Article Text

Abstract
Objective The 2010 ILCOR neonatal resuscitation guidelines do not specify appropriate inflation times for the initial lung inflations in apnoeic newborn infants. The authors compared three ventilation strategies immediately after delivery in asphyxiated newborn lambs.
Design Experimental animal study.
Setting Facility for animal research.
Subjects Eighteen near-term lambs (weight 3.5–3.9 kg) delivered by caesarean section.
Interventions Asphyxia was induced by occluding the umbilical cord and delaying ventilation onset (10–11 min) until mean carotid blood pressure (CBP) was ≤22 mm Hg. Animals were divided into three groups (n=6) and ventilation started with: (1) inflation times of 0.5 s at a ventilation rate 60/min, (2) five 3 s inflations or (3) a single 30 s inflation. Subsequent ventilation used inflations at 0.5 s at 60/min for all groups.
Main outcome measures Times to reach a heart rate (HR) of 120 bpm and a mean CBP of 40 mm Hg. Secondary outcome was change in lung compliance.
Results Median time to reach HR 120 bpm and mean CBP 40 mm Hg was significantly shorter in the single 30 s inflation group (8 s and 74 s) versus the 5×3 s inflation group (38 s and 466 s) and the conventional ventilation group (64 s and 264 s). Lung compliance was significantly better in the single 30 s inflation group.
Conclusion A single sustained inflation of 30 s immediately after birth improved speed of circulatory recovery and lung compliance in near-term asphyxiated lambs. This approach for neonatal resuscitation merits further investigation.
Statistics from Altmetric.com
What is already known on this topic
-
Current resuscitation guidelines state that both short and long inflation times may be used for the establishment of initial lung inflation
-
Sustained inflations may improve functional residual capacity by allowing an appropriate time-constant for the air/liquid interface to move into the distal airway.
What this study adds
-
Speed of circulatory recovery was similar when using either 5×3 s inflations or immediate conventional ventilation in near-term asphyxiated lambs
-
A single sustained inflation of 30 s immediately after birth improved speed of circulatory recovery and lung compliance in near-term asphyxiated lambs.
Introduction
Successful resuscitation of bradycardic, apnoeic neonates requires adequate ventilation.1 ,2 The optimal ventilation strategy immediately after birth, when the lungs are liquid-filled, has not been determined. In term asphyxiated infants, there is a lack of evidence to support any specific ventilation strategy for the initial inflations, although one sustained inflation (SI) of 2–5 s has been shown to improve functional residual capacity (FRC).3 ,4 However, to the best of our knowledge, no clinical trials in term infants and no experiments with term or near-term animals have evaluated the effect of different initial inflation times during resuscitation.
The International Liaison Committee on Resuscitation (ILCOR) states that, ‘to establish initial lung inflation in apnoeic newborn infants, initiation of ventilation at birth can be accomplished with either shorter or longer inspiratory times’.2 However, there is a ‘transatlantic divide’5 in how to interpret the ILCOR evidence. The American Heart Association recommends that during neonatal resuscitation ‘assisted ventilation should be delivered at a rate of 40 to 60 breaths per minute’, but does not explicitly suggest using longer inflation times for the initial inflations.6 In contrast, the revised European guidelines recommend that ‘one should maintain the inflation pressure for 2–3 s for the first five inflations as this will help to expand the lungs. Subsequently, babies should be ventilated at a rate of about 30 breaths per minute allowing approximately 1 s for each inflation’.7
Initiating respiratory support with SIs may improve FRC by providing enough pressure for a sufficient period of time to allow the liquid and the air/liquid interface to move through the airways and into the alveoli. Imaging studies in preterm rabbits demonstrated that inflation times of 10–20 s duration, combined with a positive end expiratory pressure (PEEP), immediately after delivery accelerated lung aeration compared with shorter inflation times.8 Similar long inflation times (10–20 s) have been used in clinical studies of preterm infants.9,–,12 However, the best ventilation strategies for preterm infants and term asphyxiated infants may differ because of changes in lung structure and function through gestation and the respiratory drive at birth.
Our objective was to assess the effects of different initial ventilation strategies immediately after birth in near-term asphyxiated lambs. We compared three strategies: (1) inflation times of 0.5 s at a rate of 60/min, (2) five inflations of 3 s or (3) a single 30 s inflation. Our hypothesis was that five short SIs or a single long SI would improve the speed of circulatory recovery and facilitate improved lung liquid clearance compared with no SI.
Methods
Experimental protocol
We used a lamb model of near-term intrauterine asphyxia based on previously published protocols.13 ,14 To assess the ventilation strategies without additional complications, such as a need for chest compressions, we performed a pilot study. We found that allowing the mean carotid blood pressure (CBP) to decrease below 20 mm Hg (normal range 50±10 mm Hg, table 1) was associated with an increased need for chest compression. Thus, we considered a decrease in the mean CBP to ~ 22 mm Hg as an appropriate target to achieve a similar level of asphyxiation in all animals before ventilation was started.
Baseline characteristics and physiological parameters before cord occlusion
Animal preparation
Pregnant ewes at mean (SD) 139(2) days of gestation (term ~ 147 days) were anaesthetised and the fetal head and neck were exposed via caesarean section. At this gestation in sheep, the fetal lungs are well developed with normal surfactant function.15,–,17 Polyvinyl catheters were inserted into a fetal carotid artery and jugular vein. The fetal trachea was intubated with a cuffed endotracheal tube (ETT; 4.5 mm) and clamped to avoid inhalation. The umbilical cord was clamped and cut. Lambs were delivered, dried, weighed and placed on a resuscitation table under a radiant heater to maintain normal body temperature. Lambs received dextrose 50 mg/ml (4) and were lightly sedated (alfaxane iv 5–15 mg/kg/h; Jurox, Auckland, New Zealand) as an ethical requirement. Lung liquid was drained passively via the ETT for 20 s before onset of ventilation. Ewes were euthanised with an overdose of sodium pentobarbitone after delivery.
Asphyxiation
After delivery, neonatal asphyxia was induced by delaying endotracheal ventilation until the mean CBP had decreased to ∼22 mm Hg.
Resuscitation procedure
Lambs received either one of three resuscitation protocols: (1) ventilation with inflation times of 0.5 s at rate 60/min (n=6), (2) five inflations of 3 s duration with 1 s expiratory time (n=6) or (3) a single 30 s inflation (n=6). Lambs in the first two groups (1–2) were randomised into treatment groups by numbered, sealed opaque envelopes. The third group (3) was added after a preliminary analysis of data from the first two groups. For all three groups, we used a peak inflating pressure (PIP) of 35 cm H2O, PEEP of 5 cm H2O and FiO2 0.21. For group (1) and (2), ventilation was delivered with a ventilator (Dräger Babylog 8000plus, Lübeck, Germany). For group (3), the 30 s inflation was delivered with a T-piece device (Neopuff, Fisher & Paykel, Auckland, New Zealand) and the ETT then briefly clamped (to maintain lung volume) during disconnection from the T-piece and connection to the mechanical ventilator.
After the initial ventilation strategies, all three groups received pressure-limited ventilation for the next 10 min (PIP 35 cm H2O, PEEP 5 cm H2O, inflation time 0.5 s, rate 60/min and FiO2 0.21). The ventilator setting was then changed to volume-guarantee ventilation with a target expiratory tidal volume (VT) of 8 ml/kg. After 30 min ventilation (10 min pressure-limited + 20 min volume-guarantee), lambs were euthanised by an overdose of sodium pentobarbitone.
Monitoring
We continuously recorded heart rate (HR), mean CBP, VT and PIP. Dynamic lung compliance (ml/cmH2O/kg=(VT/kg)/(PIP-PEEP)) was calculated.18 Arterial blood samples were collected at 1, 2.5, 5, 7.5, 10, 15, 20 and 30 min after the onset of resuscitation and measured for partial pressure of oxygen (PaO2), partial pressure of carbon dioxide (PaCO2), pH, Base excess (BE) and lactate (ABL30, Radiometer, Copenhagen, Denmark).
Characteristics before the onset of ventilation
Outcome measures
The primary outcome was speed of circulatory recovery assessed by time from start of ventilation until HR was ≥ 120 bpm and mean CBP was ≥ 40 mm Hg. Secondary outcome measure was lung liquid clearance reflected by improvements in lung compliance and blood gases.
Analytical methods
Data were divided into 2 time periods; 0–10 min and 10–30 min after onset of ventilation. These periods were analysed separately as the ventilation protocol changed at 10 min after initiation of ventilation. Mean HR and CBP, VT and PIP were averaged over 5 s epochs every 30 s for the first 10 min. Epochs were then averaged every min until 15 min, then 20, 25 and 30 min. To investigate rapid changes in HR during initial resuscitation, average values were calculated every 1 s during the first 30 s.
Statistical methods
Data were analysed using 2-way repeated measures ANOVA with treatment group (5×3 s SI, 30 s SI and no-SI) and time as factors. Post hoc comparisons between groups and timepoints were performed using the Holm-Sidak test. Data are presented as mean (SD) or median (IQR), as appropriate. A p value < 0.05 was considered significant.
Results
Before cord occlusion, minor differences in PaO2 and lactate values were detected between the groups (table 1), but all physiological parameters were within normal ranges for anaesthetised fetal sheep. The duration of asphyxia (10–11 min) was similar in all groups. At the end of the asphyxia, immediately before onset of ventilation, all physiological parameters were similar between the groups (table 2).
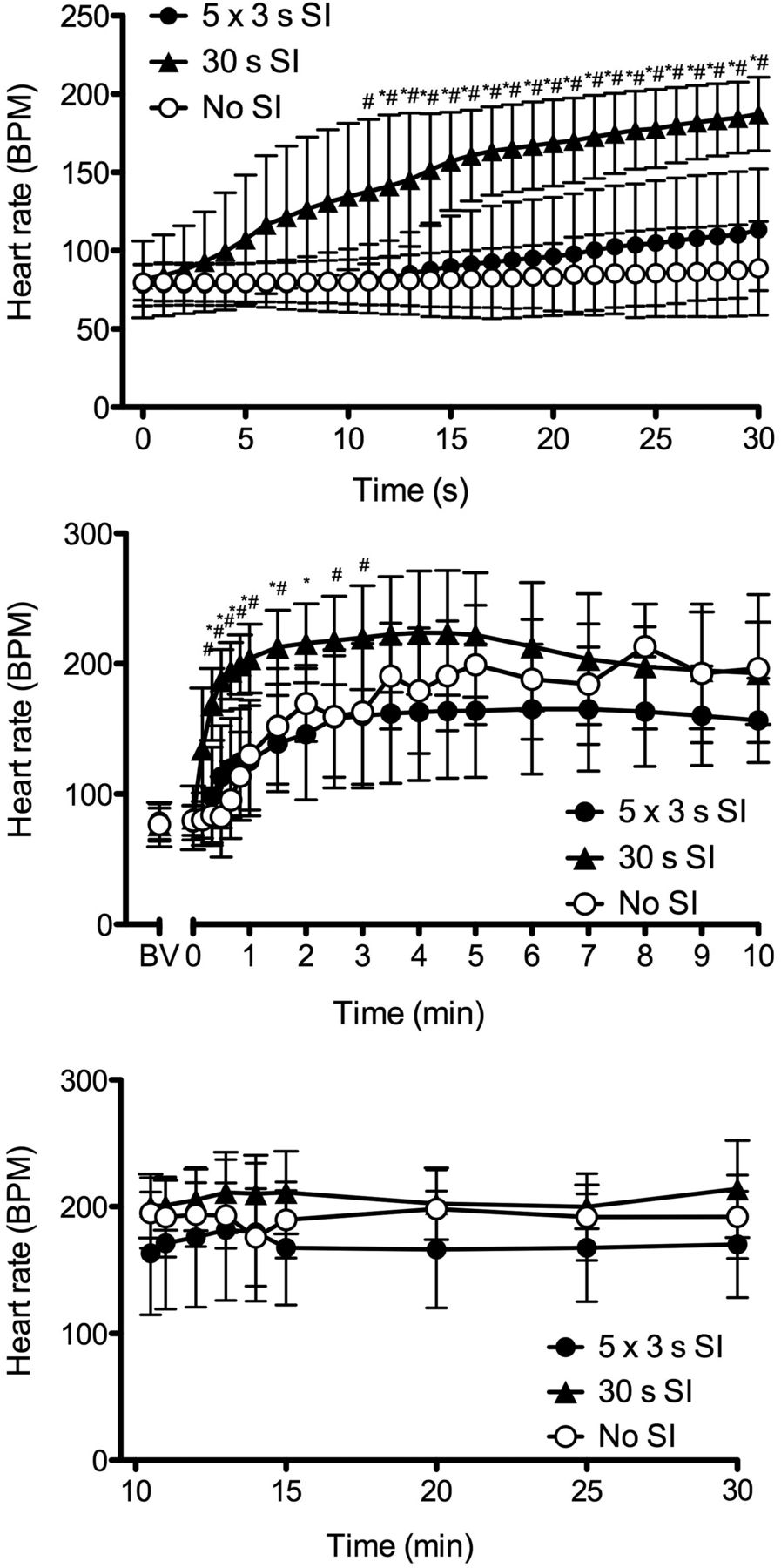
In the 30 s SI group, there was an early and rapid increase in HR compared with the other two groups (figure 1). Lambs in the 30 s SI group reached the target HR of 120 bpm significantly earlier than lambs in both other groups (table 3, figure 1). From 4 min after the onset of ventilation, there were no differences in HR between all groups (figure 1). The rapid increase in HR in the 30 s SI group was accompanied by a rapid increase in mean CBP (table 3, figure 2). In contrast, it took significantly longer for lambs in the two other groups to achieve the target CBP of 40 mm Hg (table 3) and the CBP was significantly lower in these groups between three and 5 min after ventilation onset (table 3, figure 2). No significant differences in the metabolic components of asphyxia (lactate and BE) were observed between the groups at any time point during the study period.

Heart rate in lambs receiving five sustained inflations of 3 s (5 x 3 s SI; •), a single 30 s sustained inflation (30 s SI; ▴), or no sustained inflation (No SI; •). Top panel is from 0 to 30 s, middle panel is from 0–10 min and bottom panel is from 10–30 min. The initiation of ventilation is designated as time 0. BV; before onset of ventilation. Data are mean (SD). * p<0.05 5 x 3s SI vs 30 s SI; # p<0.05 30 s SI vs No SI.
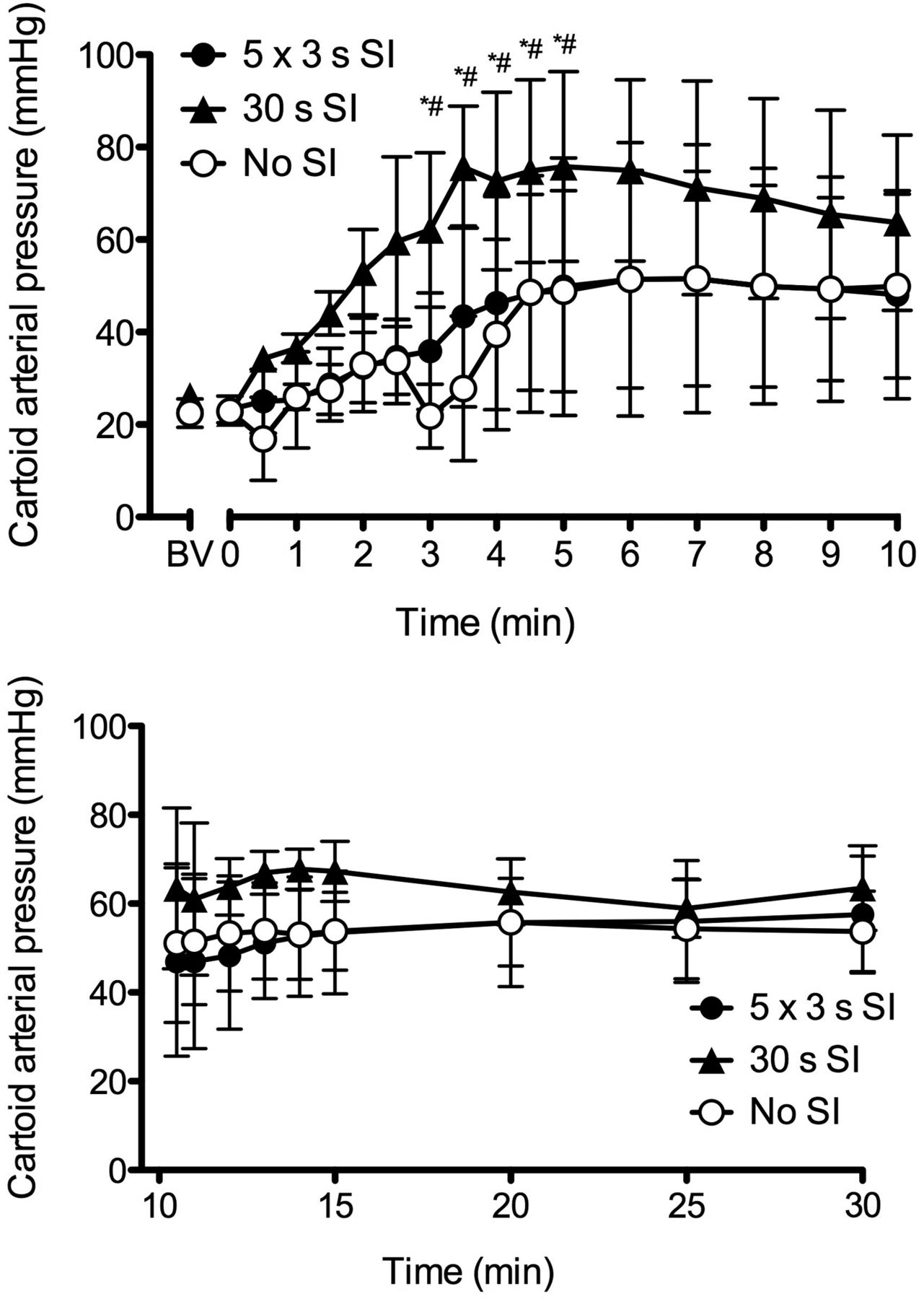
Carotid arterial pressure in lambs receiving five sustained inflations of 3 s (5×3 s SI; •), a single 30 s sustained inflation (30 s SI; ▴), or no sustained inflation (No SI; O). The initiation of ventilation is designated as time 0. Top panel is from 0 to 10 min and bottom panel from 10 to 30 min. BV; before onset of ventilation. Data are mean (SD). *p<0.05 5×3 s SI vs 30 s SI; #p<0.05 30 s SI vs No SI.
Speed of circulatory recovery
The PaCO2 decreased earlier in the 30 s SI group compared with both other groups (figure 3). In the 30 s SI group, the PaO2 values were significantly higher from 5–10 min after start of ventilation compared with both other groups (figure 3).

PaCO2 (top panel) and PaO2 (bottom panel) in lambs receiving five sustained inflations of 3 s (5×3 s SI; •), a single 30 s sustained inflation (30 s SI; ▴), or no sustained inflation SI (No SI; O). The initiation of ventilation is designated as time 0. BV; before onset of ventilation. Data are mean (SD). *p<0.05 5×3 s SI vs 30 s SI; #p<0.05 30 s SI vs No SI.
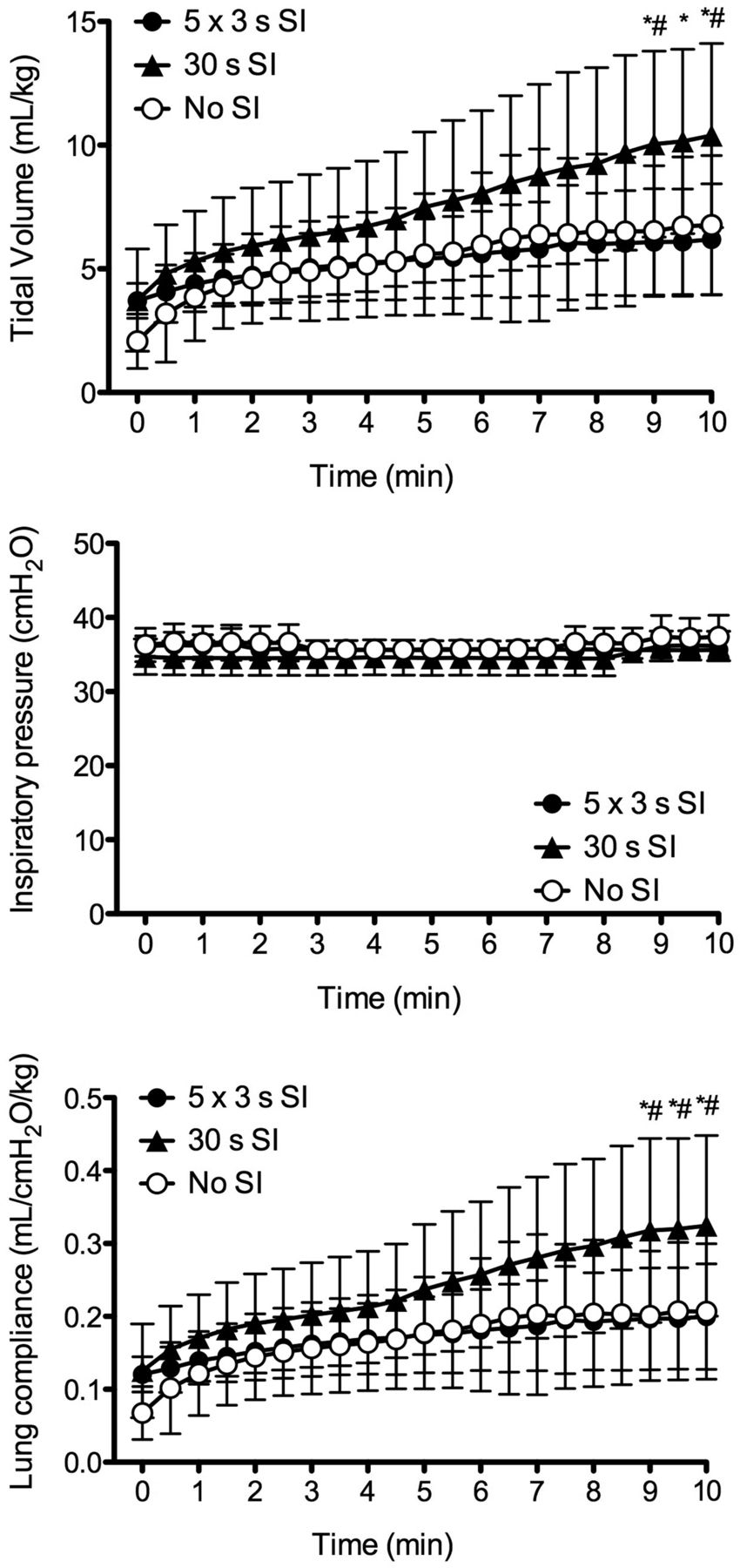
The average VT obtained with the PIP set at 35 cm H2O increased gradually in the 30 s SI group and from 8–10 min it was significantly higher than in both other groups (figure 4). This was due to improved lung compliance (figure 4). Following the switch to volume-guarantee ventilation (set VT 8 ml/kg), the expired VT was similar in all groups (figure 5). However, the PIP required to achieve the set VT was lower and the lung compliance was significantly higher in the 30 s SI group compared with both other groups (figure 5).

Tidal volume (top panel), inspiratory pressure (middle panel) and lung compliance (bottom panel) in lambs receiving five sustained inflations of 3 s (5×3 s SI; •), a single 30 s sustained inflation (30 s SI; ▴), or no sustained inflation SI (No SI; O) from 0 to 10 min. The initiation of ventilation is designated as time 0. Data are mean (SD). *p<0.05 5×3 s SI vs 30 s SI. #p<0.05 30 s SI vs No SI.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Tidal volume (top panel), inspiratory pressure (middle panel) and lung compliance (bottom panel) in lambs receiving five sustained inflations of 3 s (5×3 s SI; •), a single 30 s sustained inflation (30 s SI; ▴), or no sustained inflation SI (No SI; O) from 10 to 30 min. The initiation of ventilation is designated as time 0. Data are mean (SD). *p<0.05 5×3s SI vs 30 s SI; #p<0.05 30 s SI vs No SI.
Discussion
This is the first study to investigate initial ventilation strategies for severe perinatal asphyxia in near-term animals. We compared strategies recommended by expert groups from US6 and Europe/UK7 as well as one based on our previous experiments of using a single long SI.8 ,19 Our primary objective was the speed of circulatory recovery, particularly an increase in HR which is the most sensitive indicator of effective ventilation after birth.2 ,20
Our main finding was a significantly improved increase in HR and CBP, in lambs initially ventilated with a single 30 s SI compared with the much slower increase in HR and CBP observed in both other groups. In contrast, no difference in HR and CBP was observed between lambs receiving initial inflations of 0.5 s at rate 60/min or 5 inflations of 3 s duration. Similar increases in HR have been reported previously in babies21 ,22 and are consistent with observations of a pulmonary vagal inflation reflex reported in a previous animal model.23 This vagal reflex may be modulated by the effectiveness of ventilation, but has primarily been linked with the degree of compromise in infants with primary apnoea.21 Infants and newborn animals showing a slower increase in HR are usually more severely compromised and hence reliant on assisted ventilation.13 It was, however, a striking observation that lambs with similar levels of bradycardia, hypotension and lactic acidosis demonstrated a different pattern of HR-response depending on the initial ventilation strategy.
There is limited evidence supporting guidelines recommending resuscitation with five inflations of 2–3 s duration.7 The use of prolonged inflation times (2–5 s) via an ETT to improve FRC during resuscitation of asphyxiated infants (n=9) was first reported in 1981.3 In a later study, 22 infants were given prolonged inflations by face mask. Most of these 22 infants made an initial cry before the apnoeic episode and were probably not severely compromised.4 Consistent with our findings, in a preterm lamb study, the application of five initial inflations for 5 s produced no significant alteration in gas exchange or lung mechanics, compared with commencing conventional ventilation with PEEP.24 Longer inflation times (≥10 s) have been used in other human and animal studies and these have been associated with beneficial clinical outcomes11 ,12 and uniform aeration of the lungs.8 ,25
Normal term newborns inhale by creating a subatmospheric intra-thoracic pressure as high as −80 cm H2O during their first few breaths.26 An asphyxiated apnoeic newborn infant is unable to generate the pressures required to clear lung liquid and, therefore, will need assistance to initiate lung aeration.27 ,28 The combination of inflation pressure and duration (‘inspiratory effort’) are required for lung aeration and creation of FRC.3 ,27 ,29 High inflating pressures alone are not sufficient29 and may potentially cause a pneumothorax.30 Previous studies have indicated a significantly different pattern of lung expansion in asphyxiated infants requiring resuscitation compared with those breathing spontaneously.31 As inflation times > 2–3 s are needed to rapidly clear lung liquid and improve gas exchange,8 longer inflations may be required to speed circulatory recovery following perinatal asphyxia.
Improved lung aeration results in a marked increase in pulmonary blood flow.19 An increase in oxygenated blood flow returning from the lungs restores cardiac function, resulting in an increased coronary perfusion and cerebral blood flow during the initial resuscitation. We have shown that the initiation of resuscitation in preterm animals may result in adverse fluctuations to pulmonary blood flow, left ventricular output, and subsequently, cerebral blood flow.32 However, an initial SI of 30 s improved the circulatory transition during the immediate resuscitation at birth and stabilised cerebral blood flow in preterm lambs.19 A 30 s SI may thus facilitate a smoother circulatory transition. It is, however, important to acknowledge that large rapid swings in cardiac function caused by ventilation, resuscitation and volume expansion have been associated with cerebral pathology, even in term infants.33 The marked increase in CBP and HR in response to the single 30 s SI may cause a significantly higher cerebral blood flow, which, in a compromised newborn whom is unable to autoregulate, may result in haemorrhage. Further assessment of cerebral haemodynamics and brain injury is required to further elucidate this relationship.
We observed a persistent increase in lung compliance in the single 30 s SI group. Most likely this resulted from improved lung aeration, also reflected by improved oxygenation. To our surprise, this effect persisted beyond the stabilisation period.
The strength of this study is that we examined animals during the fetal-neonatal transition, mimicking an acute asphyxia. We selected to commence ventilation with a fixed PIP, in line with ‘standard practice’ during neonatal resuscitation,6 ,7 and then transition to volume-controlled ventilation which is often used after initial stabilisation. The duration of asphyxia was in a ‘clinical range’ and produced compromised animals with bradycardia, hypotension and lactic acidosis. Our physiological findings are in line with results from a similar near-term lamb asphyxia study, where ventilation commenced 10 min after clamping the umbilical cord.14 A limitation is that the 30 s SI study group was added after the first two were complete. The first two groups tested the efficacy of current recommended clinical guidelines,6 ,7 but our belief was that both strategies failed to successfully aerate the lungs. We therefore added the 30 s SI group to examine physiological changes using a strategy that better aerates the lung. As we used the identical asphyxia model and achieved identical levels of fetal compromise, we believe that the initial long SI was the single factor that improved outcomes. We were able to drain substantial volumes of lung liquid from the ETT of lambs born by caesarean section. In humans, a similar phenomenon has been described as liquid ‘gushing’ from the nose and mouth following delivery of the fetal head.35 The amount of lung liquid drained passively following a human infant's birth has not been quantified, but our impression is that it is less than the volume drained from the ETT in lambs. In our model, we therefore passively drained lung liquid from the major airways. Still, a significant amount of lung liquid remains in the lungs, which presumably equates to the residual lung volume.36
As it is still unclear whether a SI during the transition is injurious to the lung, an examination for lung injury may have broadened the outcomes and significance of this study. However, the lambs we used were mature, were not surfactant deficient and all received PEEP. As surfactant and PEEP are able to protect the immature lung from inflammation and injury,37 it is likely that any lung injury would have been subtle and difficult to detect in our near-term lambs. Further studies are, therefore, needed to elucidate whether an SI is protective or injurious to the neonatal lung.
Conclusion
A single sustained inflation of 30 s duration markedly improved speed of circulatory recovery, lung compliance and oxygenation in this near-term lamb asphyxia model. This approach for resuscitation following perinatal asphyxia merits further investigation.
Acknowledgments
The authors thank Ms Karyn Rodgers and Ms Alison Moxham for their assistance with these experiments and Colin Morley for critical reading and input to the manuscript.
References
Footnotes
Both CK and KS contributed equally to this study.
-
Funding PGD and SBH hold an Australian National Health and Medical Research Council Program Grant No. 384100. PGD is a recipient of an NHMRC Practitioner Fellowship. JAD and GMS are past recipients of a RWH Postgraduate Scholarship. GRP and SBH are NH&MRC Research Fellows and the authors gratefully acknowledge the Victorian Government's Operational Infrastructure Support Program. JAD is recipient of a National Health and Medical Research Council Post Doctoral Fellowship.
-
Competing interests None.
-
Ethics approval All experimental procedures were approved by the relevant Monash University Animal Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.