similar unrealised potential in similar centres, and almost certainly some potential in most units. The total possible beneficiaries are unknown as infants are not currently listed.
Neonatal donation following death certified using neurological criteria requires alteration of current professional guidance in the UK, which will soon be addressed. This will enable the families of infants dying in appropriate circumstances to donate their child's organs to others.
However, donation after cardiorespiratory certification of death is currently possible—although antenatal interventions such as anticoagulant administration to facilitate heart transplantation require further legal clarification. DCDD can yield other organs from small infants, albeit sometimes with adult recipients—but surely this is an option, which ought to be offered to families.
References
Footnotes
-
Contributors AS and JB conceived and designed the work. EC collected the data, which all three authors analysed and interpreted. EC drafted the manuscript, which all three authors have revised. All three authors have given final approval of the version to be published.
-
Competing interests None.
-
Ethics approval Registered as audit with Great Ormond St NHS Trust.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement The database can be made available with appropriate permissions.