Article Text

Abstract
Objectives To provide survival data and rates of severe disability at 2 years of corrected age in infants born prior to 26 weeks' gestation in 2001–2003 and to compare these outcomes with an earlier cohort from 1991 to 1993.
Design Population-based prospective cohort study.
Setting Former Trent region of UK covering a population of approximately five million and around 55 000 births per annum.
Participants The authors identified a 3-year cohort of infants born before 26 weeks' gestation between 1 January 2001 and 31 December 2003 from The Neonatal Survey (TNS). Questionnaires based on the Oxford minimum dataset were completed.
Main outcome measures Survival, service use and disability levels were compared between the 2001– 2003 cohort and the cohort from 1991 to 1993.
Results In 2001–2003, 0%, 18% and 35% of live born babies were alive at 2 years without any evidence of severe disability at 23, 24 and 25 weeks' gestation, respectively. Overall, of those children admitted to neonatal care, the proportion with no evidence of severe disability at 2 years corrected age improved from 14.5% in 1991–1993 to 26.5% in 2001–2003. There was an increase in the proportion of children with at least one severe disability, out of total admissions to neonatal unit (8% vs 17%) and of those assessed at 2 years (35% vs 39%).
Conclusions This study has shown an improvement in survival to discharge in babies admitted for neonatal care. However, this improved survival has been associated with an increase in the proportion of children with at least one severe disability at a corrected age of 2 years.
Statistics from Altmetric.com
Introduction
In the last 20–30 years there has been a rapid growth in the provision of care and dramatic improvements in the survival of preterm infants.1 During this time there has been considerable speculation about the extent to which any improved survival might have been at the cost of higher levels of disability in survivors. Results from previous population-based studies have varied. Some reports have found increasing levels of disability in parallel with improving foetal survival2 while others have shown both an improvement in the survival and reduced rates of cerebral palsy.3,–,5 However, direct comparisons of these various studies is difficult as outcome measures have not been consistent. Some studies have been based on very low birthweight infants, some have selected their population by early gestational age, while others use a combination of the two.
What is already known on this subject?
▶ There has been considerable speculation about whether improved neonatal survival might have been at the cost of higher levels of disability in survivors.
▶ Results from previous population-based studies have varied and direct comparison of these various studies is difficult as outcome measures have not been consistent.
What this study adds
▶ Routine follow-up data can be effectively collected from existing hospital notes, community childhealth records and special registers and this will facilitate national and international comparison of outcome of extremely preterm babies.
▶ Improved survival has been associated with an increase in the proportion of children with at least one severe disability at a corrected age of 2 years.
Information on late morbidity in survivors of neonatal intensive care is needed by several groups of people: by parents, so they can understand the possible consequences of survival in their baby and take informed decisions about their child's care; by the clinical team, for sharing with parents, for evaluating their service and for research; by commissioners of neonatal care and other services for children so that they can make informed decisions and plans; and by the general public so they can take part in an informed debate on priorities in healthcare. Although official reports since 1992 have highlighted the need for neonatal units and health authorities to collect information on later morbidity,6 it remains generally unavailable on a population basis or outside specialist centres.
In 1999, the authors published the results concerning the health status of a population of infants born before 26 weeks' gestation from the Trent health region during 1991–1993.7 Outcome data were collected from routine childhealth data systems at approximately 2 years corrected gestational age. This current study provides information on the outcome of extremely preterm births born from 2001 to 2003 in the same geographical region, thus providing an insight into the changes that have occurred over time.
Methodology
A population-based study of all babies born at or before 32 weeks has been running for the former ‘Trent’ health region since February 1990 (The Neonatal Survey [TNS]); covering a population of approximately five million and around 55 000 births per annum. Neonatal care for this former health region is now provided by the Trent, Central and North Trent Neonatal networks. However, the hospitals involved and the distribution of births remained largely unchanged.
TNS uses a standardised method of data collection. A number of neonatal nurses visit the units regularly and record information about pregnancy, delivery and care provided on the neonatal unit, for all infants meeting the criteria for inclusion in the study, including all admissions for neonatal intensive care for the cohort of interest: from 22+0 to 25+6 weeks' gestational age. In addition, since the inception of the Confidential Enquiry into Stillbirths and Deaths in Infancy (CESDI) in 1993, data for all outcomes of pregnancy for the extreme preterm birth cohort have been merged with TNS to provide a total cohort of very preterm births including those from 22+0 to 25+6 weeks' gestational age. Gestation was allocated using the following hierarchy; mother certain of dates (most reliable); early dating scan; late dating scan; postnatal examination (least reliable).
At the time of this study no data was routinely collected after discharge from the neonatal service.
The methodology for the 1991–1993 cohort is described in Bohin et al (1999)7 and was repeated for the more recent cohort. Using the TNS database the authors identified a 3-year cohort of infants born between 1 January 2001 and 31 December 2003 who delivered between 22+0 to 25+6 weeks' gestational ages. Follow-up information was collected for all surviving children from existing hospital notes, community childhealth records and special registers. A standardised questionnaire was designed based on the Oxford minimum dataset,8 which defines severe disability as abnormality in the form of either malformation (any malformation which despite physical assistance impairs the performance of daily activities), neuromotor function (inability to sit, to use hands to feed self, and to control head movement without support or having no head control), seizures (more than one seizure per month duration despite treatment), auditory function (hearing impaired, uncorrected even with aids), communication (inability to comprehend word/sign in cued situation, to produce less than five recognisable sounds or having no vocalisation), visual function (blind or seeing light only), cognitive function (about 12 months behind at 2 years or more than 3 SD below mean on standardised assessment), respiratory function (requiring continual oxygen therapy, mechanical ventilation), gastrointestinal function (requiring tube feeding, parental nutrition), renal function (requiring dialysis) or growth (height or weight more than 3 SD below mean for age). To aid comparison to the previous study the authors also included questions based on the Audit Commission criteria which defines severe disability as abnormality in the form of either developmental delay (delay of about more than two SDs on Griffiths scale), cerebral palsy (any neuromotor impairment, due to brain lesion), visual impairment (blind or seeing light only or corrected binocular visual acuity of 6/24 or less), hearing impairment (hearing loss uncorrected even with aids or loss more than 60 dB), epilepsy (a diagnosis of epilepsy needing regular medication) or others (breathlessness needing intervention in the form of, oxygen, ventilation or tracheostomy; hydrocephalus which has required shunt; presence of stoma and loss of limb). As for the 1991–1993 cohort, any information obtained from any review performed between corrected age of 18 months and 2 years was used to define the child's health status since we were unable to specify the age at which children were reviewed by local services.
For children who were under follow-up by one of the 16 hospitals within the region, a single observer reviewed all the hospital records. For children who had moved out of the area, where the child's new address could be located, the questionnaire was forwarded to a named consultant or health visitor for completion.
Multi-centre Ethics Committee permission was granted for the study.
Statistical analysis
The authors compared the outcome for the two periods of 3 years: 1991–1993 and 2001–2003 inclusive. The number and percentage of children with the specified impairments are reported. Overall differences between the two time periods were tested using χ2 tests. Differences between the two cohorts in the proportion of babies with specific impairments were not formally tested due to the missing outcome data in the earlier cohort. Measures of neonatal care provision are summarised using the observed median and range. Differences in length of stay for those admitted to neonatal care were tested using the Mann–Whitney U test.
Results
In the 2001–2003 cohort all the babies born at 20 and 21 weeks died before admission to neonatal unit (table 1). None of the babies born at 22 weeks and only two (7%) babies born at 23 weeks were discharged alive from the neonatal care, whereas, 31 (33%) and 72 (56%) of live births at 24 and 25 weeks, respectively, survived to discharge. After discharge to home, two more babies died before the age of 2 years.
Number and percentage of live born babies born at 20–25 complete weeks' gestational age by outcome in 2001–2003 cohort
One hundred of the 105 babies who were discharged alive from the unit were followed up at 2 years. Of the five children not assessed at 2 years, two had died, one could not be traced but was known to be alive at 2 years and two were lost to follow-up at 2 years but had been subsequently referred back with reported concerns and were assessed at 4 years. These five children were excluded from the analysis. Of the two children who were followed up later, the first child, born at a gestational age of 24 weeks, was reportedly unable to walk without assistance or aids, to have some difficulty locating mouth and facial features and to have normal vision with correction at 4 years of age. The second child, who was born at a gestational age of 25 weeks, was reported at the age of 4 years and 8 months to show definite left-handed preference and subtle right-sided hemi-paresis, to walk unsteadily and to have normal vision with correction and bilateral neurosensory deafness.
Survival to discharge for the two extreme preterm cohorts following admission to neonatal care increased from 27% (66/249) to 46% (105/230) over the study period. The total number of babies admitted for neonatal care was similar in the two time periods (249 in 1991–1993 and 230 in 2001–2003). There was evidence of an increase in length of stay in the later cohort from a median of 2 days to 5 days for babies who died before discharge and from a median of 102 days to 118 days for those discharged alive (table 2). The marked increase (1 vs 30 days) in the use of continuous positive airway pressure (CPAP) for extremely preterm babies discharged alive from neonatal care is almost certainly the result of better devices for the delivery of nasal CPAP being developed during the mid-1990s and greater confidence in this modality of respiratory support. There was no concomitant fall in the use of ventilation and this too is likely to have been influenced by changes to routine treatment (in particular increasing use of antenatal steroids and surfactant) combined perhaps with a greater willingness to treat babies at this gestation aggressively1.
Neonatal care provided to infants admitted below 26 weeks' gestation; 1991–1993 compared with 2001–2003
In the 1991–1993 cohort, seven of the 66 children who had been discharged alive from neonatal care died before the age of 2 years. Of the remaining 59 children, 55 were followed up at a corrected age of 2 years.
The health status at follow-up at 2 years corrected age for both the cohorts is described in table 3. There was an apparent increase in the proportion of children with cerebral palsy from 16% in 1991–1993 compared to 28% in 2001–2003 and the proportion of children without evidence of cerebral palsy remained fairly static at 75% and 72%, respectively. This result may be influenced by the five children of unknown outcome in the earlier cohort. In the later cohort, there was a decrease in abnormal outcome for severe breathlessness (33% vs 8%) as well as in developmental delay (31% vs 21%). There were no significant differences in terms of the incidence of abnormal outcomes for abnormal vision and loss of limb over the two time periods. There was a slight improvement in outcomes for the very preterm infants for other impairments (hearing, epilepsy, hydrocephalus and stoma).
Health status of children who were born extremely preterm assessed at 2 years corrected age; 1991–1993 compared with 2001–2003
Our questionnaire allowed us to estimate the levels of severe disability using the Oxford minimum dataset criteria. The proportion of children without severe disability out of total admissions to neonatal care was 29% by Oxford minimum dataset criteria, which was comparable to the 27% derived by the audit commission criteria (table 1).
As seen in figure 1, overall of those children admitted to neonatal care, the proportion with no evidence of severe disability at 2 years corrected age improved from 14% in 1991–1993 to 26% in 2001–2003 (p=0.0015). However, of those surviving children assessed at 2 years, this proportion decreased over the two time periods (66% vs 61%: p=0.58). Also, there was an increase in the proportion of children with at least one severe disability, both out of total admissions to the neonatal unit (8% vs 17%: p=0.0028) as well as those assessed at 2 years (34% vs 39%: p=0.58).

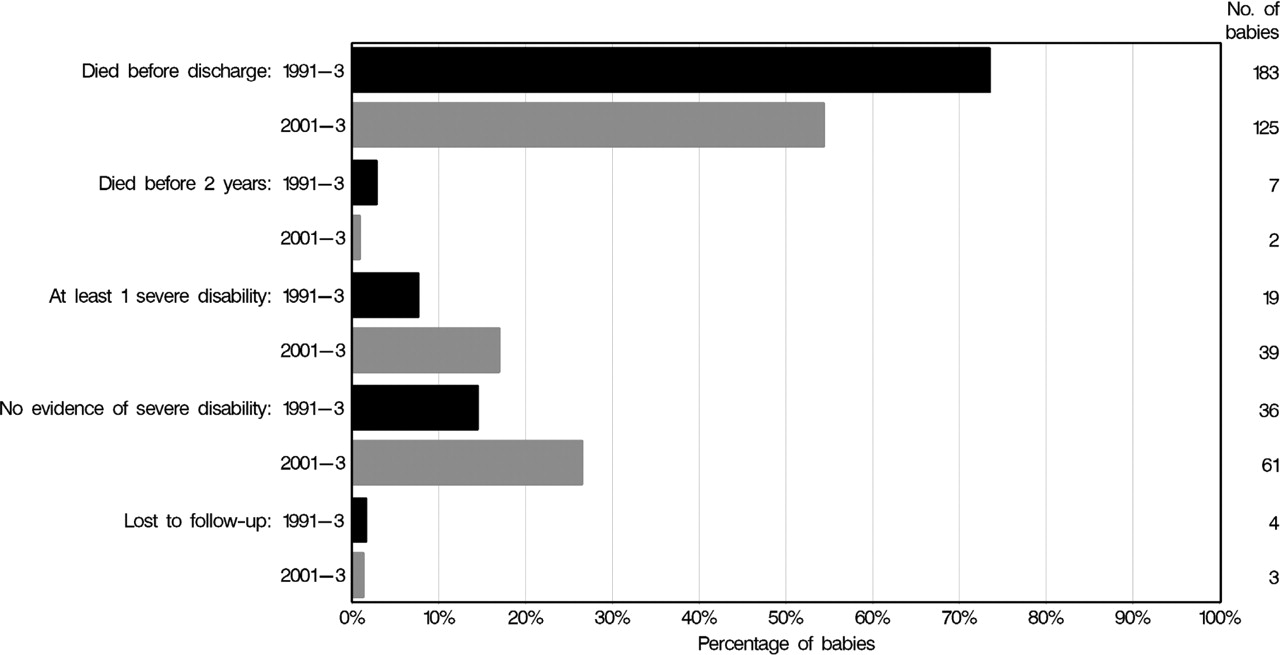{kind=link}
Summary of outcome at 2 years for extremely preterm neonates admitted to the neonatal unit.
Discussion
By comparing infants born during two 3-year time periods separated by 10 years, the authors have demonstrated an improvement in the proportion of babies admitted for neonatal care surviving to discharge. However, this improved survival has been associated with an increase in the proportion of children who at a corrected age of 2 years have at least one severe disability. TNS covers approximately one-tenth of the births for England and has been shown to be fairly representative of England and Wales as a whole.9 These results therefore have major national implications for health, social and educational services.
Large-scale population-based follow-up studies have provided us with valuable information about the outcome of extremely preterm babies in the recent years (table 4). Such studies are more reliable than neonatal unit based follow-up studies because they provide us with total birth cohorts that are not subject to referral bias. However, direct comparisons are only possible if data collection is standardised and adjusted for policy differences. Results from the EPICure study10 regarding the outcome at 30 months for babies born before 26 weeks in 1995 in UK and Ireland showed levels of severe disability comparable to our earlier cohort of babies born in 1991–1993. Results from a Dutch study11 that followed up a cohort of babies born during 1996–1997 at less than 26 weeks had results comparable with our later 2001–2003 cohort. The Victoria Infant Collaborative Study Group12 13 reported that in a cohort of babies born at less than 28 weeks in 2005, the level of disability had improved as compared to a similar cohort of babies born in 1997. In the Extremely Preterm Infants in Belgium (EPIBEL) study14 outcome at 3 years for a similar cohort of babies born in 1999–2000 in Belgium showed a survival to follow-up similar to our later cohort with decreased levels of severe disability. Direct comparison of these studies is difficult and the observed variations may be due to a wide range of factors including definitional, policy and measurement differences.
Comparison of survival and disability outcomes in various geographical cohorts in babies born at less than 26 weeks
Some studies of the outcomes of extremely preterm birth have selected their cohort by birth weight. However, the advantages of investigating outcome by gestational age rather than birth weight are well recognised15 as they are not affected by more mature small for gestation babies resulting in apparently better outcomes. Additionally, as foetal weight can only be estimated it is more practical to use gestational age for decision making and counselling prior to delivery. Our study collected information about the health status at corrected age 2 years for our very preterm cohort using a questionnaire based on the Oxford minimum dataset. This allowed us to collect data from routine sources using a reliable, validated tool. Results for the first cohort showed results similar to other large-scale population-based cohorts around that time. The latter cohort provides important information about the trends in survival and disability at 2 years. The need for a universally accepted tool to assess outcome is well recognised. Such a tool would have to be easily applicable and translatable into other languages and settings, require minimal resources and be able to provide necessary information in timely manner. The EUROPERISTAT16project has proposed a similar minimal follow-up set of indicators and this is currently being evaluated.
Major changes in neonatal intensive care provision occurred in the mid-1990s. Most importantly, the routine use of surfactant for pulmonary support of extreme preterm infants led to significant improvement in the survival of extreme preterm infants.17 Also, the introduction of the routine provision of antenatal steroids for women with threatening preterm delivery could also have influenced outcome,18 though there is no clear evidence for their usefulness in this extremely preterm group.19 The changes demonstrated in this study over the two time periods are most likely to be due to these two changes in care and the similarity between the EPICure results and our early cohort is probably explained by the fact that the routine introduction of these two prophylactic treatments was not well established until after 1995. Resuscitation practices vary around the world for babies born at the threshold of viability and have a direct impact on their reported survival and long-term outcome figures. In The Netherlands,20 neonatal intensive care is recommended from 25 weeks' gestational age and comfort care alone for babies of 24 weeks or less. In the UK, the recommendation from the Nuffield Council is to perform cardiopulmonary resuscitation (CPR) unless not indicated at 24 weeks with routine provision of CPR from 25 weeks.21 Work from New Jersey has shown that a more aggressive approach to resuscitating extreme preterm babies could improve survival at the cost of increased disability while a low intervention approach, common in The Netherlands produced a better quality of survival but at the expense of not resuscitating potentially viable infants.22 The longer length of stay in babies who died in the second period suggests this could be due to reluctance to withdraw care, indicating that attitudes towards the resuscitation of extremely preterm infants may have changed over the course of our study. However, despite the similar number of live births in our two cohorts, monitoring systems such as the CESDI now Centre for Maternal and Child Enquiries (CEMACE), which collect data on all stillbirths and neonatal deaths (providing information about deaths on the labour ward and resuscitation practices), are not available before 1993 and therefore a direct comparison of such changes is not possible. Up-to-date, standardised information concerning the resuscitation and subsequent survival and long-term outcome for these infants is required by both healthcare professionals and parents to facilitate decision making. The collection of routine follow-up data has been established as part of TNS and is being developed as part of the UK National Neonatal Audit Programme. Across Europe the EUROPERISTAT project has highlighted the increased resources required for the perinatal, neonatal and long-term care of very preterm infants and has developed an e-platform to facilitate standardised data collection and international comparisons.16
The main strengths of this study include our enrolment of all preterm births for two large population-based cohorts born 10 years apart for whom the authors have demonstrated changes in survival and disability levels at a corrected age of 2 years. The method of data collection was based on a validated minimum dataset enabling the collection of standardised information from routine sources. A weakness of the study was a small proportion of unknown outcomes in the earlier cohort. Follow-up at 2 years corrected age is a first step in the determination of the long-term outcome for these extremely preterm births for whom educational, psychological and behavioural problems are likely to be prevalent during the school years with a significant proportion having some functional limitations in their teenage years.23
Over the next year or so, outcomes at 30 months for very preterm infants from the second EPICure and the Swedish EXPRESS cohort24 should be available for confirmation of our results. To date, improved neonatal care has led to increased survival of extremely preterm infants. The next challenge for neonatal services is to decrease the long-term levels of disability in these children without compromising on the rate of survival.
Acknowledgments
The authors thank all the health professionals who were involved in the data collection.
References
Footnotes
-
Funding The Neonatal Survey is funded by Primary Care Trusts of the East Midlands and Yorkshire and additional data collection was funded by the University Hospital Leicester Service Delivery and Organisation Board.
-
Competing interest All authors declare that the answer to the questions on your competing interest form are all no and therefore have nothing to declare (available on request from the corresponding author).
-
Ethics approval Multi-centre Ethics Committee permission was granted for the study.
-
Provenance and peer review Not commissioned; externally peer reviewed.