Article Text

Abstract
Background Nasal intermittent positive pressure ventilation (NIPPV) may be beneficial but the mechanisms of action are undetermined.
Aim To investigate the effects of non-synchronised NIPPV on spontaneous breathing in premature infants.
Methods 10 infants receiving ventilator generated non-synchronised NIPPV were studied for 30 min. Delivered pressure was measured at the nose; respiration was recorded using respiratory inductance plethysmography. Oxygen saturation, carbon dioxide, heart rate, inspired oxygen and video images were recorded.
Results Median gestational age, birth weight, age and study weight were 25+3 weeks, 797 g, 24 days and 1076 g. When the NIPPV pressure peak commenced during spontaneous inspiration the inspiratory time increased by 21% (p=0.002), relative tidal volume increased by 15% (p=0.01) and expiratory time was unchanged. When the NIPPV pressure peak commenced during spontaneous expiration the expiratory time increased by 13% (p=0.04). NIPPV pressures delivered during apnoea (range 8–28 cm H2O) produced chest inflation 5% of the time, resulting in small tidal volumes (26.7% of spontaneous breath size) but reduced oxygen desaturation. NIPPV pressure peaks occurred throughout spontaneous respiration proportional to the inspiratory: expiratory ratio.
Conclusion NIPPV pressure peaks only resulted in a small increase in relative tidal volumes when delivered during spontaneous inspiration. During apnoea pressure peaks occasionally resulted in chest inflation, which ameliorated oxygen desaturations. Infants did not become entrained with the NIPPV pressure changes. Synchronising every rise in applied pressure with spontaneous inspiration may increase the effectiveness of NIPPV and warrants investigation.
Statistics from Altmetric.com
Introduction
Non-invasive respiratory support is increasingly used to assist breathing in premature infants.1 2 Nasal continuous positive airway pressure (CPAP) may help to avoid intubation and ventilation in premature infants.3 4 However nasal CPAP does not provide sufficient support for all infants; up to half of preterm infants less than 28 weeks gestation ‘fail’ initial CPAP support3 5 and up to a third ‘fail’ extubation to CPAP.6,–,8 As a result nasal intermittent positive pressure ventilation (NIPPV) is of increasing interest and importance and may offer more effective support than CPAP alone.
What is already known about this subject
▶ Nasal intermittent positive pressure ventilation (NIPPV) is a form of non-invasive respiratory support. It reduces intubation rates, extubation failure and broncho-pulmonary dysplasia in preterm infants, compared with continuous positive airway pressure.
▶ Neonatal NIPPV may increase tidal volume, improve gas exchange, reduce work of breathing and reduce respiratory rate but its mechanisms of action are undetermined.
What this study adds
▶ Infants didn't become entrained with the ventilator rate during non-synchronised NIPPV. When pressure peaks occurred during inspiration tidal volume increased, suggesting that synchronisation may be beneficial.
▶ During apnoea NIPPV pressures were rarely transmitted to the chest, when they were there was less oxygen desaturation, despite producing only small tidal volumes.
NIPPV refers to techniques that combine nasal CPAP with intermittent increases in applied pressure. Nomenclature describing NIPPV varies as different methods of generating NIPPV ‘inflations’ have led to different ways of describing the technique. Using the term ‘inflations’ for NIPPV pressure variations is misleading as there is little evidence the delivered pressure results in chest inflation.
Non-invasive ventilatory techniques are established in adults9,10,–,13 and children14 15 where they work like ventilation. They use tight fitting masks with minimal leak and flow sensors for synchronisation. NIPPV in neonates is quite different; nasal prongs often have a large leak around the prongs and from the mouth. This means that synchronising NIPPV pressure changes with spontaneous breathing using flow triggering is extremely difficult. Abdominal pneumatic capsules, which detect abdominal movement, have been used to attempt synchronisation, but it is unclear how accurate and effective they are. Worldwide, few neonatal devices are available which synchronise the non-invasive pressure changes with spontaneous breathing.
Several physiological studies have described the effects of neonatal NIPPV16,17,–,20 and although several hypotheses have been generated, the mechanisms of action have not been determined. The assumption is that some of the applied pressure is transmitted to the lower airways, but it is not known whether this happens. The applied peak pressures during neonatal NIPPV, particularly NIPPV generated via a ventilator, are usually not synchronised to the infant's inspiration. A recent survey found that 25% of NIPPV users in England do not routinely use a synchronisation device.1 In other countries this percentage may be higher as some ‘synchronising’ NIPPV devices are unlicensed in other countries, for example, the SiPAP (Care Fusion, Dublin, OH, USA) device is not licensed for use in its ‘synchronised’ mode in the USA. One early observational study of non-synchronised NIPPV21 suggested that infants became entrained with the non-synchronised NIPPV cycles. This has not been replicated and it is not clear how spontaneous breathing and NIPPV pressures interact during neonatal NIPPV.
The aims of this observational study were to investigate whether, during non-synchronised ventilator-generated NIPPV, the applied NIPPV pressures are transmitted to the lower airways to produce volume change; to describe the effects of NIPPV on spontaneous breathing and to determine whether infants become entrained with the NIPPV pressure cycles.
Methods
Study population
A convenience sample of 10 infants born below 30 weeks gestation was studied. Infants were at least 48 h old, receiving ventilator generated NIPPV and without major congenital abnormalities. The study was at the Royal Women's Hospital, Melbourne, Australia and was approved by the hospital research and ethics committees. Written parental consent was obtained prior to enrolment.
NIPPV delivery
Non-synchronised NIPPV was generated using a Dräger Babylog 8000+ ventilator (Dräger Medical, Lübeck, Germany) in continuous mandatory ventilation mode. NIPPV settings were determined by the clinical team. No changes were made to ventilator settings, or infant position, during the studies. Manufacturer's recommendations guided Hudson prong size (Teleflex Medical, Research Triangle Park, North Carolina, USA) and nursing staff judged the prong size that did not blanch the nares. The prongs were secured using a hat and chin strap (CPAP CAP System; Austranter Medical System, ACT, Canberra, Australia).
Physiological measurements
The NIPPV pressures were measured using a calibrated Florian Respiratory Function Monitor (Acutronic Medical Systems AG, Hirzel, Switzerland), sampling from the inspiratory limb of the Hudson prong. Spontaneous breathing and relative tidal volume were recorded using respiratory inductance plethysmography—RIP (Somnostar and Respiband Plus; SensorMedics, Yorba Linda, California, USA). RIP records impedance change (mV) from the chest (RIPchest) and abdomen (RIPabdo). RIP was not calibrated to a measured tidal volume hence the sum of the abdominal and chest recordings represented relative tidal volume (RIPsum). Respiratory rate was recorded using an abdominal pneumatic capsule (Graseby Respiration Monitor MR10; Graseby Medical, Watford, England) secured onto the anterior abdominal wall. Oxygen saturation (SpO2) and heart rate were measured with a Masimo Radical SET Pulse Oximeter (Masimo, Irvine, California, USA) and the inspired oxygen was measured using an oxygen analyser in the inspiratory limb of the NIPPV circuit (MX300 Oxygen Analyzer; Teledyne Analytical Instruments, City of Industry, California, USA). Transcutaneous carbon dioxide (CO2) levels were continuously recorded by a TINA-TCM3 Transcutaneous Saturation Monitor (Radiometer, Copenhagen, Denmark). A webcam (QuickCam 6.4.8; Logitech, Romanel-sur-Morges, Switzerland) recorded images of the infants face, chest and abdomen. Data were continuously sampled at 200 Hz, digitised and recorded using Spectra 3.013 software (Grove Medical, London, UK). Each infant was studied for 30 min.
Data analysis
Demographic and comparative data are summarised as medians, IQR and ranges. The timing and effect of the peak NIPPV pressures on spontaneous breathing were assessed by analysing the first 30 consecutive NIPPV pressure cycles in each recording, that were free of movement artefact, assessed by video and RIP and Graseby waveforms. Video, RIP and Graseby signal data were used to identify all recorded episodes of apnoea lasting at least 3 s. NIPPV pressure peaks delivered during periods of complete absence of respiratory effort, presumed central apnoea, were examined for any effect of pressure change on chest movement. Chest movement was quantified by comparison with an average of the five breaths immediately prior to each apnoea. Comparisons of medians were made using Mann–Whitney U and linear regression tests. Correlation analyses were made using Spearman's rank correlations. Analyses were performed using STATA V.10.
Results
Table 1 shows the demographic details of the 10 infants. The median (range) gestational age, birth weight, day of study and study weight were 25+3 (24+6 to 27+6) weeks, 797 (565–1103) g, 24 (7–57) days and 1076 (810–1280) g, respectively. Three infants were female and nine were studied prone. All had previously received endotracheal ventilation for a median (range) of 9 (1–55) days, and NIPPV for 9 (2–33) days. All were receiving caffeine.
Demographic data and NIPPV settings
Effect of NIPPV pressures on spontaneous breathing
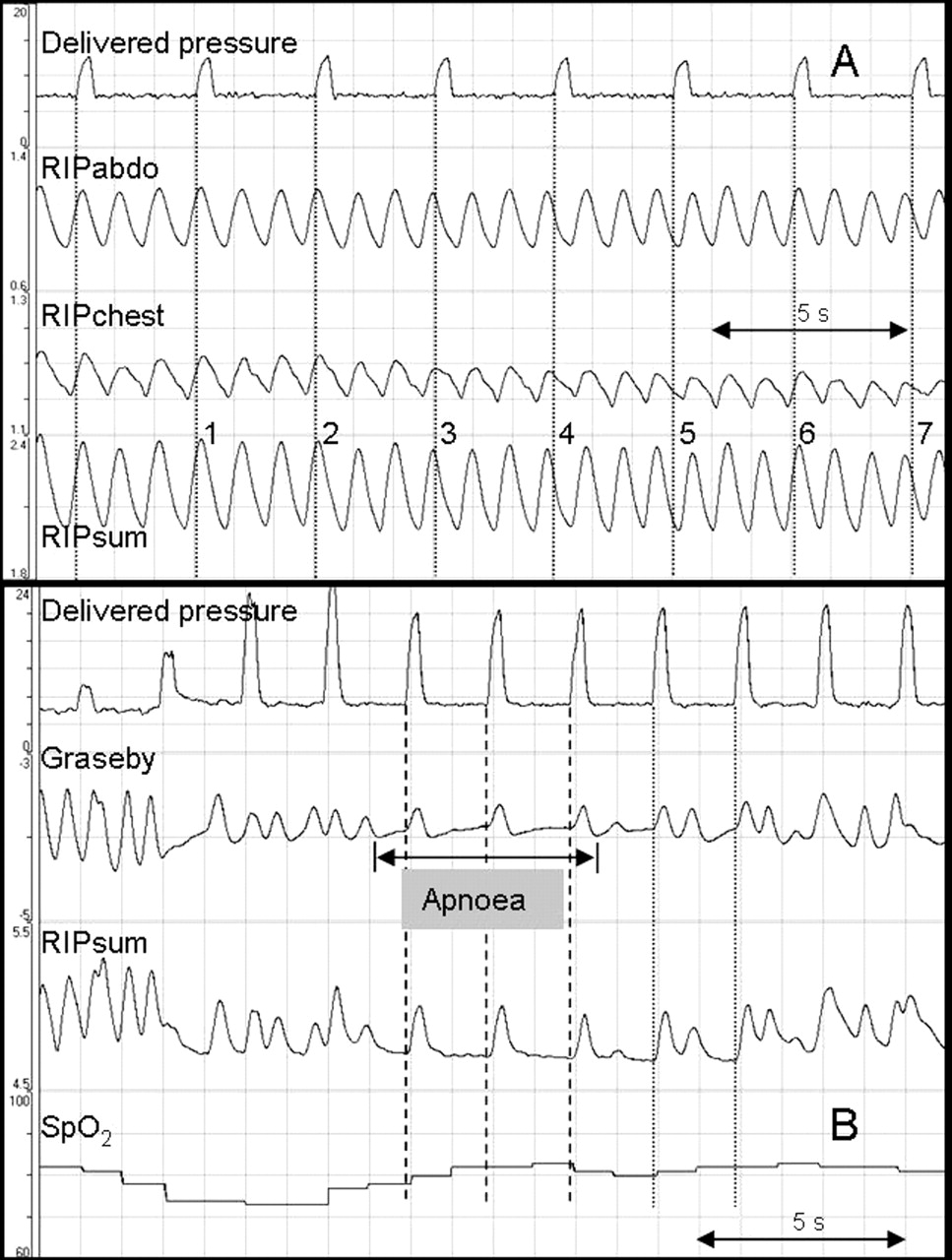
For the majority of each study the infants had stable RIPsum recordings, without any discernable influence from the NIPPV pressure peaks on the breathing pattern (figure 1A). In only two infants brief periods were identified where interruptions in the background breathing pattern correlated with pressure peaks. These lasted for 68 s in one infant and 15 s in the other. Figure 1B shows one of these episodes; the pressure peaks produced chest inflations between breaths, the volume of which increased as the NIPPV pressure increased.

Recordings showing examples of the effects of the applied pressure on spontaneous breathing: (A) an example of a typical recording, there is no apparent effect of the pressure cycles on the respiratory pattern, (B) extract from an atypical section of recording where applied pressures resulted in chest inflations in addition to the infant's spontaneous breaths. These extra ‘inflations’ initially produced tidal volumes half the size of the spontaneous breaths, their volume increased in size as the magnitude of the nasal intermittent positive pressure ventilation pressure peak increased, spontaneous respiratory rate fell to 29 breaths/min during this time (from 64 breaths/min) and SpO2 remained stable (C) an example demonstrating larger tidal volumes recorded when the onset of NIPPV pressure peaks (dotted lines) coincided with spontaneous inspiration.
Despite the overall lack of visible effect, NIPPV had some effect on spontaneous breaths. When the pressure peak commenced during inspiration the inspiratory time increased by 21% from 0.28 (IQR 0.25–0.32) to 0.34 (0.28–0.48) s (p=0.002) and relative tidal volume increased by 15% (0.33–0.38 mV, p=0.01), see figure 1C. There was no significant effect on expiratory time (0.52 s vs 0.55 s, p=0.13). When the pressure peak commenced during expiration the expiratory time increased by 13% from 0.52 (IQR 0.39–0.65) to 0.59 (0.45–0.77) s (p=0.04), see table 2.
Inspiratory and expiratory times, and relative tidal volumes, related to the onset of NIPPV pressure peaks
Effect of NIPPV pressures on chest inflation during apnoea
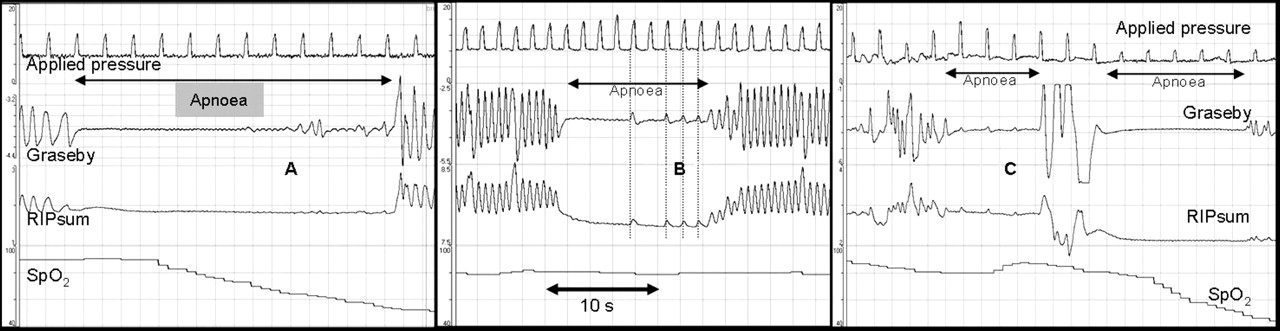
In all, 133 episodes of central apnoea were identified. These lasted a median of 6 s (range 3–40 s), with 13 episodes (range 1–27) per infant. The median proportion of apnoeas where some NIPPV pressure peaks produced some chest inflation was 19.1% (range 0–88%). During the apnoeas, 440 pressure peaks were delivered (1–99 per infant, median 38). Only 5% (range 0–32%) of the pressure peaks produced a deflection in the RIPsum recording, indicating chest inflation (see figure 2). They produced a median volume of 26.7% (IQR 19.1–60.3%) of the size of that infant's average spontaneous tidal volume over the previous five breaths.

Recordings showing various effects of nasal intermittent positive pressure ventilation (NIPPV) pressures during apnoea: (A) 11 pressure peaks delivered during apnoea, no chest inflation achieved, SpO2 falls to 45%. (B) Nine pressure peaks delivered during apnoea, four resulted in small chest inflations, SpO2 maintained at 80%. (C) Apnoea with three pressure peaks resulting in small changes in chest volume and stable SpO2, followed by a second apnoea, with NIPPV pressure peaks, no corresponding chest inflation and a fall in SpO2 to 42%.
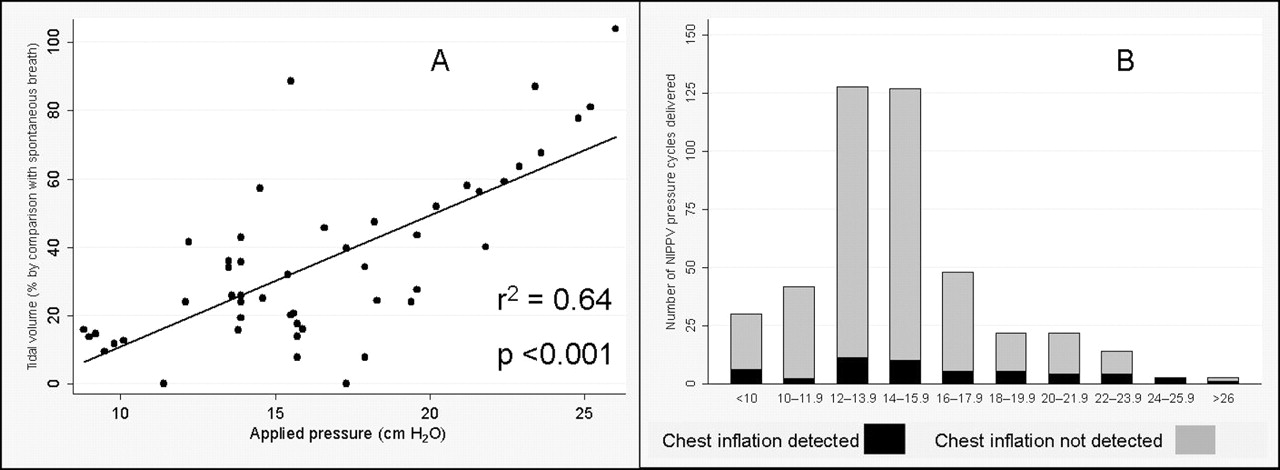
During apnoeas the peak NIPPV pressures with resulting chest inflation ranged from 8.0 to 28.1 (median 15.7) cm H2O and were not statistically different from the pressures delivered without corresponding chest inflation: 8.8–26.0 (median 14.2) cm H2O (p=0.06) (figure 3). There was no correlation between the peak pressure and likelihood of chest inflation occurring (r2=0.11, p=0.12). However, if chest inflation did occur, higher peak pressures resulted in larger tidal volumes (r2=64, p<0.001) see figure 4A. Seventy per cent of the data forming the basis of this calculation came from two infants who had several apnoeas exhibiting transmitted NIPPV pressures; therefore these data should be interpreted with caution.

Histograms comparing the peak nasal intermittent positive pressure ventilation pressures when (A) no chest inflation was seen, and (B) when corresponding chest inflation was seen.

Effects of nasal intermittent positive pressure ventilation (NIPPV) pressure peaks delivered during apnoea; (A) scatter graph of the correlation between the peak NIPPV pressures and tidal volumes when chest inflation did occur during apnoea, as measured in six infants and (B) histogram of the applied pressures delivered during apnoea (shown in 2 cm H2O increments), demonstrating the number of pressure cycles where chest inflation occurred.
Across the range of peak pressures delivered during apnoea (range 8.0–28.1 cm H2O), some peaks resulted in chest inflation and some did not. No pressure consistently produced chest inflation, or never resulted in chest inflation (figure 4B).
The severity of desaturations was assessed in apnoeas which lasted longer than 10 s (n=29). In 22 apnoeas where the NIPPV pressure peaks did not produce chest inflation the SpO2 fell by a median (IQR) of 21% (14–45). In seven apnoeas where the NIPPV pressures did produce chest inflation the SpO2 fell by 6% (2–13)% (p=0.01).
The CO2 ranged from 40 to 100 mm Hg. No infant had a CO2 range greater than 27 mm Hg during the study period, CO2 levels gently fluctuated and increased during apnoea. In five infants no apnoeas contained any pressure transmission to the chest. In the other five some apnoeas produced chest inflation and some did not; comparison of CO2 levels demonstrated mean CO2 levels during apnoeas without pressure transmission of 61.3 mm Hg and mean CO2 levels during apnoeas with pressure transmission of 62.0 mm Hg (p=0.50).
Timing of NIPPV pressure peaks with spontaneous breathing
The timing of the pressure cycles were examined to determine whether the onset of pressure rise commenced during spontaneous inspiration or expiration. Figure 5A is a typical recording showing onset of rise in NIPPV pressure occurring at all stages of the respiratory cycle. One recording (figure 5B) showed a 5-s apnoea where the pressure peaks produced chest inflation, followed by two pressure peaks which appeared to trigger spontaneous inspiration, regular breathing was then re-established. No other examples of infant breathing triggered by the ventilator were seen.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Example of a typical recording demonstrating the onset of rise in applied nasal intermittent positive pressure ventilation pressure occurring at all stages of the spontaneous respiratory cycle (1. late inspiration, 2. late inspiration, 3. peak of breath, 4. early expiration, 5. late expiration, 6. mid inspiration, 7. mid expiration) and (B) a recording showing the one example of a brief episode of apnoea where the applied pressure resulted in chest inflation and then appeared to trigger spontaneous inspiration twice, before regular respiration was re-established.
The median inspiratory and expiratory times during this study were 0.29 and 0.51 s, respectively (table 2), giving a total respiratory cycle time of 0.8 s; therefore inspiratory proportion was 36% and expiratory proportion 64%. The majority of breaths (median 65%) did not contain an NIPPV pressure peak. Of the remaining 35% of breaths; 40% had a pressure peak during inspiration and 60% during expiration. The distribution of the pressure peaks was proportional to the time infants spent in inspiration and expiration. Infants did not become entrained with the ventilator rate. The ventilator rate did not alter the proportion of pressures peaks delivered during inspiration.
Discussion
As survival of extremely preterm infants has improved, clinicians have sought techniques that support breathing while avoiding invasive techniques which may cause lung damage. NIPPV appears to provide additional support for very preterm infants who cannot manage with nasal CPAP alone. NIPPV may reduce intubation rates22 23 and two small studies report reduction in broncho-pulmonary dysplasia22 24 in infants with respiratory distress syndrome. Compared with CPAP, NIPPV reduces ‘failure’ rates following extubation.25 26 However, many questions remain about exactly how NIPPV works in neonates. Mechanisms of action of NIPPV in adults and children are relatively straightforward; synchronised pressure variations result in lung volume change, but due to differences in the delivery interface and difficulties with synchronisation, neonatal NIPPV may work quite differently.
Effects of NIPPV pressures on spontaneous breathing
During endotracheal ventilation, non-synchronised mechanical inflations can alter the background respiratory pattern.27 Similar effects could be expected to occur during NIPPV. If NIPPV increased lung expansion it could enhance or halt inspiration, or cause reflex laryngeal constriction. In this study it was usually not possible to see any effect of NIPPV pressure peaks on breathing patterns. However, analysis showed that the relative tidal volume increased slightly when the onset of pressure rise occurred during spontaneous inspiration. This suggests that timing the onset of pressure rise to correlate with every inspiration would be beneficial. This agrees with Moretti et al's20 observation that during ‘synchronised’ neonatal NIPPV only mechanical ‘inflations’ delivered during inspiration produced chest inflation. The finding that pressure peaks delivered during expiration slowed background respiratory rate was not unexpected, this is unlikely to be beneficial. Adult studies have demonstrated that non-synchronised NIPPV is less effective than synchronised NIPPV, particularly in certain sleep states.28 29 Application of these data to preterm neonates is limited by the lack of devices delivering synchronised NIPPV, and the lack of evidence that such devices achieve clinically important benefits in neonates.
In adults supported with synchronised NIPPV, upper airway dilatation due to pharyngeal muscle activity usually occurs prior to diaphragmatic contraction, so that NIPPV pressure peaks occurring after diaphragmatic contraction are likely to occur after the glottis has opened. In premature infants this sequence of muscle contractions is more variable with up to 60% of breaths commencing with diaphragmatic contraction in advance of glottic opening.30 Therefore using diaphragmatic contraction to trigger NIPPV pressure rise does not guarantee an open glottis. In addition, newborn infants and animals commonly have laryngeal abduction during expiratory braking31 and central apnoeas32 to preserve lung volume and protect against desaturation. This would limit the effects of NIPPV by preventing the applied pressures reaching the chest.
Effect of NIPPV pressures on chest inflation during apnoea
A small proportion of the pressure cycles delivered during apnoea produced small chest inflations. Lack of effect may have been due to insufficient pressure to inflate the chest, or obstruction due to a closed glottis. Ryan et al observed that pressures up to 20 cm H2O did not consistently produce chest inflation.33 We have demonstrated that pressures as low as 8 cm H2O produced some chest inflation about 20% of the time, and pressures as high as 26 cm H2O produced some inflation about 30% of the time. Lack of correlation between the peak pressure and the likelihood of chest inflation suggests that if airway obstruction were present then even high NIPPV pressures would not overcome it. These findings imply that when chest inflation occurred it was because the airway was patent. For NIPPV to be maximally effective it may be necessary to ensure that the airway is patent at the onset of the increase in applied pressure, this may not be possible during apnoea.
Although peak pressures did not often produce chest inflation during apnoea, analysis of longer apnoeas demonstrated that desaturations were less marked if NIPPV pressures lead to chest inflation. This supports a suggestion that NIPPV pressure changes reduce apnoea related desaturation, compared with CPAP.34 We have also shown that when the applied NIPPV pressures caused chest inflation during apnoea, the relative tidal volume produced was proportional to the applied pressure, that is, when the airway was patent, the higher peak pressures resulted in proportionally larger chest volume changes. However, in this study the vast majority of the NIPPV pressure peaks delivered during apnoea produced no chest inflation at all.
Carbon dioxide levels are very important during NIPPV. Adult29 35 and animal36 data have shown that hypocapnia during non-invasive ventilation caused reflex glottic constriction, reducing minute ventilation and limiting the effectiveness of NIPPV. Conversely hypercapnia activates the glottic dilator muscles and opens the larynx in both adults37 and neonates.38 In this study no infant was hypocapnic and transcutaneous CO2 levels were similar during apnoeas in which NIPPV pressures did and did not cause chest inflation. The small CO2 fluctuations seen during this study did not significantly affect delivery of NIPPV.
Timing of NIPPV pressure peaks with spontaneous breathing
It has been reported that infants become ‘entrained’ with both non-synchronised endotracheal inflations39 40 and non-synchronised NIPPV.21 If infants did become ‘entrained’ they would match their spontaneous respiratory rates to the ventilator rhythm. We hypothesised that if the NIPPV pressure peaks triggered spontaneous inspiration then the onset of the pressure peak would consistently occur at the end of spontaneous expiration, just prior to inspiration. However, if the infants became entrained by ‘anticipating’ when the NIPPV pressure would increase, then the onset of the pressure peak would consistently occur in early inspiration. These hypotheses were both proved to be incorrect as we found that the onset of the NIPPV pressure peaks were distributed evenly throughout the respiratory cycle, proportional to the time spent in inspiration and expiration, fitting neither theory and demonstrating no evidence of entrainment.
Reports of entrainment during NIPPV were during an NIPPV rate of 40 cycles/min21 and during endotracheal ventilation at rates of 60 and 120 inflations/min. Infants in this study had been on NIPPV for at least 2 days prior to the study, and had set rates of 10–40 cycles/min, no evidence of entrainment was seen at any of these rates. It may be possible that entrainment could occur at faster NIPPV rates.
The results from this study suggest that the onset of rise in pressure during NIPPV should occur when the airway is most likely to be patent, during inspiration. Tailoring NIPPV to achieve this may increase its effectiveness. Certainly during non-synchronised NIPPV the term ‘nasal intermittent positive pressure ventilation’ may not be entirely appropriate.
There have been concerns that non-synchronised NIPPV may result in high pressures being delivered during spontaneous expiration, resulting in increased upper airway and intrathoracic pressure, risking pneumothorax.41 42 We have demonstrated that for most of the time the NIPPV pressure peak did indeed occur during expiration, but as we did not measure oesophageal pressure we do not know whether high pharyngeal or intrathoracic pressures were induced. Reassuringly, there have been no reports of air leak, or recent reports of gastrointestinal perforation, attributed to non-synchronised NIPPV.
Abdominal pneumatic capsules have been used to attempt to synchronise the applied pressure rise with spontaneous breathing, but they are dependant on site of placement, are subject to movement artefact and may trigger during expiration.40 In neonates, only one small study using abdominal capsule ‘synchronised’ NIPPV has reported how well synchronisation occurred, reporting that 94% of pressure peaks were delivered during inspiration.43
Randomised trials in very preterm infants comparing ‘synchronised’ NIPPV with CPAP postextubation showed that NIPPV reduces re-intubations26 44,–,46 whereas the single published study using non-synchronised NIPPV found no advantage over CPAP.47 It remains unclear how much benefit, if any, non-synchronised NIPPV has over CPAP.
Conclusions
Non-synchronised NIPPV pressures did not ‘inflate’ the chest, unless the pressure peaks commenced during spontaneous inspiration, when a modest increase in inspiratory time and relative tidal volume were seen. During apnoea transmission of the pressure to the chest was uncommon, but when chest volume change occurred less oxygen desaturation resulted. Infants did not become entrained with the cyclical changes in applied pressure during non-synchronised NIPPV.
Methods to synchronise delivery of the NIPPV pressure peak with spontaneous inspiration may increase the benefits of NIPPV and should be investigated.
References
Footnotes
-
Funding LSO is part funded by a Royal Women's Hospital Postgraduate Research Scholarship. The research work is funded by an Australian NHMRC program grant number 384100.
-
Competing interests CJM was a consultant to Drager Medical.
-
Ethics approval This study was approved by the Research and Ethics Committees of the Royal Women's Hospital, Melbourne, Victoria, Australia: Project Number 07/03.
-
Provenance and peer review Not commissioned; externally peer reviewed.