Article Text

Abstract
Objective To describe simple estimates of likely duration of stay for very premature babies born in the UK and discharged home.
Design Statistical modelling of data from thirty neonatal units in a geographically defined region of the UK.
Participants All babies born at 23 to 32 completed weeks of gestation in 2005, 2006 and 2007 who were discharged home with the expectation that they would survive.
Main outcome measure Total duration of stay in the neonatal service.
Results 5528 babies were initially identified. 558 (10.1%) who died or who did not follow a normal care pathway were excluded. In a further 27, data were either missing or inadequate, leaving a study population of 4702 babies. As expected, gestation and birthweight exhibited strong influence on length of stay. Of the other variables tested, initial reason for admission (need for early respiratory support) showed the most consistent association. These factors were combined to produce predictive tables. The predictive performance of the tables was found to fit the data well for various groups, with the exception of multiple births who tended to have longer stays. However, when tested against individual units, much greater variation was seen independent of unit size and case mix.
Conclusion The prediction tables should permit parents to make sensible estimates about the duration of their baby's stay in the neonatal service; however, there appear to be important differences between units. The variation noted in length of stay between otherwise similar units merits further investigation.
Statistics from Altmetric.com
For parents who have a very premature baby, there is often little warning and little time to prepare. Where admission to a neonatal unit follows the birth, their initial concerns typically focus on the chances of the baby's survival and the risk of long-term neurodevelopmental problems. However, once beyond the early stabilisation phase, they are often keen to know how long their baby is likely to need to remain in hospital.
In the UK, this issue has received relatively little attention, perhaps because of the historic approach to funding, but in those countries, such as the USA, where costs of hospital care have routinely been linked to length of stay, there has been a greater focus on this topic.1,–,5 Since the health economic data from these studies are very much linked to the local health system, it is not necessarily applicable to other populations. Despite the overt linkage of length of stay and hospital costs information, surveys of practice in relation to discharge criteria indicate that there is considerable variation even in the USA.6 7
What is already known on this topic
▶. Duration of stay for very preterm babies is related to their gestational age.
▶. Various interventions are able to reduce length of stay in settings around the world.
What this paper adds
▶. Precise estimates of length of stay of very preterm babies based on the babies' gestation and clinical condition.
▶. Evidence that unit of care at the time of discharge has major effects on the overall length of admission.
In the last few years, significant changes have occurred to the organisation and funding of healthcare in the UK and neonatal care, as a specialised service, in particular. The anticipated policy move to charging on a daily basis for such services has made length of stay in such high-cost, low-volume services of much greater interest to funders.
The study reported here had two specific aims:
▶. To provide a simple means by which parents of premature babies might estimate the likely duration of their babies stay in the neonatal service.
▶. To assess the extent to which variation in length of stay occurs between neonatal units.
Methods
Data for the study were collected as part of The Neonatal Survey (TNS). This is an ongoing study of neonatal intensive care activity in the East Midlands and Yorkshire regions of the UK. All of the perinatal services in this geographical area contribute to the TNS and units in adjacent regions also permit data collection on “displaced” infants. Data collection for a more limited area started in February 1990, but expansion to this larger population began in 2004. The database holds information relating to all infants of 32-week gestation or less born to a mother resident in the East Midlands or Yorkshire and admitted to a neonatal unit. Data for TNS are collected by a group of eight part-time research nurses who visit each of the 30 neonatal units on a regular basis and complete a standardised data set about each infant. Information is obtained from the clinical records, discussions with staff and, where appropriate, personal observation. For this study, all babies born to a mother resident in the TNS area during 2005, 2006 and 2007 were included if they were born at 23 to 32 completed weeks of gestation and were discharged home from a neonatal unit.
The work of TNS has been approved by the Trent Research Ethics Committee. In addition, approval to collect data without individual consent has been provided by PIAG/NIGB.
The babies were categorised into groups according to gestational age at birth (completed weeks) and birthweight (250-g categories), both factors known to influence length of stay.1 5 Gestational age was assigned using an algorithm described previously.8 To improve the precision of the tables, a further predictive factor was sought, which, when assigned into two categories, predicted length of stay across all the gestational ages included in the study population and which could be assigned early in neonatal care. The factors investigated were sex, multiplicity of pregnancy, reason for the first admission (categorised as either “respiratory” where respiratory support was needed in the first 12 h or alternatively as “prematurity” where other problems of prematurity were the cause of the admission), length of ventilation and duration of respiratory support (all types).
The 10th, 50th and 90th percentiles for length of stay were estimated using quantile regression adjusted for these characteristics.9 Quantile regression allows any specific percentile to be directly estimated from the data. In this paper, each percentile was estimated separately, allowing for the possibility that the functions for the different percentiles took different shapes. Gestational age in completed weeks and birthweight group were entered into the model as ordered categories together with all possible two- and three-way interactions. The shapes of the functions for gestational age, birthweight group and interactions were investigated using fractional polynomials up to degree 3 to allow the investigation of a wide variety of different shaped curves.10 Model selection was by change in deviance using a 5% significance level.
All modelling was carried out using STATA V.10.0 and SAS V.9.1 was used to generate the predictive tables.
The predictive performance of the model was investigated by calculating the proportion of babies falling below each estimated percentile for groups defined by factors included in the model and other important characteristics (sex, year of birth, CRIB II, Apgar at 1 and 5 min, multiplicity of pregnancy).
The proportion falling below each estimated percentile was also calculated for each of the neonatal units within the TNS area. Where babies were transferred, they were assigned to the unit from which they were discharged home.
Results
During the period 1 January 2005 to 31 December 2007, there were 5528 babies of the relevant gestation born to mothers from the TNS area who were admitted to a neonatal unit. Of these, 558 (10.1%) died before discharge and 241 (4.4%) were discharged to somewhere other than home or were discharged home under special circumstances (eg, terminal care). These babies were excluded from the subsequent modelling. Similarly, we excluded babies where length of stay or birthweight data were missing (19) or where we had reason to doubt the accuracy of the birthweight recorded (4) or where the nature of the admission did not appear to be related primarily to problems of prematurity (4). This left a study population of 4702 babies, of whom 1334 (28%) were transferred between units during their stay.
A range of descriptive variables were inspected to identify those that, when dichotomised, had the most consistent influence on length of stay above that of gestation and birthweight, which, unsurprisingly exhibited strong influence. The initial reason for admission (whether the baby needed respiratory support in the first 12 h or not) showed the most consistent association across all gestational ages. The distribution of infants in relation to the need for respiratory support in the first 12 h is shown in table 1. It is clear from this that very few babies under 28-week gestation required no respiratory support during this time.
Distribution of reason for first admission by gestational age at birth
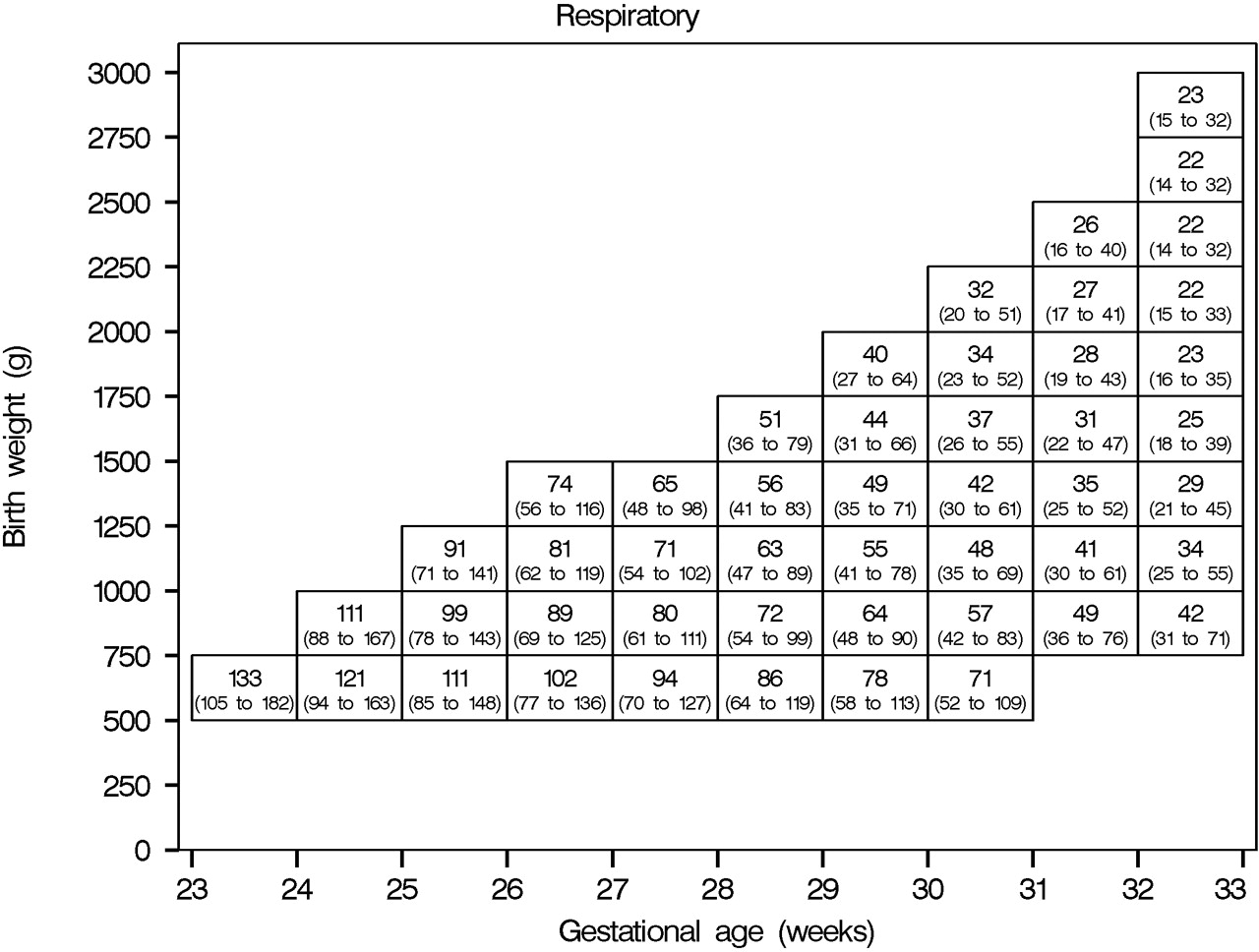
The data from these two groups were then combined with data regarding gestation, birthweight and length of stay to construct two predictive tables, that is, one for babies needing respiratory support in the first 12 h and one for babies needing no such support (figs 1 and 2). Each cell shows the estimated median (10th to 90th percentiles) length of stay. Cells in fig 2 representing babies <29-week gestation needing no respiratory support are shaded as data were sparse for these babies.
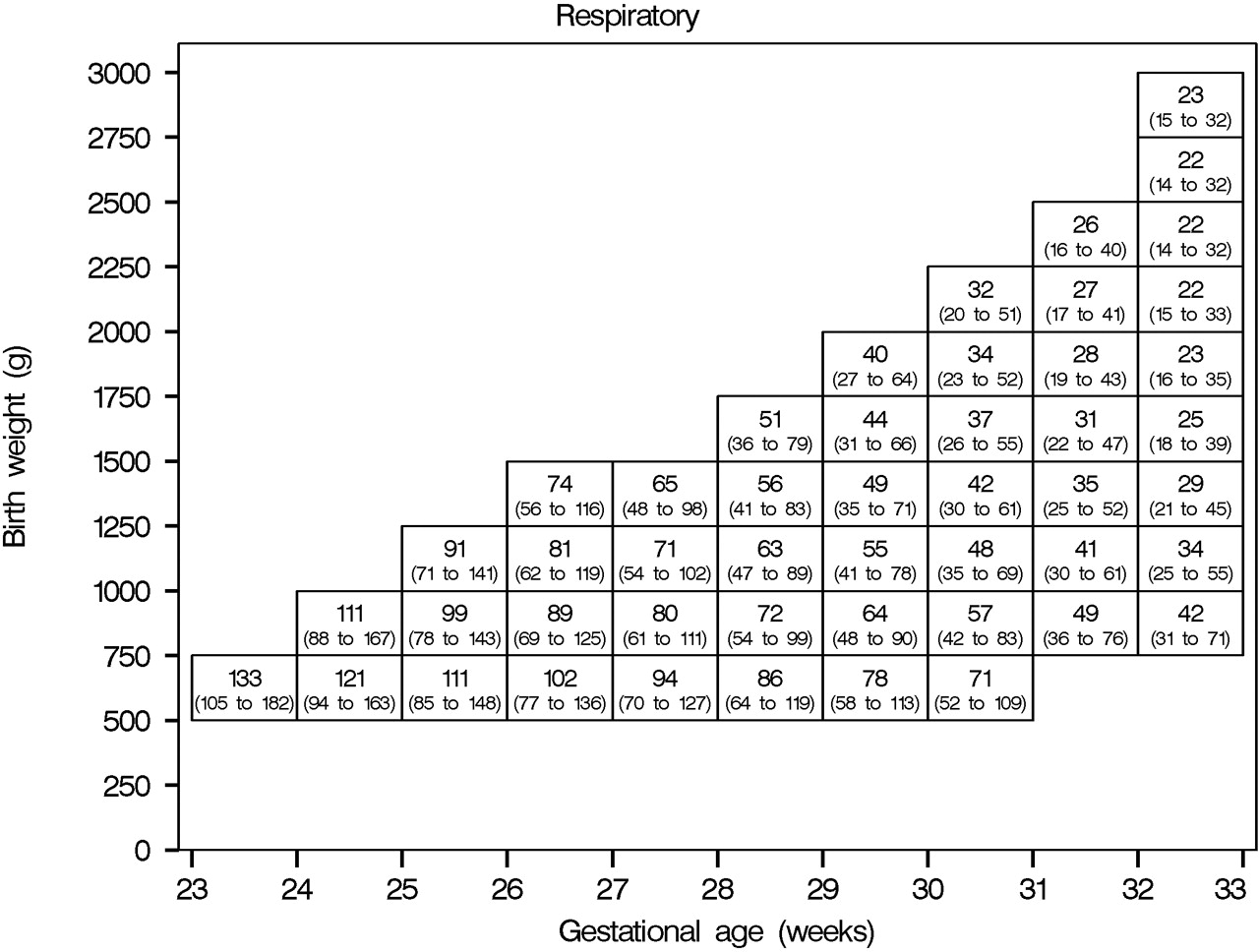
Median length of stay (10th to 90th percentile) in days of infants discharged home from neonatal care for babies needing respiratory support in the first 12 h.

Median length of stay (10th to 90th percentile) in days of infants discharged home from neonatal care for babies not needing respiratory support in the first 12 h.
The predictive performance of the tables was inspected for various groups (table 2). The model was found to fit the data well, with the exception of multiplicity of the pregnancy. Babies from multiple births tended to have longer stays than singleton babies, particularly for babies born >27-week of gestational age. There may also be some suggestion of increasing lengths of stay over time as the proportion below each estimated percentile fell slightly over the 3 years.
Predictive performance of the final model against various sub-divisions of the population.
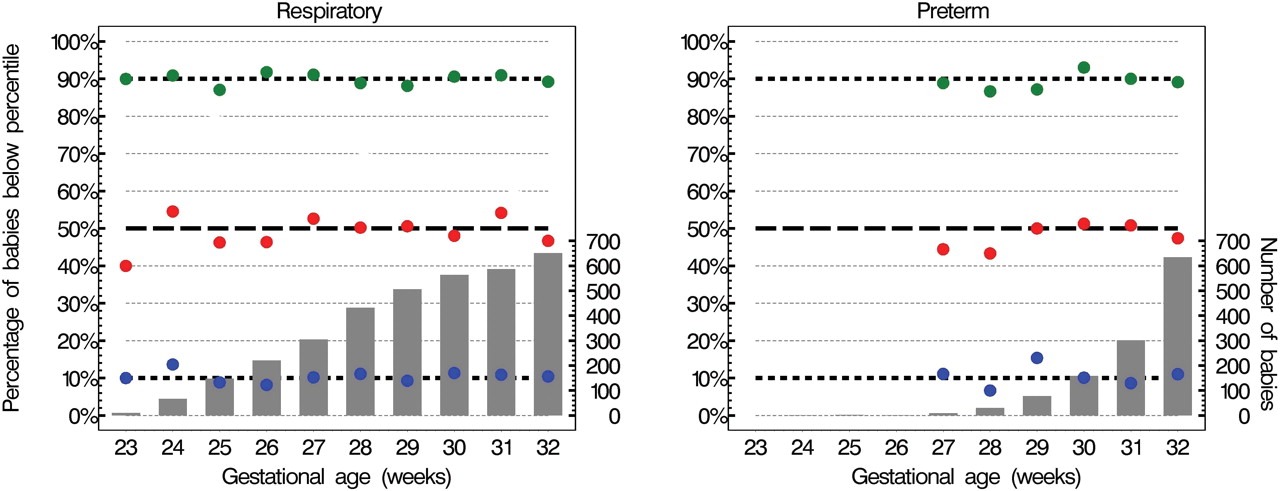
The tables predict well by gestational age, where there were sufficient numbers of babies (fig 3).
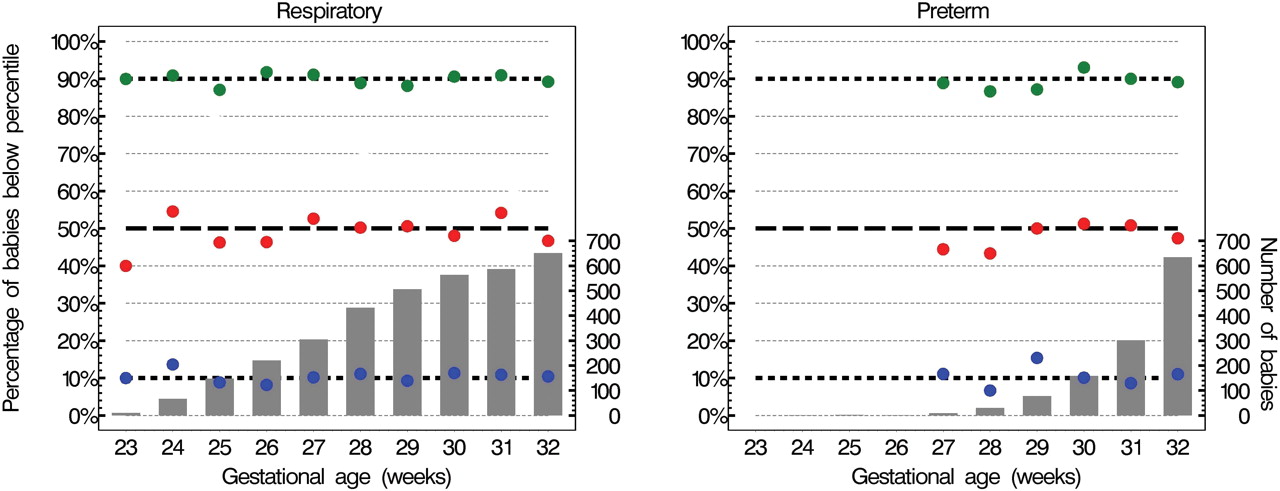
Percentage of babies falling below estimated percentiles (10th blue; 50th red; 90th green) and number of babies by gestation and need for respiratory support in the first 12 h.
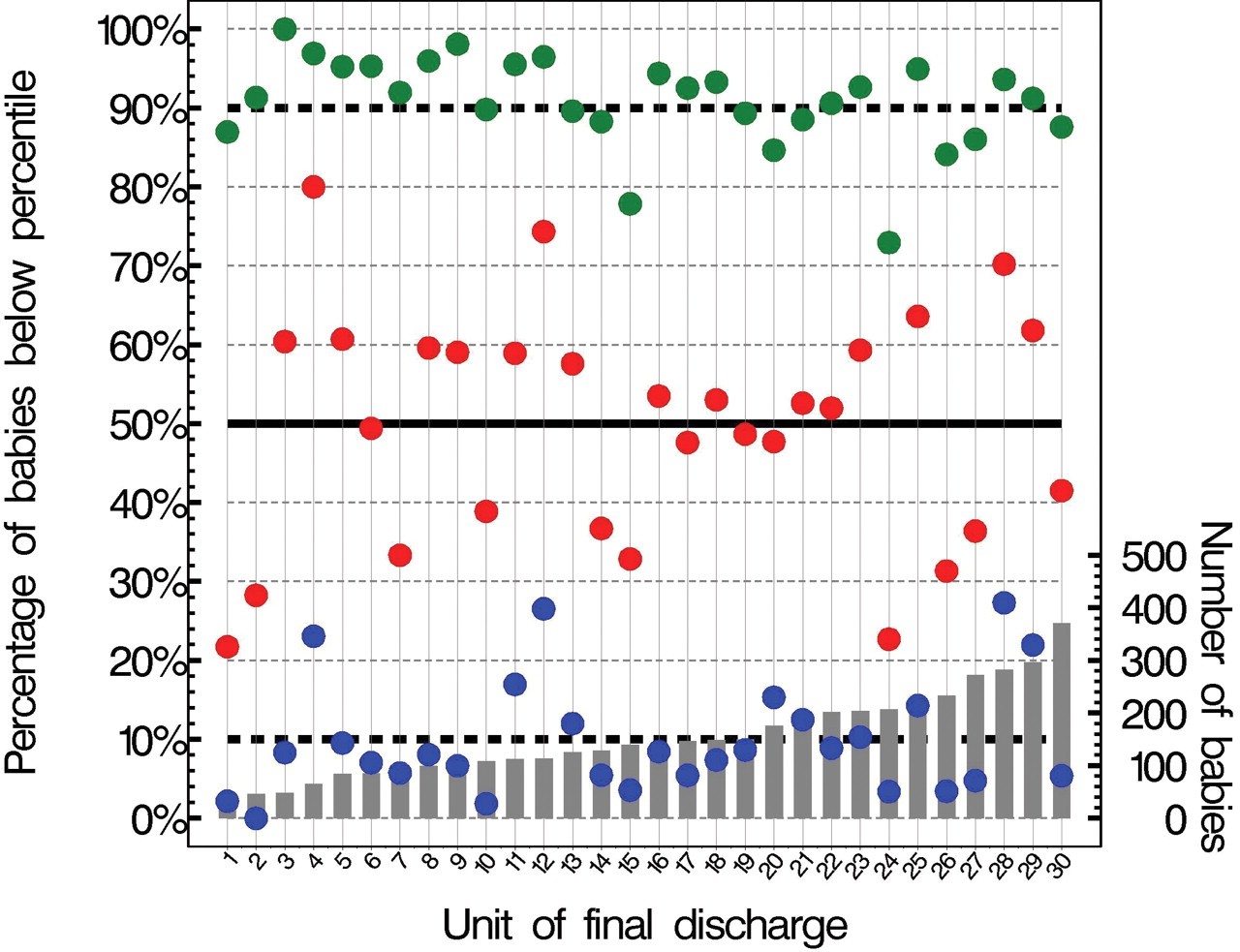
The prediction was much less good when tested against individual units (fig 4). There was evidence that the units varied in the proportion falling below each percentile (χ2 test: p<0.001 for each estimated percentile).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Percentage of babies falling below estimated percentiles (10th blue; 50th red; 90th green) and number of babies by unit of final discharge.
It seemed highly likely that the lack of predictive performance when assessing the tables against individual units was the result of local policies and services governing the timing of discharge home since, when assessed against measures affecting severity (such as a disease severity score), predictive ability appeared excellent, and as shown in the figure, there was no apparent association with size of unit. To assess the scale of this affect on overall length of stay we estimated that if all units had lengths of stay equivalent to the median length of stay for the group over 3 years the total number of cot days would fall by 12 426 days, or 5.5%. Similarly, if length of stay was reduced to a figure equivalent to the current 10th centile (ie, the group with the shortest stays), the effect would be a fall of 68 493 days, or 30%.
Discussion
One of the aims of this paper was to provide parents with a straightforward means of estimating length of stay, and we have done this using a simple tabular format, which we know, from previous experience of similar tables predicting death, parents generally find useful and understandable. In using such tables, it is important that parents understand that clinical factors are being used to provide an estimate based on what has happened to other babies.
The percentiles were estimated using quantile regression. Other methods could potentially have been used, including linear models and generalised linear modelling. This method was chosen because it is straightforward and makes fewer assumptions than other methods. Ultimately, whatever statistical method is used, what is required is that the estimated percentiles describe the data sufficiently well to be of use to others. In addition, fractional polynomials were used to describe functions, allowing them to take a wider range of shapes than is possible using conventional polynomial terms in the models.
Although the tables reported in this paper describe the observed data well, their predictive performance would need to be investigated in other populations before any conclusions could be drawn on their generalisability. Indeed, given the variation seen in the units included here, it is unlikely that the tables will describe precisely the length of stay on any particular unit but may be representative of other geographic-based cohorts. Nevertheless, since these tables are derived from all admissions from a large UK population (~110 000 births/year comprising over 15% of all births in England and Wales), we feel the data are likely to provide users with a useful estimate of length of stay. The number of clinical factors in the model is deliberately small in order to produce useful tables, and it is recognised that the addition of further variables into the model could explain some of the variation in lengths of stay. This, however, was not the primary focus of this paper and will be explored in later work.
In order to produce a model that reliably estimates of length of stay for this population, we have focused on clinical factors. However, it appears that length of stay can be strongly influenced by organisational factors as we observed significant variation between otherwise similar units. Clearly, this is not unexpected because a range of approaches are possible with regard to both inpatient care and, in particular, discharge policies. These variations have been well documented particularly in North America, where the economic costs of neonatal care are recognised as very significant.11 It would appear from our data that there is potential for reducing inpatients stays in a proportion of the units included with likely health economic benefits. It seems equally likely that such variation in length of stay will be apparent in other countries, and we speculate that this will be particularly evident in those where costs to either the family or insurer are not adjusted by reference to a “standard” length of stay for a baby of similar gestation, that is, there is no financial incentive to the provider unit for early discharge. However, from a parental point of view, there are clearly other advantages from having their baby home earlier, provided it is safe to do so.12
For this cohort, we have not collected prospective information about discharge policy from the 30 units contributing data. Important factors that might influence length of stay include whether the unit has a specified weight criteria before discharge can occur, the presence and extent of a community support team,13 whether babies are allowed home tube feeding, criteria for discharge home on oxygen and local policies regarding discharge planning and preparation. Certainly in the UK, these aspects of the service have received far less attention than the intensive care elements of looking after preterm babies. While proper preparation and timely discharge have been seen as good practice from a family care perspective, the health economic implications for the service have not been explored extensively. Certainly, data from the USA would suggest that it is possible to produce significant change by targetting different aspects of discharge practice.3 4
The data presented here will give an opportunity for those who provide neonatal services to assess their performance in terms of length of stay. It seem highly likely that for a proportion careful investment in measures to facilitate early discharge will produce significant savings in terms of in patient stays as well as freeing up capacity within the service.
Acknowledgments
The authors wish to acknowledge the continuing help and collaboration of the hospitals delivering perinatal care in both Trent and adjacent regions. This study is one of the Trent Infant Mortality and Morbidity Studies, which are funded by the PCTs of the East Midlands of England and Yorkshire.
References
Footnotes
-
Funding Multiple NHS funders (PCTs) in East Midlands and Yorkshire; NHS Specialist Commissioners/PCTs.
-
Competing interests None. The funders were independent of the research team. The sponsors were University Hospitals of Leicester NHS Trust, whose role was purely in relation to research governance.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Ethics approval This study was conducted with the approval of the Trent MREC.