Article Text

Abstract
Objective To investigate a method of minimally invasive surfactant therapy (MIST) to be used in spontaneously breathing preterm infants on continuous positive airway pressure (CPAP), evaluating the feasibility of the technique and the therapeutic benefit after MIST.
Design Non-randomised feasibility study.
Setting Tertiary neonatal intensive care unit.
Patients and interventions Study subjects were preterm infants with respiratory distress supported with CPAP, with early enrolment of 25–28-week infants (n=11) at any CPAP pressure and fractional inspired O2 concentration (FiO2), and enrolment of 29–34-week infants (n=14) at CPAP pressure ≥7 cm H2O and FiO2 ≥0.35. Without premedication, a 16 gauge vascular catheter was inserted through the vocal cords under direct vision. Porcine surfactant (∼100 mg/kg) was then instilled, followed by reinstitution of CPAP.
Measurements and results Respiratory indices were documented for 4 h following MIST, and neonatal outcomes ascertained. In all cases, surfactant was successfully administered and CPAP re-established. Coughing (32%) and bradycardia (44%) were transiently noted, and 44% received positive pressure inflations. There was a clear surfactant effect, with lower FiO2 after MIST (pre-MIST: 0.39±0.092 (mean±SD); 4 h: 0.26±0.093; p<0.01), and a modest reduction in CPAP pressure. Adverse outcomes were few: intubation within 72 h (n=3), pneumothorax (n=1), chronic lung disease (n=3) and death (n=1), all in the 25–28-week group. Outcome was otherwise favourable in both gestation groups, with a trend towards reduction in intubation in the first 72 h in the 25–28-week infants compared with historical controls.
Conclusions Surfactant can be effectively delivered via a vascular catheter, and this method of MIST deserves further investigation.
Statistics from Altmetric.com
Introduction
With the evolution and refinement of intensive care for preterm infants, the place of exogenous surfactant therapy is changing.1 The more widespread use of nasal continuous positive airway pressure (CPAP) for initial respiratory support means many preterm infants with respiratory distress now avoid intubation in the delivery room or in early postnatal life.2,–,4 This approach also means delaying or avoiding administration of surfactant. The potential advantages of early CPAP have been highlighted in two large randomised controlled trials in which treatment with CPAP from birth, without administration of surfactant, resulted in less ventilator days and a trend towards lower risk of chronic lung disease compared to intubated controls.5 6 It is conceivable, however, that outcomes in the CPAP group as a whole could be improved further if the subgroup of infants showing early signs of surfactant deficiency was to receive an early dose of surfactant.
What is already known on this topic
▶ Many preterm infants with respiratory distress are now managed from the outset on CPAP, and thus fewer infants with HMD receive surfactant at an optimal time.
▶ While there appear to be benefits from intubation with an endotracheal tube solely for surfactant administration, a simpler and less invasive technique to administer surfactant would be advantageous.
What this study adds
▶ Surfactant can be successfully administered to preterm infants without premedication using a narrow-bore vascular catheter passed into the trachea under direct vision.
▶ This technique of surfactant delivery produces a clear therapeutic benefit with reductions in FiO2 and CPAP pressure, and further evaluation of this method, ultimately including clinical trials, appears warranted.
Recognising the merits of surfactant, especially when given early,7,–,9 some clinicians choose to intubate infants on CPAP solely for the purpose of giving surfactant, followed by immediate extubation and return to CPAP.10,–,12 Several clinical trials of this technique have pointed to reductions in the need for subsequent mechanical ventilation and further surfactant therapy,13,–,17 and the risk of pneumothorax.17 A more recent study did not find a difference in the primary outcome of need for mechanical ventilation during the first 5 days, but 10% of those intubated solely for surfactant administration could not be extubated within 1 h and were thus deemed to have reached the primary outcome.18
Intubation of the trachea with an endotracheal tube can be hazardous,19 and is usually undertaken with premedication,20 which may contribute to a delay in extubation once surfactant has been administered. In view of this, less invasive methods of delivering surfactant have been pursued. Several techniques of what we term ‘minimally invasive surfactant therapy’ (MIST) have been described in which surfactant is delivered without tracheal intubation, including nasopharyngeal instillation,21 laryngeal mask placement22 and aerosolization.23 Currently, none of these methods appears ready for clinical application on a wider scale. Another method of MIST in which the trachea is catheterised with a 5–6 FG feeding tube has been reported24,–,27 and is undergoing further evaluation in clinical trials.27 The technical difficulties associated with this method, in particular the use of a highly flexible feeding tube and the need to use Magill's forceps to advance the tube tip into the trachea, may be limiting factors to its wider application.
Our research group has developed a technique of MIST (the Hobart method) in which surfactant is delivered into the trachea using a narrow-bore vascular catheter. Here, we describe a preliminary study of this technique in preterm infants with respiratory insufficiency. We aimed to establish whether the technique was feasible in preterm infants and evaluate the effect of the delivered surfactant. Our hypothesis was that exogenous surfactant could be effectively administered by the MIST technique, and that reductions in fractional inspired O2 concentration (FiO2) and/or CPAP pressure would follow.
Methods
This was a feasibility study conducted with the approval of the Institutional Ethics Committee. Written informed consent was obtained from the parents of enrolled infants. Infants between 25 weeks and 34 weeks 6 days gestation and less than 24 h of age were eligible if they were not intubated at birth, but showed evidence of respiratory distress necessitating the use of CPAP (eg, rib and sternal retraction, grunting respiration, requirement for oxygen). Infants with a congenital anomaly were excluded. For infants of 25–28 weeks gestation, enrolment was allowable immediately after birth once successfully resuscitated and spontaneously breathing on CPAP, regardless of oxygen requirement. For infants of 29–34 weeks gestation, minimum entry criteria were a CPAP pressure ≥7 cm H2O and FiO2≥0.35.
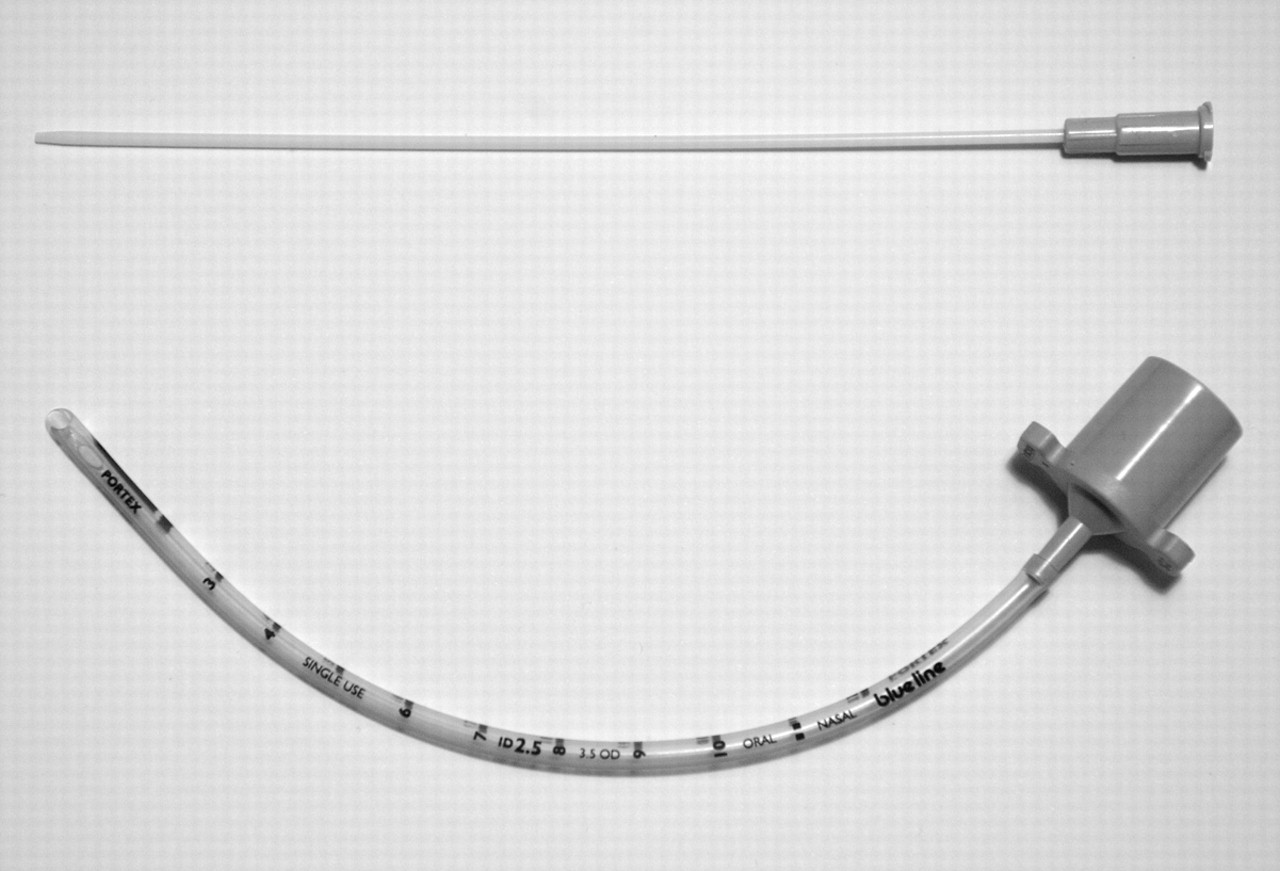
Exogenous surfactant administration via the new technique was performed once the infant was in a stable condition, with heart rate >120 bpm and oxygen saturation (SpO2) >85%. The procedure was performed with the infant either under a radiant warmer or in a humidicrib. No premedication was used. A 16 gauge (16G) vascular catheter 130 mm in length (16G Angiocath, BD, Sandy, Utah, USA) was used for the procedure (figure 1). The catheter was prepared by marking a point indicating the desired depth of insertion beyond the vocal cords with a marker pen. For infants 25–26 weeks this was 1 cm, 27–28 weeks 1.5 cm and 29–34 weeks 2 cm. Porcine surfactant (Curosurf, Chiesi Farmaceutici, Parma, Italy) at a dose of 100 mg/kg (1.25 ml/kg) was drawn up in a 3 ml syringe, and an additional 0.5 ml of air was drawn up into the syringe taking account of the dead volume of the instillation catheter.

Catheter used for MIST. Top: 16 gauge vascular catheter used for the MIST procedure, with external diameter of 1.7 mm. This catheter is semirigid and can be guided through the vocal cords without a trochar. Bottom: Standard 2.5 mm internal diameter endotracheal tube for comparison. This tube has an external diameter of 3.5 mm.
For the MIST procedure, the CPAP face mask or prongs were removed and direct laryngoscopy was performed using a standard laryngoscope and Miller 00 blade. The instillation catheter was inserted through the vocal cords to the desired depth and manually held in position at the lips. If catheterisation of the trachea was not possible within 20–30 s, face mask CPAP was briefly reinstituted followed by a further catheterisation attempt. After tracheal catheterisation, the surfactant syringe was then connected to the catheter hub, and the dose of exogenous surfactant administered in one bolus (25–28 weeks) or two boluses 10 s apart (29–34 weeks). The tracheal catheter was immediately withdrawn, and CPAP reinstituted by mask, with positive pressure inflations as necessary if the infant was apnoeic or bradycardic. Once re-stabilised, the infant was established on CPAP using Hudson binasal prongs (Hudson Respiratory Care, Temecula, California, USA). A video of the procedure is available as an online supplement to this article.
Management after MIST was as per standard practice at our institution, and was at the discretion of the treating clinicians. An arterial or capillary blood gas sample was taken around 2 h after the procedure. CPAP pressure was titrated according to work of breathing and oxygen requirement, with an oxygen saturation (SpO2) target of 88–92%. Maximum acceptable settings were a sustained CPAP pressure of 8 cm H2O (with pressures up to 10 cm H2O used for short periods), along with an FiO2 of 0.5. Infants exceeding these limits were intubated, and a further dose of surfactant was given if clinically indicated. Other indications for intubation were sustained respiratory acidosis (pH<7.2) and apnoea requiring repeated episodes of positive pressure inflation by mask. In those not requiring intubation, CPAP pressure was not reduced until FiO2 was below 0.25, that is, inspired oxygen was weaned before CPAP. Infants were treated with indomethacin if there was evidence of a haemodynamically significant patent ductus arteriosus (PDA). Screening for intraventricular haemorrhage (IVH) and retinopathy of prematurity (ROP) was done according to standard schedules.
Demographic and clinical data were collected prospectively, along with details of the MIST procedure, including number of attempts required to catheterise the trachea, and occurrence of coughing or gagging, surfactant reflux, bradycardia and need for positive pressure inflations. CPAP pressure, oxygen requirement and SpO2 were documented prior to and for 4 h after the MIST procedure. Partial pressure of carbon dioxide (PCO2) and pH values were compared in paired blood gas samples taken before and 2 h after MIST. The radiographic severity of hyaline membrane disease (HMD) was graded as mild, moderate or severe.28 Neonatal outcomes recorded were: need for intubation and mechanical ventilation in the first 72 h (and thereafter), further surfactant therapy, pneumothorax, PDA requiring indomethacin treatment, chronic lung disease (need for supplemental oxygen at 36 weeks corrected gestational age),29 IVH, ROP greater than stage 2 and survival to hospital discharge. Outcomes in study infants were compared with those of all like-gestation infants managed initially on CPAP in the years 2006–2008 (3 calendar years), excluding those with congenital anomalies and pulmonary hypoplasia.
As this was a feasibility study of a new technique, no formal sample size calculation could be applied. We chose to study 25 infants, and aimed to include at least 10 infants of 25–28 weeks gestation. In this report, continuous data are expressed as mean and SD and dichotomous outcomes as n (%). Effectiveness of surfactant delivery by MIST was assessed by comparison of SpO2, FiO2 and CPAP pressure before and after the procedure (paired t-test). Comparison of outcomes in study infants and historical controls was using OR and 95% CIs.
Results
In a 12-month period commencing in February 2009, 25 infants were recruited into the study of gestational age range 25–34 weeks and birth weight range 500–3000 g. Demographic and clinical characteristics for the different gestational age groups are shown in table 1. All 25–28-week infants were inborn, whereas 5 infants in the 29–34-week group were outborn and required transfer into our nursery because of respiratory distress.
Demographic and clinical characteristics
The MIST procedure was performed in the delivery room in 2 infants, and in the neonatal intensive care unit in the remaining 23. The procedure was performed by one of four neonatal Consultants (16 cases in total) or by a neonatal Senior Registrar (9 cases). Surfactant could be administered by the Hobart method in every infant, with two catheterisation attempts required in eight (32%). All infants were able to return to Hudson prong CPAP after the procedure. By virtue of the different entry criteria in the two gestation groups, the 25–28-week infants were treated relatively early, on average at 1.4 h, whereas the 29–34-week infants were treated at a mean of 9.4 h (table 2).
Details of MIST procedure
More of the 29–34-week infants required two catheterisation attempts. Coughing or gagging was noted in 32% of infants, with equal distribution among the gestation groups. Occurrence of bradycardia was similar in the two groups (44% overall), with recovery of heart rate above 100 bpm in all cases within 10 s. Positive pressure inflations were given to 44% of infants, for a longer duration in smaller babies.
There was evidence of a surfactant effect commencing within a few minutes of the MIST procedure. SpO2 increased following surfactant administration (figure 2A), with a more immediate response in 29–34-week infants than in the 25–28-week group (figure 3A). As a result, FiO2 could be reduced (figure 2B) and remained well below the baseline value at 4 h (pre-MIST: 0.39±0.092 (mean±SD); 4 h: 0.26±0.093; p<0.01). The FiO2 reduction was more rapid in 29–34-week infants, but by 60 min an apparent reduction in FiO2 was noted in both groups (figure 3B). Only for the 29–34-week group was the 4 h FiO2 value significantly different from baseline. CPAP pressure was also reduced after MIST (figure 2C), with values at 4 h being less than at baseline for the study group overall and for the 25–28-week group when analysed separately (figure 3C).

Respiratory indices before and after minimally invasive surfactant therapy (MIST) – all infants. Plot of SpO2 (A), FiO2 (B) and continuous positive airway pressure (CPAP) pressure (C) in all study infants before and for the first 4 h after the MIST procedure. Black arrow indicates the timing of MIST. *Value at 4 h differs from pre-MIST value, p<0.01.

{kind=link}
{kind=link}
{kind=link}
Respiratory indices before and after minimally invasive surfactant therapy (MIST), by gestation group. Plot of SpO2 (A), FiO2 (B) and continuous positive airway pressure (CPAP) pressure (C) in the two gestation groups before and for the first 4 h after the MIST procedure. Circles and dashed line: 25–28 weeks; squares and solid line: 29–34 weeks. Black arrow indicates the timing of MIST. *Value at 4 h differs from pre-MIST value, p<0.01; †p<0.05
For 17 infants (including four 25–28 weeks) paired blood gas samples were available (15 capillary, 2 arterial), with a lower PCO2 and higher pH noted at 2 h after the procedure (PCO2 pre-MIST: 54±8.0 mm Hg; 2 h: 49±8.1 mm Hg; p=0.014; pH pre-MIST: 7.29±0.046; 2 h: 7.32±0.036; p<0.01). Severity of HMD was mild in 1 (4%), moderate in 18 (72%) and severe in 6 (24%). In five cases there appeared to be some asymmetry of lung aeration after surfactant administration by MIST.
Outcome by gestation group is shown in table 3, including comparison with historical controls of similar gestation. Among study infants of 25–28 weeks gestation, three required intubation in the first 72 h of life, including one intubated and given surfactant at 12 h with severe HMD, and two others intubated beyond 48 h with recurrent apnoea. A further three infants were intubated at a later time with suspected sepsis. One of these had a pneumothorax noted as part of a terminal respiratory deterioration on day 13 in the context of Staphylococcus aureus septicaemia and cystic lung disease. Five infants in the 25–28-week group had a PDA treated with indomethacin, 2 had a germinal matrix haemorrhage (ie, grade I IVH) and 3 out of 10 survivors (30%) had chronic lung disease. As described above, one infant in the 25–28-week group died of respiratory complications.
Neonatal outcomes
Comparison was made with a control group of 25–28-week infants managed initially with CPAP in the period 2006–2008 (table 3). These infants were of gestation 27±0.96 weeks and birth weight 1070±220 g. There were no significant differences between the MIST-treated infants and historical controls for any outcome, but there was a trend towards a lower rate of intubation after MIST in the first 72 h (OR 0.26, 95% CI 0.058, 1.2).
Outcomes for infants of 29–34 weeks gestation treated with MIST were very favourable (table 3), with no infant requiring intubation, having a pneumothorax or developing chronic lung disease. Historical controls (gestation 32±1.7 weeks and birth weight 1790±510 g) had modest risk of each of these outcomes, in particular the need for ventilation (18%) and pneumothorax (7.6%). OR for these outcomes were not calculable given the null values in MIST-treated infants.
Discussion
Given the practical difficulties and potential hazards of endotracheal intubation in preterm infants, an alternative and less invasive means of surfactant delivery would be advantageous in infants on CPAP. We found the Hobart method of MIST using a narrow-bore vascular catheter to be feasible in infants of 25–34 weeks gestation, in all cases of successful catheterisation of the trachea, and return to Hudson prong CPAP after the procedure. There was clear evidence of surfactant delivery to the lung, with reductions in FiO2 and CPAP pressure in the 4 h after the procedure.
Use of nasal CPAP as the initial means of respiratory support for preterm infants has become commonplace, and with this approach up to 50% of infants of 25–28 weeks gestation can avoid intubation during their primary hospitalisation.5 30 On the other hand, the risk of pneumothorax with early CPAP may be higher,5 possibly as a consequence of the avoidance of exogenous surfactant in these infants unless they require intubation. Exogenous surfactant therapy is clearly associated with a reduction in the risk of pneumothorax,7 especially when given early. The delivery of surfactant with a minimally invasive technique in spontaneously breathing infants on CPAP would seem a logical additional therapy in this group, potentially preventing pneumothorax whilst at the same time avoiding intubation with an endotracheal tube.
Several techniques of MIST have been described, including those not involving tracheal catheterisation21,–,23 and others where the trachea is briefly catheterised.24,–,27 First described in 1992,24,–,27 the technique of tracheal catheterisation with a small bore feeding tube has been evaluated in more than 300 infants, and clinical trials using the technique are underway. This method uses a highly flexible catheter requiring the use of Magill's forceps to pass the tip into the trachea. Many neonatologists and trainees practice oral intubation,31 and are thus unfamiliar with Magill's forceps, and may find them cumbersome and difficult to use. The semirigid narrow-bore vascular catheter used in the present study can be passed straight along the laryngoscope blade in the line of sight to the vocal cords. In this sense, the technique is potentially easier than intubation with a standard endotracheal tube, which tends to obscure the view of the vocal cords when passed in line with the laryngoscope blade, especially in small infants. The tip of the vascular catheter can also be manipulated through the vocal cords without the need for Magill's forceps.
Coughing and gagging were noted in some infants, mostly after instillation of the surfactant. These responses, which have been noted by other investigators,25 did not appear in any case to cause sufficient surfactant reflux to prevent a therapeutic effect. Bradycardia was also noted in some infants, in particular with direct laryngoscopy, but in no case was sustained for more than 10 s. This reflex response may be ameliorated to some degree by atropine, which was used in the initial report of Kribs et al,25 and may explain the lower rate of bradycardia observed in that study (7.4%) compared to our own (44%). The incidence of bradycardia was also higher than that reported in studies of endotracheal intubation,19 20 again attributable at least in part to the use of premedication.20 The short-lived adverse effects we noted did not prevent return to CPAP in any of our study infants. The physiological changes during MIST, and their potential consequences, will require further evaluation as the technique is applied in a larger number of infants.
We successfully performed the Hobart MIST method in infants up to 34 weeks gestation. Other investigators have suggested that MIST may be poorly tolerated in infants beyond 28 weeks gestation32 and have proposed that these infants may require intubation for surfactant delivery. The proportion of infants 29–34 weeks requiring two catheterisation attempts (43%) was certainly greater than that noted by Kribs et al in infants of 23–27 weeks gestation (17%)25 and was also higher than for the 25–28-week infants in our study (20%). Overall, the proportion of cases requiring a second catheterisation attempt (32%) compared favourably with the corresponding value reported for neonatal endotracheal intubation (∼43%).20 We did not observe any episodes of significant physiological deterioration attributable to repeated catheterisation attempts, and positive pressure inflations were required only briefly. Nonetheless, infants of more advanced gestation may benefit from some form of short-acting premedication prior to MIST, for example, inhaled nitrous oxide,33 possibly supplemented by the use of topical anaesthetic.34
The sustained reduction in FiO2 after MIST indicates that an adequate dose of exogenous surfactant was delivered, overcoming some of the atelectasis related to high surface tension in the airspaces of the surfactant-deficient lung. Even in instances where surfactant reflux into the oropharynx was noted, significant reductions in FiO2 occurred, suggesting deposition of a sufficient quantity of surfactant into the lung. A satisfactory physiological response to surfactant was also seen in the infants in whom there was radiographic asymmetry of lung aeration suggesting uneven surfactant delivery, a phenomenon previously reported after conventional surfactant instillation in intubated infants.35
This study has the limitation of being a non-randomised investigation of a relatively small number of preterm infants, with comparison of outcomes with historical controls. Definitive evaluation of the benefits of the Hobart method will only come from randomised controlled trials comparing MIST with standard approaches to management of preterm infants managed initially with CPAP. An important potential advantage of MIST to be further explored is that surfactant administration in a spontaneously breathing subject would appear to result in more effective dispersion and greater tissue incorporation of phospholipid than when administered during mechanical ventilation.36
We conclude that surfactant can be effectively delivered to preterm infants with a minimally invasive technique using a vascular catheter. Further studies are now required to confirm the safety and applicability of this technique of MIST, and, ultimately, randomised controlled trials will be necessary to assess the impact upon neonatal outcomes such as pneumothorax, need for intubation and chronic lung disease.
References
Supplementary materials
Web Only Data 10.1136/adc.2010.192518
Files in this Data Supplement:
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval This study was conducted with the approval of the Human Research Ethics Committee Tasmania.
-
Provenance and peer review Not commissioned; externally peer reviewed.