Article Text

Abstract
Objective The objective of our study was to examine the relationship between brain injury and outcome following neonatal hypoxic–ischaemic encephalopathy treated with hypothermia.
Design and patients Neonatal MRI scans were evaluated in the National Institute of Child Health and Human Development (NICHD) randomised controlled trial of whole-body hypothermia and each infant was categorised based upon the pattern of brain injury on the MRI findings. Brain injury patterns were assessed as a marker of death or disability at 18–22 months of age.
Results Scans were obtained on 136 of 208 trial participants (65%); 73 in the hypothermia and 63 in the control group. Normal scans were noted in 38 of 73 infants (52%) in the hypothermia group and 22 of 63 infants (35%) in the control group. Infants in the hypothermia group had fewer areas of infarction (12%) compared to infants in the control group (22%). Fifty-one of the 136 infants died or had moderate or severe disability at 18 months. The brain injury pattern correlated with outcome of death or disability and with disability among survivors. Each point increase in the severity of the pattern of brain injury was independently associated with a twofold increase in the odds of death or disability.
Conclusions Fewer areas of infarction and a trend towards more normal scans were noted in brain MRI following whole-body hypothermia. Presence of the NICHD pattern of brain injury is a marker of death or moderate or severe disability at 18–22 months following hypothermia for neonatal encephalopathy.
Statistics from Altmetric.com
Brain injury in term infants with hypoxic–ischaemic encephalopathy (HIE) is shown by conventional MRI1,–,4 as either a watershed pattern involving the white matter (WM) and extending to the cortical grey matter, or as a basal nuclei pattern. Both motor and cognitive impairments are seen in childhood following acute perinatal events.5,–,9
Hypothermia initiated within 6 h of birth at 33–34°C and continued for 72 h among term infants with HIE decreases death or disability among cooled infants or increases survival-free disability at 18 months of age.10,–,15 In 2010, Rutherford et al reported the results of brain imaging in a subset of infants in the TOBY randomised controlled trial (RCT).16 In the National Institute of Child Health and Human Development (NICHD) Neonatal Research Network (NRN) RCT of whole-body hypothermia for 72 h at 33.5°C,11 we assigned a score based on the pattern of brain injury on the neonatal MRI scans. Our objective was to evaluate whether the score could serve as a marker of death or disability at 18 months of age.
What is already known on this topic
Perinatal hypoxic–ischaemic encephalopathy (HIE) is associated with childhood morbidity/mortality.
Hypothermia is associated with a reduction in death and disability at 18–22 months following neonatal HIE.
Brain injury can be reduced on MRI in neonatal encephalopathy treated with hypothermia.
What this study adds
In a randomised controlled trial of hypothermia therapy, 65% of infants had MRI scans.
A categorisation capturing all areas of brain injury, including hemispheric devastation, is described.
The National Institute of Child Health and Human Development Neonatal Research Network pattern of brain injury is strongly associated with death or disability at 18–22 months.
Methods
The RCT recruited 208 subjects between July 2000 and May 2003 in the 15 participating NICHD NRN centres. The follow-up visits ended in December 2004. Term infants were eligible if they had severe acidosis or birth resuscitation following an acute perinatal event and moderate or severe encephalopathy within 6 h of birth. After informed consent was obtained from a parent, infants were randomly assigned by telephone by the data-coordinating centre (RTI International) to whole-body hypothermia at 33.5°C for 72 h or usual intensive care. Assignments were stratified by centre and generated by a random, permuted-block algorithm with block sizes of two or four. The primary outcome of the main RCT and this secondary study was death or disability at 18–22 months of age. All surviving infants were evaluated by certified examiners who were trained to reliability to perform the neurodevelopmental assessments and were unaware of study intervention status. Severe disability was defined as either: Bayley II Mental Developmental Index (MDI) less than 70, a Gross Motor Function Classification System (GMFCS) grade level 3 to 5, hearing impairment requiring hearing aids, or blindness. Moderate disability was defined as an MDI of 70–84 in addition to a GMFCS grade of level 2, hearing impairment with no amplification, or a persistent seizure disorder.
The cranial imaging protocol required an MRI to be performed by 44 weeks postmenstrual age or when clinically feasible. T1 and T2 weighted sequences with 1.5 or 3 T conventional images were obtained. MRI evaluations were stored on computer discs at the NRN sites for later evaluation. In 2006, an MRI form was developed to capture areas of brain injury described previously1 ,2 and to gather additional detailed information on the location and size of signal abnormalities in the following regions: cerebral hemispheres, intraventricular areas, cerebellum, basal ganglia (BG), thalamus, internal capsule, corona radiata, hippocampus, brain stem, corpus callosum, pituitary, hypothalamus, optic chiasma and extra-axial area. Lesions were coded as cystic, non-cystic, haemorrhagic, mineralisation or gliosis and whether they were minimal or more extensive. Areas of watershed infarction, cerebral atrophy and ventricular enlargement were also documented. All MRI examinations were sent to the data centre.
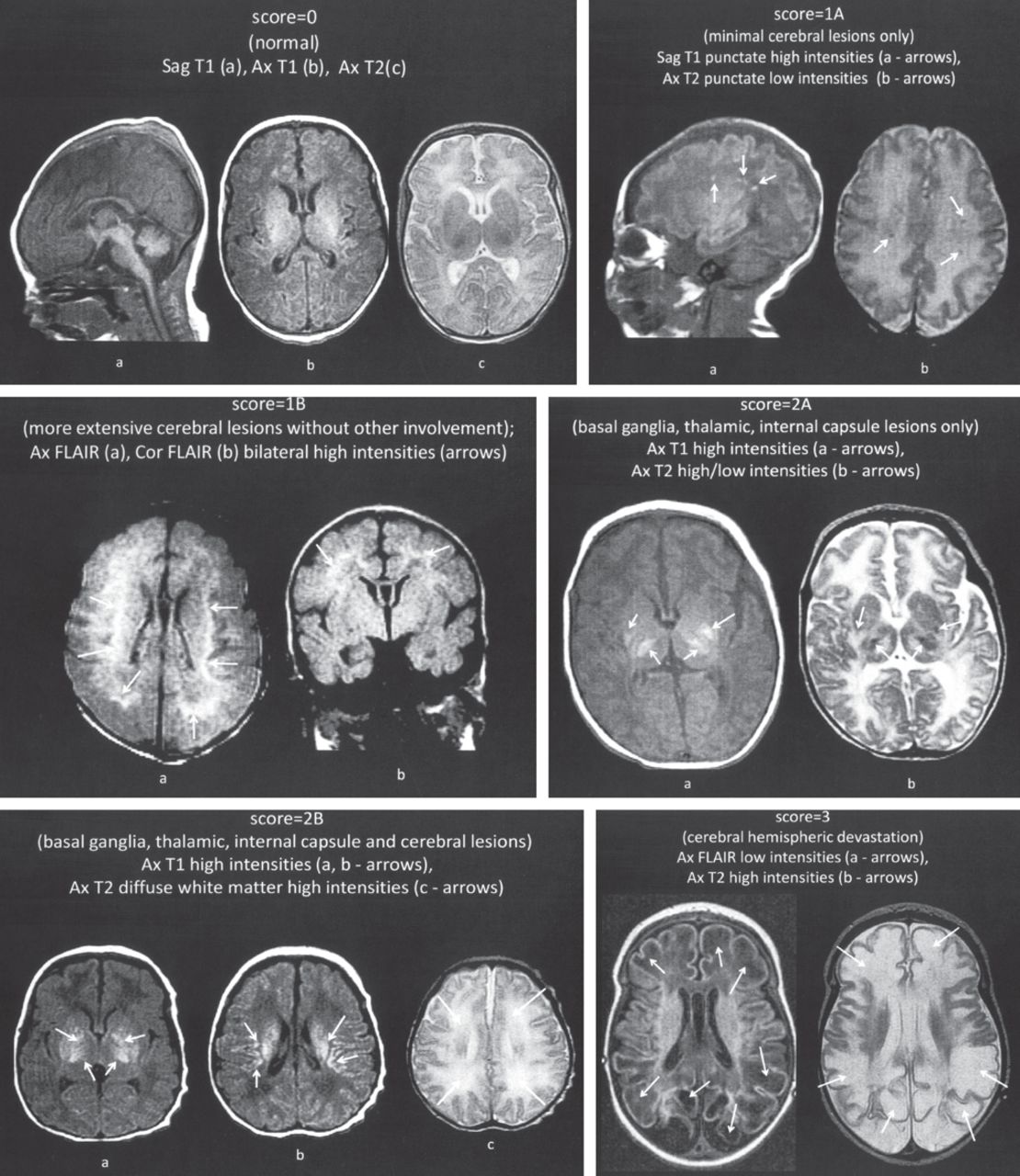
In 2007–2008, all MRI readings were evaluated for quality and read by a central reader (PDB). The readings were then reviewed by the central reader and the NICHD MRI NRN study subcommittee in 2009. Since multiple areas of injury were noted by the central reader that did not fall into existing assessment systems,1 ,2 an additional NICHD brain injury pattern was created (figure 1). Each level reflected a greater involvement of brain injury: 0, normal; 1A, minimal cerebral lesions only with no involvement of BG or thalamus (T) or anterior limb of the internal capsule (ALIC) or posterior limb of the internal capsule (PLIC) and no area of watershed infarction; 1B, more extensive cerebral lesions without basal ganglia and thalamic (BGT), PLIC or ALIC involvement or infarction; 2A, any BGT, ALIC or PLIC involvement or watershed infarction noted without any other cerebral lesions; 2B, involvement of either BGT, ALIC or PLIC or area of infarction and additional cerebral lesions; and 3, cerebral hemispheric devastation. All infants were coded based on the pattern of injury without knowledge of treatment intervention status.
{kind=link}
(A) National Institute of Child Health and Human Development Neonatal Research Network score=0; (B) score 1A: lesions in frontal and parietal subcortical areas; (C) score 1B: more extensive cerebral lesions in frontal, parietal and occipital subcortical areas; (D) score 2A: lesions in the basal ganglia and thalamic area (BGT) and internal capsule (IC); (E) score 2B: lesions in the BGT, IC and cerebral areas; (F) score 3: cerebral hemispheric devastation.
The RCT protocol was approved by the institutional review board of the NRN centres.
Statistical analysis
Data were analysed at the data centre with SAS V.9.2. The maternal and neonatal characteristics were compared between treatment groups by Fisher's exact test for categorical variables and t tests for continuous data. MRI findings by region were compared between treatment groups with Fisher's exact test. The frequency of infants with a normal MRI was compared to other levels of injury using previously described patterns and NICHD score using Fisher's exact test. The relationship between the MRI patterns of injury and the primary outcome was assessed by Cochran-Armitage trend tests, with the NICHD NRN pattern of injury used as a six-level variable (0, 1A, 1B, 2A, 2B, 3). Lastly, the relationship between the NICHD NRN pattern of injury and death or disability was assessed using a multivariate logistic regression model controlling for severity of encephalopathy, hypothermia therapy and age at MRI scan.
Results
MRI studies were obtained for 151 of the 208 RCT participants. Of these, 143 were of adequate quality and 136 (90%) were obtained by 44 weeks postmenstrual age and comprised the cohort analysed. There were 73 infants in the hypothermia group and 63 infants in the control group. The average age (mean±SD) at which scans were obtained was 15±12 days. There were 39 infants with MRI scans obtained before 7 days of age.
The maternal and neonatal characteristics were similar in the hypothermia and control groups except that antepartum haemorrhage occurred in fewer mothers in the hypothermia group compared to the control group (table 1). The most frequent MRI lesions among the total cohort (65 of 136 infants, 48%) were noted in the cerebral hemispheres other than the BGT and watershed area. The perisylvian region was involved in 32%, perirolandic in 29% and parasagittal area in 8% of infants. Fifty-four (40%) infants had BG injury, 37 of whom had multiple lesions. Isolated BG lesions were noted in 17 infants; 16 in the putamen and one in the globus pallidus. Thalamic lesions were noted in 50 of 136 infants (37%); of these, the majority (98%) of lesions were bilateral. Haemorrhagic lesions were noted in 10 of 132 (8%) infants. None of the infants had a specific MRI diagnosis of venous sinus thrombosis. WM scarring/gliosis was noted in 36 infants, whose age at MRI was 16.4±13.0 days. Cerebral atrophy was noted in 10 infants, all of whom had the scans obtained beyond 3 weeks of age. Moderate/marked enlargement of the subarachnoid space was noted on the left in six infants and on the right in seven infants. Moderate to marked thinning of the corpus callosum was noted in eight infants. Moderate/marked ventricular dilatation was seen on the right in eight infants and on the left in nine infants. Cerebellar lesions were infrequent; five infants had signal abnormalities in the cerebellum including one haemorrhagic lesion. Abnormalities in the corona radiata were noted in 11 infants (all of which were bilateral). Only five infants had involvement of the hippocampus and six infants had involvement of the brain stem. None of the infants had a shift in the midline structures noted.
Characteristics of study subjects
The MRI findings among the hypothermia and control group infants were categorised by site (table 2). Cerebral lesions were similar in frequency in the two groups except that the perisylvian location was abnormal in five of 30 infants (17%) in the hypothermia group and 16 of 35 infants (46%) in the control group (p=0.02). There was a trend for more normal MRI studies and normal appearance of the PLIC and ALIC among infants in the hypothermia group as compared to infants in the control group. There were significantly fewer areas of watershed infarction noted in the hypothermia group compared to the control group. MRI studies of all infants were categorised by the NICHD NRN pattern of injury; three infants could not be classified by the Barkovich pattern and nine could not be classified by the Rutherford pattern. The most frequent pattern of injury with the NICHD score was 2B: BGT, PLIC or ALIC involvement, or areas of infarction with additional cerebral lesions.
MRI findings among study subjects by region and pattern of injury
The relationships between the pattern of injury (among infants who could be categorised) and the primary outcome of death or moderate/severe disability at 18–22 months of age are noted in table 3. Occurrence of any of the three patterns was associated with death or disability. Based on the NICHD NRN pattern of injury, among the 52 infants with the primary outcome of death and disability, 47 had abnormal patterns of injury; of the 82 infants without the primary outcome, 53 had normal MRI studies (sensitivity 0.90, specificity 0.65, positive predictive value 0.62 and negative predictive value 0.91). Within the hypothermia and control groups there were consistent relationships between the NICHD pattern of injury and outcome of death or disability and disability among survivors (table 4); there was no relationship with death alone, probably due to the small number of infants who died for whom MRI was available. The relationship between the NICHD pattern of injury and outcome was further examined by regression analysis while controlling for treatment group, level of HIE and age at MRI. The interaction between age at MRI and the NICHD pattern of injury was p=0.11 with age as a continuous variable and p=0.20 with age dichotomised as birth to 7 versus ≥8 days. Each point increase in the severity of the NICHD NRN pattern of injury was independently associated with a more than a twofold increase in the odds of death or disability at 18–22 months of age: OR 2.3 (95% CI 1.7 to 3.1) with age at MRI as a dichotomous variable and OR 2.4 (1.8 to 3.3) with age at MRI as a continuous variable.
Relationship between MRI pattern of injury and outcome
Relationship between the NICHD MRI pattern of injury and primary outcome within the two groups
Discussion
Recent reports16,–,20 describing MRI studies in infants with asphyxia treated with hypothermia have shown protection of grey matter in a study of 26 infants randomly assigned to normothermia or whole-body hypothermia.17 A decrease in BGT lesions was noted when 14 infants with head cooling were compared to 20 infants with whole-body hypothermia and 52 non-cooled infants with HIE of similar severity.18 In the TOBY trial, with 40% of trial participants, a reduction in BGT, WM and PLIC lesions was noted in infants in the whole-body hypothermia group compared to infants in the control group.16 In our study of 65% of trial participants, we found fewer areas of watershed infarction along with a trend for more normal studies and normal ALIC and PLIC among infants who received hypothermia.
The TOBY trial noted that scans performed within the first week of age were more likely to show abnormalities compared to those performed after 8 days.16 In our study, scans were performed at the discretion of the treating neonatologist and the average age of obtaining the scans was later than in the TOBY study. We did not find any statistical interaction between the NICHD NRN pattern of brain injury and outcome based on age at scanning. A recent review has suggested that the discriminatory power of later MRI scanning (8–30 days) is better than that of early MRI (1–7 days).21 Compared to the TOBY study, infants in our study had fewer areas of BGT injury (31% vs 59% of hypothermia group and 49% vs 79% of control group infants) and fewer equivocal/abnormal PLIC (36% vs 47% of hypothermia group and 55% vs 66% of control group infants). We identified fewer areas of haemorrhage: 7% versus 39% of hypothermia group and 8% versus 33% of control group infants, respectively. The differences in brain injury patterns between the two studies may be due to the greater number of infants with moderate encephalopathy in our study.
The predictive value of the NRN pattern of injury and outcome at 18–22 months was consistent in both the hypothermia and control groups in our study. The TOBY study also noted that patterns of brain injury correlate with outcome whether the infant is cooled or not.16 We do not know how cooling to 33–34°C for 72 h impacts on the evolution of images, but hypothermia does not appear to delay the appearance of abnormalities.22 The reduction in areas of brain injury in the hypothermia group compared to the control group in both the NICHD NRN and the TOBY study, despite a difference in the age at acquisition of MRI scans, strengthens the evidence that whole-body hypothermia is neuroprotective for term infants with HIE.
The strength of our study is that we have examined brain injury within an RCT of hypothermia compared to intensive care alone in the largest reported proportion of trial participants (136 of 208 or 65%). All readings were performed by a central reader unaware of the clinical course or treatment, with adjudication by the study subcommittee. The NICHD pattern of injury was developed to capture all areas of brain injury in a well defined cohort of infants with moderate or severe HIE assigned to hypothermia or intensive care alone and followed to 18–22 months of age. Previous summary scores1 ,2 have correlated areas of brain injury to outcome, however infants in these studies did not have comprehensive follow-up and the cohorts were not limited to infants with severe acidosis/birth resuscitation and physiological and clinical evidence of moderate/severe HIE. Categorisation of the majority of our study infants based on patterns of injury described previously1 ,2 was correlated with outcome, emphasising the predictive value of existing MRI scoring systems. We have described hemispheric devastation, a finding not reported by other investigators; all infants with this level of brain injury have an adverse outcome of death or survival with disability. The limitations of our study include inadequate or unavailable MRI data on 72 infants, 47 of whom died. Magnetic resoance spectroscopy, diffusion weighted imaging or diffusion tensor imaging studies were not obtained on our trial participants.21 ,23
Our study demonstrating an excellent correlation between the NICHD NRN MRI evidence of neonatal brain injury and outcome of death or disability at 18–22 months of age may be useful when counselling parents of infants with HIE.24 A normal MRI is associated with a normal outcome, while each point increase in the abnormal pattern of brain injury has a twofold increase in the odds of death or disability. Conventional MRI is currently available in the majority of neonatal centres. With further study and validation, the NICHD pattern of injury following hypoxia–ischaemia may serve as a biomarker of brain injury as well as a response to neuroprotective strategies.
Acknowledgments
The following investigators, in addition to those listed as authors, participated in this study: NRN Steering Committee Chairs: Alan H Jobe, University of Cincinnati (2003–2006); Michael S Caplan, University of Chicago, Pritzker School of Medicine (2006–present); Alpert Medical School of Brown University and Women and Infants Hospital of Rhode Island (U10 HD27904): William Oh, Betty R Vohr, Bonnie E Stephens, Theresa M Leach, Angelita M Hensman, Lucy Noel, Victoria E Watson; Case Western Reserve University Rainbow Babies and Children's Hospital (U10 HD21364, M01 RR80): Avroy A Fanaroff, Deanne E Wilson-Costello, Nancy Bass, Harriet G Friedman, Nancy S Newman, Bonnie S Siner; Cincinnati Children's Hospital Medical Center University of Cincinnati Hospital (U10 HD27853, M01 RR8084): Kurt Schibler, Kate Bridges, Jean J Steichen, Kimberly Yolton, Barbara Alexander, Cathy Grisby, Holly L Mincey, Jody Hessling, Teresa L Gratton; Duke University School of Medicine University Hospital, Alamance Regional Medical Center, and Durham Regional Hospital (U10 HD40492, M01 RR30): C Michael Cotten, Kathryn E Gustafson, Ricki F Goldstein, Kathy J Auten, Kimberley A Fisher, Sandy Grimes, Melody B Lohmeyer; Emory University Grady Memorial Hospital and Emory University Hospital Midtown (U10 HD27851, M01 RR39): Ira Adams-Chapman, Lucky Jain, Ann M Blackwelder, Ellen C Hale, Sobha Fritz, Sheena Carter, Maureen Mulligan LaRossa; Eunice Kennedy Shriver National Institute of Child Health and Human Development: Linda L Wright, Elizabeth M McClure; Indiana University Indiana University Hospital, Methodist Hospital, Riley Hospital for Children and Wishard Health Services (U10 HD27856, M01 RR750): James A Lemons, Anna M Dusick, Lucy C Miller, Leslie Richard, Leslie Dawn Wilson; RTI International (U10 HD36790): W Kenneth Poole, Jeanette O’Donnell Auman, Margaret Cunningham, Betty K Hastings, Jamie E Newman, Carolyn M Petrie Huitema, Scott E Schaefer; Stanford University Lucile Packard Children's Hospital (U10 HD27880, M01 RR70): David K Stevenson, Susan R Hintz, M Bethany Ball, Barry E Fleisher, Anne M DeBattista, Joan M Baran, Julie C Lee-Ancajas; University of Alabama at Birmingham Health System and Children's Hospital of Alabama (U10 HD34216, M01 RR32): Namasivayam Ambalavanan, Myriam Peralta-Carcelen, Kathleen G Nelson, Monica V Collins, Shirley S Cosby, Vivien A Phillips, Fred J Biasini, Kirstin J Bailey; University of California-San Diego Medical Center and Sharp Mary Birch Hospital for Women and Newborns (U10 HD40461): Martha G Fuller, Radmila West, David Kaegi, Maynard R Rasmussen, Yvonne E Vaucher, Kathy Arnell, Chris Henderson, Wade Rich; University of Miami Holtz Children's Hospital (U10 HD21397, GCRC M01 RR16587): Charles R Bauer, Sylvia Hiriart-Fajardo, Mary Allison, Maria Calejo, Ruth Everett-Thomas, Silvia M Frade Eguaras, Susan Gauthier; University of Rochester Medical Center Golisano Children's Hospital (U10 HD40521, M01 RR44): Dale L Phelps, Rosemary Jensen, Linda J Reubens; University of Texas Southwestern Medical Center at Dallas Parkland Health & Hospital System and Children's Medical Center Dallas (U10 HD40689, M01 RR633): Pablo J Sánchez, R Sue Broyles, Charles R Rosenfeld, Walid A Salhab, Roy J Heyne, Cathy Boatman, Cristin Dooley, Gaynelle Hensley, Jackie F Hickman, Susie Madison, Nancy A Miller, Janet S Morgan, Alicia Guzman, Elizabeth Heyne, Linda A Madden, Sally Adams; University of Texas Health Science Center at Houston Medical School, Children's Memorial Hermann Hospital and Lyndon Baines Johnson General Hospital/Harris County Hospital District (U10 HD21373, M01 RR2588): Kathleen A Kennedy, Esther G Akpa, Patty A Cluff, Claudia Y Franco, Anna E Lis, Georgia E McDavid, Patti L Tate, Nora I Alaniz, Pamela J Bradt, Magda Cedillo, Susan Dieterich, Terri Major-Kincade, Brenda H Morris, Maegan C Simmons, Laura L Whitely; Wayne State University Hutzel Women's Hospital and Children's Hospital of Michigan (U10 HD21385): Geraldine Muran, Yvette R Johnson, Deborah Kennedy, Laura A Goldston; Yale University Yale-New Haven Children's Hospital (U10 HD27871, MO1 RR125, MO1 RR6022): Patricia Gettner, Monica Konstantino, JoAnn Poulsen, Elaine Romano, Joanne Williams; Data and Safety Monitoring Committee: Gordon Avery, chair, Children's National Medical Center; Mary E D’Alton, Columbia University; W Kenneth Poole (ex officio), RTI International; J C Fletcher (deceased), University of Virginia; Christine A Gleason, chair, University of Washington; Carol K Redmond, University of Pittsburg; Marian Willinger (ex officio), Eunice Kennedy Shriver National Institute of Child Health and Human Development.
References
Footnotes
-
Funding The National Institutes of Health and the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) provided grant support for the Neonatal Research Network's whole-body hypothermia and follow-up studies.
-
Competing interests Dr Cotten reports having served on the data and safety monitoring board for the Inhibitex phase 3 study of Vernonate for the prevention of infections in preterm infants. Dr Donovan reports having received support from the Environmental Protection Agency (Lanphear) and the Gerber Foundation. Dr Carlo reports holding stock options at the Pediatrix Medical Group. Dr Stevenson reports having received research support from Pfizer.
-
Ethics approval The institutional review board at each of the participating centres approved this study.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Currently, unpublished data are unavailable pending further NICHD Neonatal Research Network analyses and publications.
Data collected at participating sites of the NICHD Neonatal Research Network (NRN) were transmitted to RTI International, the data coordinating centre (DCC) for the network, which stored, managed and analysed the data for this study. On behalf of the NRN, Dr Abhik Das (DCC Principal Investigator) and Mr Scott A McDonald (DCC Statistician) had full access to all the data in the study and take responsibility for the integrity of the data and accuracy of the data analysis.
Linked Articles
- Fantoms