Article Text

Abstract
Although survival rates for preterm infants have greatly improved over the last three to four decades, these infants remain at risk of developing a broad range of short-term and long-term complications. Despite the large body of work on the clinical sequelae of preterm birth, relatively little is known about its economic consequences. This paper represents a structured review of the recent scientific literature on the economic consequences of preterm birth for the health services, for other sectors of the economy, for families and carers and, more broadly, for society. A total of 2497 studies were identified by a pretested literature search strategy, 52 of which were included in the final review. Of these 52 studies, 19 reported the costs associated with the initial period of hospitalisation, 35 reported costs incurred following the initial hospital discharge (without providing costs for the entire remaining period of childhood), four of which also reported costs associated with the initial period of hospitalisation, while two reported costs incurred throughout childhood. The paper highlights the variable methodological quality of this body of literature. The results of the studies included in the review are summarised and critically appraised. The paper also highlights gaps in our current knowledge of the topic and identifies requirements for further research in this area.
Statistics from Altmetric.com
Introduction
Preterm births are defined as those before 37 completed weeks' gestation, with very preterm (VPT) births occurring before 32 weeks' gestation and extremely preterm (EPT) births before 28 weeks' gestation.1 The incidence of preterm birth has been reported at between 5% and 11% throughout the industrialised world with some of the highest rates reported in the United States.2 In the United Kingdom, approximately 7% of births are preterm.1 The incidence of preterm birth has increased slightly since the 1980s, which has been attributed to increasing rates of multiple births, greater use of assisted reproduction and increased obstetric intervention, such as induced labour and caesarean section.3 4 Developments in clinical practice, such as the use of ultrasonography to estimate gestational age, may also have had a slight effect on the incidence rate as may the trend towards registering a live birth for infants born at the limits of viability whose deaths might previously been classified as stillbirths or spontaneous abortions.3 Preterm birth has been associated with socioeconomic disadvantage, non-white ethnic background, substance misuse and extremes in maternal age, with both teenage and older mothers at an increased risk.5 6
Although survival rates for preterm infants have greatly improved over the last three to four decades, these infants remain at risk of developing a broad range of short-term and long-term complications.6 Infants born at the lower limit of viability have the highest morbidity and disability rates. A substantial body of literature has reported that extremely preterm infants are at an increased risk of a range of adverse neonatal outcomes including chronic lung disease,7 severe brain injury,8 retinopathy of prematurity,9 necrotising enterocolitis10 and neonatal sepsis.11 In later life, these infants are also at an increased risk of motor and sensory impairment,12 13 learning difficulties14,–,18 and behavioural problems.19,–,22
Despite the large body of work on the clinical sequelae of preterm birth, relatively little is known about its economic consequences. This paper represents a structured review of the recent scientific literature on the economic consequences of preterm birth for the health services, for other sectors of the economy, for families and carers and, more broadly, for society. It highlights gaps in our current knowledge of the topic and identifies requirements for further research in this area. It represents an update of a previous review article published by one of the authors (SP).23
Methods
A number of computerised databases were searched to identify relevant economic studies. These included Medline, CINAHL, EconLit, Science Citation Index (SCI), Social Science Citation Index, Index to Scientific and Technical Proceedings (ISTP), British Library Inside Information (BLII), EMBASE, Cochrane Library (CDSR), York Database of Abstracts of Reviews of Effectiveness (DARE), NHS Economic Evaluation Database (NEED) and the Database of Consortium of University Research Libraries (COPAC). The search terms applied to all electronic databases were developed and tested on Medline and eventually included all minor and major topics covered by MeSH terms for ‘preterm birth’, ‘prematurity’ and ‘low birthweight’ combined with ‘cost’, ‘economic’, ‘financial’ and ‘burden’. The reference lists of all papers identified by the searches were scrutinised for additional studies. The original structured review covering the period 1980–199923 was updated to include the period January 2000 to June 2009. Studies were excluded from the literature searches if they had been conducted in non-developed countries (defined, for the purposes of this review, as countries outside of the Organization for Economic Co-operation and Development (OECD)), if the abstract had not been published in the English language or if the focus was animal research. The title and abstract of each study identified by the literature searches were screened using predetermined criteria with the full report included in the final review if it explicitly described, measured and valued the economic implications of care provided to preterm (<37 weeks' gestation) or low birthweight (<2500 g) infants. Studies of the economic consequences of low birth weight were included in the review in order to capture potentially relevant information from eras and contexts of uncertainty in and incomplete recording of estimates of gestation. Cost data extracted from studies were converted from their respective currencies into UK pounds sterling using purchasing power parities supplied by the OECD (unless otherwise stated). Once converted to UK pounds, the cost data were inflated to 2008 prices using the NHS Hospital and Community Health Services Pay and Prices Inflation Index (unless otherwise stated).24
Results
A total of 2497 studies were identified by the combined literature searches, 52 of which were included in the final review. Of these 52 studies, 19 reported the costs associated with the initial period of hospitalisation,10 25,–,42 35 reported costs incurred following the initial hospital discharge (without providing costs for the entire remaining period of childhood),27 36 41,–,73 four of which also reported costs associated with the initial period of hospitalisation,27 36 41 71 while two reported costs incurred throughout childhood.5 74
Before proceeding to discuss the results of the studies included in this review, a brief note is required on their methodological quality. Of the 52 studies, 21 were based on geographically defined cohorts of infants.28 29 31 33 35 39 41 42 48 50 60 61 63 64 66 68,–,73 The remaining studies were largely based on hospital-specific or convenience samples and, consequently, were likely to have been prone to selection biases. None of the studies included in this review used primary research alone to derive all resource use and unit cost data inputs, with all studies making use of existing accounting, administrative or clinical records. Eleven of the studies included in the review cite charges for care rather than costs and may therefore have included elements arising from corporate financial decisions.27 33 43 45 51 53 55 64 65 72 73 Twelve studies that estimated long-term costs failed to specify whether they applied a discount rate to costs accruing beyond the first year of life.27 41 49 50 53,–,55 57 59 64,–,66 The practice of techniques, such as sensitivity analysis, that explore the implications of sampling or parameter uncertainty were only applied by 16 studies.29 30 32 39 41 42 46 47 49 55 60,–,62 65 66 74
Costs associated with the initial hospitalisation
Building on the work of two previous review articles,23 75 the characteristics of studies reporting costs associated with preterm birth during the infant's initial hospitalisation are summarised in table 1. The hospital costs associated with the initial hospitalisation varied between £584 per term born infant41 and £317 166 per extremely preterm survivor.10 There are several potential sources of the variability in these cost estimates. They include the wide time frame over which studies were conducted, with many older studies conducted before the diffusion of effective perinatal practices, such as the use of antenatal corticosteroids, new modes of ventilation, exogenous surfactant and better parenteral nutrition. They also include the geographical diversity of studies, which might reflect variations in healthcare practices and organisational models, and variations in the reporting of costs by gestational age versus birth weight. Nevertheless, when studies were analysed according to date of publication, country of publication or broad costing approach, a consistent inverse relation was identified between gestational age at birth and hospital costs associated with the initial hospitalisation. A similar inverse relation was identified between birth weight and hospital costs associated with the initial hospitalisation.
Studies reporting the costs of initial hospitalisation (studies since 1980)
A second theme of this body of literature is that initial hospitalisation costs are likely to be related to the mortality of infants. Some studies have estimated costs separately for infants who died, and the estimates for low gestational age or birthweight infants show that the cost is usually higher for survivors than for those who die.76 The implication is that initial hospitalisation costs will increase as a consequence of the improved survival chances of the smallest infants.
A third theme of this body of literature is that hospital costs associated with the initial hospitalisation are related to the degree of surgical intervention performed on the infant and the level of assisted ventilation received by the infant. Several studies provide detailed information on resource utilisation, thereby circumventing the need to place an economic value on each unit of resource use.25 29 31,–,33 35,–,39 41 42 Most commonly, they estimate numbers of days of assisted ventilation or overall length of stay for each group of infants. Mean overall length of stay varied between 1.8 days for term born survivors31 and 128 days for infants born at 23 gestational weeks (inclusive of survivors and non-survivors).36 When the data were analysed by birth weight, mean overall length of stay varied between 1.7 days for infants born at 3000–4500 g33 and 125 days for infants born at less than 500 g (inclusive of survivors and non-survivors).36
Recent studies have moved beyond solely estimating the economic burden of preterm birth towards estimating potential savings, both in terms of costs and lengths of stay, of incremental increases in gestational age for preterm infants.35 36 The purpose is to provide population-based data that can be used to assess the potential economic benefits of interventions that delay premature delivery. As such, the data are more amenable for economic evaluation, which focuses on incremental costs and incremental health gains associated with healthcare activities. An interesting example of this line of inquiry is the study by Phibbs and Schmitt.35 Using cohort data for all births in California in 1998–2000, the authors estimated that median savings for a two-week increase in gestational age at birth were between $28 870 and $64 021 for gestational ages below 33 weeks, with larger savings for longer delays in delivery (2003 prices). Delaying deliveries less than 29 gestational weeks to term resulted in savings of over $122 000 per case, with the savings being over $206 000 per case for deliveries less than 26 gestational weeks.
Four studies estimated non-healthcare costs associated with the initial period of hospitalisation.26 30 34 41 The most recent study from Finland valued mean direct non-medical costs and lost productivity before discharge of parents of extremely low birthweight infants at €2755 or 4% of total costs (1997 prices).41 Travel costs constituted the main cost component of non-healthcare costs, representing 64%, with the remainder attributed to lost earnings (30%) and family accommodation costs (6%). An earlier study from the UK considered the travel costs of visiting children in neonatal care and reported that more than one-third of families travelled more than 21 miles, with most (88%) visiting daily, and that median total expenditure was £100–£200 at 1990 prices.34
Costs following the initial hospital discharge
The characteristics of studies reporting costs associated with preterm birth following the infant's initial hospital discharge are summarised in table 2. There was considerable variation in the estimates of healthcare costs following the initial period of hospitalisation, though it is difficult to make direct comparisons between the cost estimates since the cohort specification, cost categories, costing methodologies and time periods of data collection were rarely comparable. Furthermore, some studies used low birth weight as a proxy for prematurity, thereby focusing on a group of infants heterogeneous for fetal development and potentially missing important economic consequences of preterm birth.
Studies reporting costs after initial discharge (studies since 1980)
The cohort dates of the studies span 1970 to 2004, over which time there have been several developments in health care, special needs education and social services, which may affect the cost of their provision. Mortality and morbidity outcomes have also changed over this time period, which is likely to have had an impact on the demand for services following the initial hospital discharge. Thus, the applicability of the earlier studies to the current context may be limited.
The majority of studies focused on healthcare costs, and sometimes only hospital costs, though over different follow-up periods. The results showed that healthcare costs following the initial hospital discharge are inversely related to gestational age at birth and birth weight. For example, McLaurin et al analysed data in a large national US database of commercially insured members and found that total first year costs were approximately three times higher among late-preterm infants than term infants, associated with higher morbidity among the preterm infants and increased re-hospitalisations.56 The most frequent cause for re-hospitalisation was respiratory distress and digestive disorders (including gastrointestinal illness). Similarly, Underwood and colleagues, building upon the work of other researchers,60 61 analysed Californian newborn hospital discharge records over the period 1992–2000 and found a clear inverse relation between gestational age at birth and the mean number of days of rehospitalisation over the first year of life with, again, respiratory disease being the most common cause of re-hospitalisation.71 Total rehospitalisation costs were highest among infants born at 35 weeks' gestation because of the larger number of infants born into this category than those born at more extreme gestations.
Several studies included in the review focused on costs over the first year or first two years of life.27 36 41,–,43 45 46 50 53,–,57 64 65 67 71 Others estimate costs over a further extended time horizon,44 48 51 60,–,63 68,–,70 72 73 though the studies with the longer follow-up periods showed that the majority of healthcare costs occurred during the first 12 months of life. A series of studies from a group based in Merseyside, England, reported on the costs associated with a population-based cohort of low birthweight infants (<2000 g) born between 1979 and 1981.68,–,70 For those low birthweight children without a disability the cost of hospital and family practitioner services was higher than for normal birthweight controls with the mean costs for the 8–9 year follow-up period estimated at £253 for those born at less than 2000 g, compared to £181 for those born at normal birth weight (at 1979 prices).69 The costs were substantially higher for children with disabilities; the estimated mean health service costs over the 8–9-year follow-up period were £3475 for those born at less than 1000 g, £2886 for those born at 1001–1500 g and £1719 for those born at 1501–2000 g (at 1979 prices).70
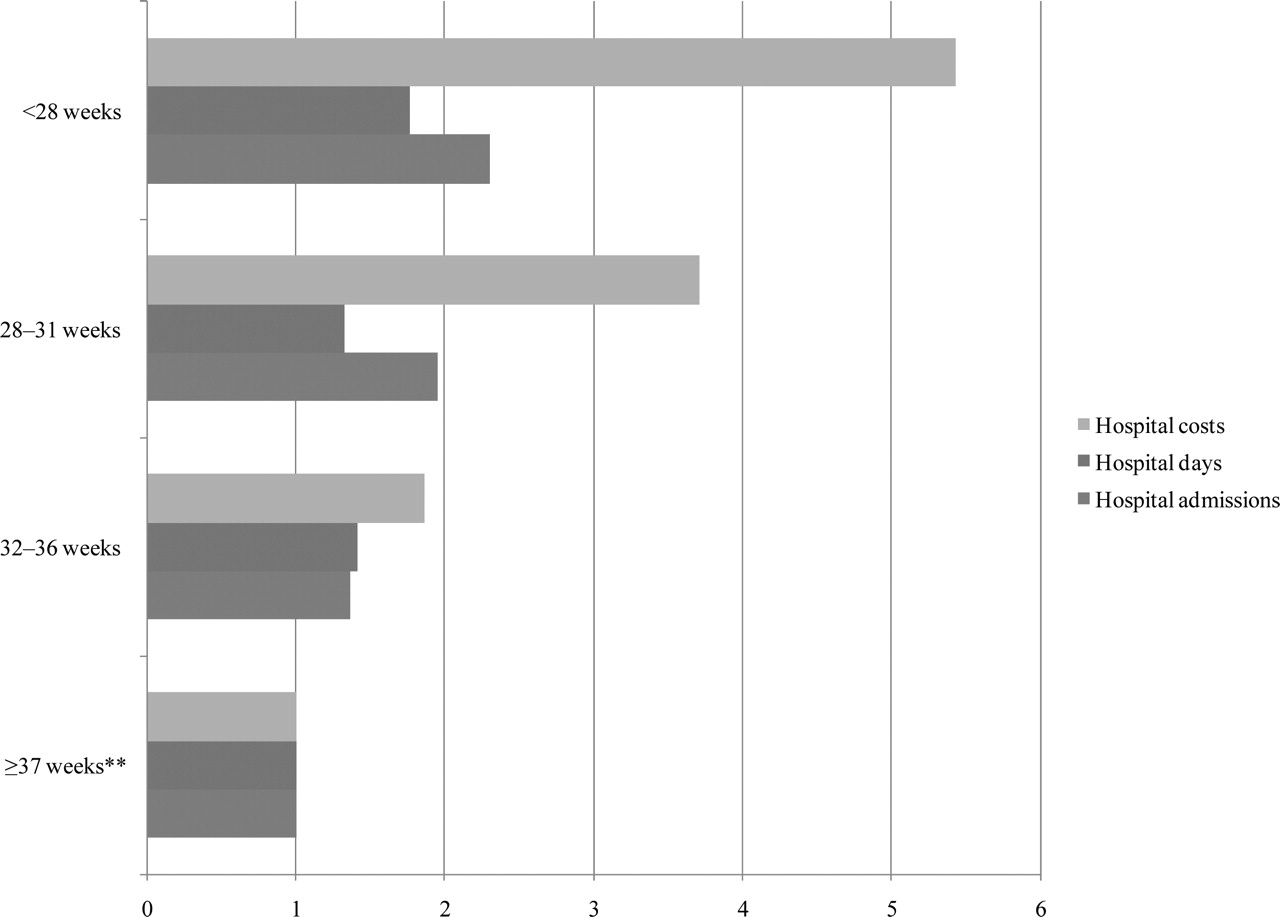
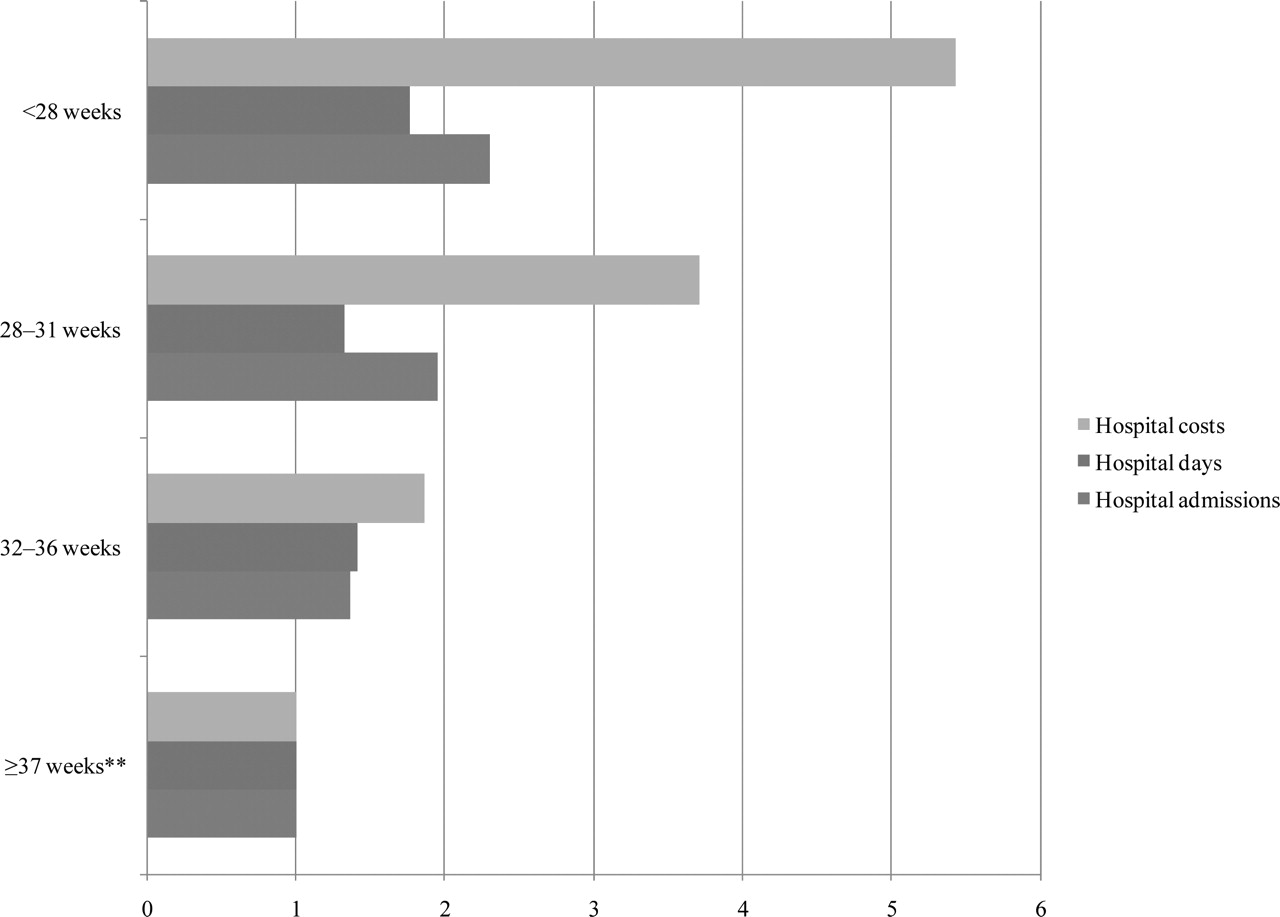
Petrou and colleagues performed a number of empirical studies based on data extracted from the Oxford Record Linkage Study, a large collection of linked, anonymised birth registrations, death certificates and statistical abstracts of NHS hospital inpatient and day case admissions for part of southern England.60 61 A multivariate negative binomial regression performed on the 5-year hospital service utilisation profile of 239 694 infants born in Oxfordshire and West Berkshire during 1970–1993 revealed that the total duration of hospital admissions for infants born at < 28 and at 28–31 gestational weeks was, respectively, 85 and 16 times that for term infants, once duration of life had been taken into account.61 A subsequent multi-level multiple regression model revealed that the adjusted effect regarding hospital inpatient admissions, days and costs over the first 10 years of life was 2.30, 1.77 and 5.43, respectively, for children born at <28 weeks' gestation when compared to children born at term (figure 1).60
{kind=link}
Adjusted effects regarding cumulative hospital inpatient admissions, days and costs over the first 10 years of life based on evidence from the Oxford Record Linkage Study, calculated using multi-level multiple regression.* (*Multiple regression controls for the following confounding factors: parity, maternal weight at first antenatal visit, the number of cigarettes smoked by the mother during pregnancy, maternal hospitalised days during pregnancy, complications of delivery, maternal operations during delivery, mode of delivery, multiplicity of birth, whether the child was small for gestational age, maternal age at the time of delivery, social class based on the male partner's occupation, whether the child was adopted or fostered around the time of birth and the duration of survival. **Reference category.) Source: Petrou60
Ten studies included in our review considered the education costs associated with preterm birth.44 47 51 53 62 63 66 68 70 72 Roth et al analysed birth and school records for 120 554 children born in Florida between September 1990 and August 1991 and found that the mean costs of kindergarten for those children born with birth weights of less than 1000 g were 60% higher than those born with birth weights over 2500 g.66 Chaikind and Corman reported that children born at less than 2500 g were 50% more likely to be enrolled in any type of special education programme than children who were of normal birth weight.47 Stevenson et al estimated the cost of special educational services for those children in the Merseyside cohort born at very low birth weight in 1979–1981 with disabilities. The mean cost estimate of net educational services provided until 8–9 years of age (approximately five years of education) was £10 083 in 1979 prices.70 More recently, the work by Petrou et al on the annual societal costs of care during the sixth year of life of children in the EPICure Study found that education costs for those born extremely preterm were £4150 greater than for the control group born at term (2003 prices).62
A relatively small number of studies considered broader societal costs attributable to preterm birth such as out-of-pocket expenses borne by families and opportunity costs associated with lost productivity. A study by McCormick et al from the USA was the main paper reported, with travel costs to health and social care providers averaging $15 per month, child care costs averaging $47 per month and other expenses averaging $62 per month during the first year of life following discharge from a neonatal care unit of a cohort of low birthweight infants (price date not reported).55 The study conducted by Tommiska et al in Finland reported wage losses by parents during the first year at €5990 for infants with birth weights of less than 1000 g compared to a much smaller loss of €880 for the normal birthweight control group (1997 prices).41 Finally, Petrou et al considered household expenditures and lost productivity associated with caring for children in the EPICure Study.62 They found that the annual additional expenditures for families of the extremely preterm children averaged £453 and that annual additional lost earnings associated with attendance at health appointments as a results of the children's ill-health averaged £39 during the sixth year of life (in 2003 prices).
Costs throughout childhood and beyond
Two studies included in the review estimated in a detailed manner the costs associated with preterm birth throughout childhood.5 74 The first, conducted by a US Institute of Medicine committee, synthesised within a decision-analytical model evidence gathered from several sources, including a number of health maintenance organisations in the USA.5 It estimated the annual societal economic burden associated with preterm birth in the USA to be at least $26.2 billion, or $51 600 per infant born preterm (over and above the costs associated with an infant born full term) (2005 prices).5 The committee reported that the majority of the costs were related to medical care ($33 200 per preterm infant), particularly those related to the initial hospitalisation with more than 85% of those services provided during the first year of life. Additional health-sector costs included those related to maternal delivery ($3800 per preterm infant) and early intervention services ($1200 per preterm infant). Special education costs associated with cerebral palsy, mental retardation, vision impairment and hearing loss were estimated to have an annual cost of $2200 per preterm infant. Finally, lost household and labour market productivity associated with those disabilities was estimated to be $11 200 per preterm infant. The study noted the concentration of medical care costs among extremely preterm infants, which account for 6% of all preterm births but account for more than a third of total preterm medical costs until age 7.5 However, the majority of the total societal costs are associated with those preterm infants born after 28 weeks' gestation since they account for the vast majority of preterm births. The authors also note the high degree of variation and skew underlying several of the cost estimates, even within gestational age categories. They attribute much of this variance to the higher average costs accruing to a small percentage of preterm children with severe disabling conditions. There are several limitations to this study, which the authors themselves acknowledge. Notably, the authors had limited data available on the costs associated with disability, such as the cost to caregivers. Furthermore, the authors do not refer to any sensitivity analysis, which would provide an indication of the uncertainty surrounding their cost estimates.
More recently, Mangham et al developed a decision analytical model to assess the economic consequences of preterm birth.74 The costs were considered from a public sector perspective and calculated throughout childhood. Consequently, the study adopted a more limited perspective and time horizon than the study by the US Institute of Medicine committee, which had adopted a societal perspective and considered costs accruing into adulthood.5 The authors constructed a Markov model for a hypothetical cohort of children, the size of which was set at 669 601 to reflect the number of live births in England and Wales in 2006. Model parameter inputs were largely drawn from three cohort studies: (i) the EPICure cohort of infants born in the UK and Ireland between March and December 1995 at less than 26 weeks' gestation; (ii) the 1991–1992 cohort of the Victorian Infant Collaborative Study Group (VICSG) of infants born in the Victoria state of Australia at 26 or 27 weeks' gestation; and (iii) the Oxford Record Linkage Study for infants born in Oxfordshire or Berkshire between 1990 and 1993 at 28 weeks' gestation or later.74 The authors estimated that the total cost of preterm birth to the public sector in England and Wales was £2.946 billion (95% CI £2.073bn to £4.048bn) over the 18-year time horizon of the model, expressed at 2006 prices and having applied a 3.5% annual discount rate. Of this amount, £989 million (95% CI £512m to £1.620bn) corresponded to those born VPT and £242 million (95%CI: £89m to £465m) to those born extremely preterm. The incremental cost per preterm child surviving to 18 years compared with a term survivor was estimated at £22 855. The corresponding estimates for a very and extremely preterm child were substantially higher at £61 781 and £94 740, respectively. These cost estimates were broadly in line with those generated by the US Institute of Medicine committee, despite the differences in modelling approach, perspective, time horizon and model parameter inputs.
Discussion
This paper has reviewed the recent published evidence on the economic consequences of preterm birth for the health services, for other sectors of the economy, for families and carers and, more broadly, for society. In addition to health service costs incurred during the initial hospital stay, the paper has revealed that preterm birth can result in substantial costs to the health services throughout childhood and can also impose a substantial economic burden on special education and other services and on the families and carers of the infants.
In addition to the costs highlighted by the review, preterm birth can have consequences that require further evaluation from an economic perspective. Institutionalisation costs for individuals with physical disabilities and learning difficulties throughout childhood and into adulthood have not been widely reported despite continued institutionalisation practices in many industrialised nations. The use of day care services and respite care has similarly been largely overlooked by economic studies of preterm birth. Other costs that have been largely overlooked include costs borne by local authorities and voluntary organisations, such as adaptations that have to be made to the individual's home as a result of their impaired state of health, and additional costs borne by families as a result of modifications to their everyday activities. In addition to the costs of travel, child care and accommodation, other potential costs faced by families and informal carers include incremental expenditures on health goods, such as alternative therapies, and non-health goods, such as nutritional requirements, laundry, clothing, heating utilities and repairs to the home. Furthermore, no monetary valuation of the intangible consequences of preterm birth, such as the pain, fear, suffering and emotional and social isolation experienced by the individuals themselves and their carers, has been attempted. The relative paucity of estimates of the long-term costs of preterm birth, particularly in adulthood, can largely be explained by a lack of routinely collected epidemiological data in this area. However, as the survival profile for preterm infants improves and further information on developmental outcomes during adolescence and adulthood becomes available, opportunities for economic research should increase.
How might the data identified in this review article be used? At one level, the cost estimates can be used to inform the planning of services and can provide a basis for assessing competing strategies for research and prevention. However, it should be noted that cost data alone cannot identify the most efficient allocation of finite healthcare resources. Rather, it is information on incremental costs and incremental health gains attributable to particular healthcare interventions that can identify the combination of human and material inputs that maximise health benefits or other measures of social welfare. This can be achieved through the general framework of economic evaluation.77 A number of interventions are effective at ameliorating the morbidity and mortality associated with preterm birth. In contrast, relatively few interventions have proved effective at preventing or delaying preterm birth. In order for finite resources in this area to be allocated in an efficient manner, it is imperative that economic evaluations of prevention and treatment interventions are carried out. The data identified by this review should be of interest and use to researchers planning to evaluate new or existing interventions from an economic perspective, particularly those wishing to incorporate within a decision-analytical framework the long-term economic impact of preterm birth and the cost-effectiveness of prevention and treatment strategies. Recent economic research has suggested that potential cost savings attributable to interventions currently of interest to clinicians, such as giving vaginal progesterone to women during pregnancy, are likely to be small and have to be counterbalanced against effects on longer-term childhood outcomes.78
It should be noted that analysts inputting data from individual studies included in this review into decision-analytical models may face a particular methodological challenge when the time horizon for the models span both childhood and adulthood. In this situation, it is plausible, and indeed likely, that the individual studies will reveal values that differ significantly by age. These differences may by explained, in part, by the geographical diversity of studies, which might reflect variations in healthcare practices and organisational models and variations in costing models applied across studies. However, they may also be explained by the direct impact of age on resource utilisation and costs. Ideally, the impact of age on costs should be estimated from data gathered in large-scale longitudinal studies as they become available. When such data are not available, however, techniques such as meta-regression of data across a number of studies should be considered as a means of disentangling age impacts.
In conclusion, this paper has provided an overview of the recent scientific literature on the economic consequences of preterm birth. Further studies of the economic consequences of moderate preterm birth and of costs of preterm birth that accrue in adulthood are particularly merited.
Acknowledgments
The authors would like to thank their colleagues at the University of Oxford for their helpful comments on the paper.
References
Footnotes
-
Funding SP is supported by a UK Medical Research Council Senior Non-Clinical Research Fellowship. The National Perinatal Epidemiology Unit, University of Oxford, is funded by the Department of Health in England. The Health Economics Research Centre, University of Oxford, is funded by the National Co-ordinating Centre for Research Capacity Development, England. The views contained in this paper are held by the authors and not necessarily the funding bodies.
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed.