Article Text

Abstract
The normal range of heart rate (HR) in the first minutes after birth has not been defined.
Objective To describe the HR changes of healthy newborn infants in the delivery room (DR) detected by pulse oximetry.
Study Design All inborn infants were eligible and included if a member of the research team attended the birth. Infants were excluded if they received any form of medical intervention in the DR including supplemental oxygen, or respiratory support.
HR was measured using a pulse oximeter (PO) with the sensor applied to the right hand or wrist immediately after birth. PO data (oxygen saturation, HR and signal quality) were downloaded every 2 sec and analysed only when the signal had no alarm messages (low IQ signal, low perfusion, sensor off, ambient light).
Results Data from 468 infants with 61 650 data points were included. Infants had a mean (range) gestational age of 38 (25–42) weeks and birth weight 2970 (625–5135) g. At 1 min the median (IQR) HR was 96 (65–127) beats per min (bpm) rising at 2 min and 5 min to 139 (110–166) bpm and 163 (146–175) bpm respectively. In preterm infants, the HR rose more slowly than term infants.
Conclusions The median HR was <100 bpm at 1 min after birth. After 2 min it was uncommon to have a HR <100 bpm. In preterm infants and those born by caesarean section the HR rose more slowly than term vaginal births.
Statistics from Altmetric.com
Background
Heart rate (HR) is the most important, objective clinical indicator of the health of newly born infants.1 Increasing HR is considered to be a good marker of effective resuscitation, and a HR exceeding 100 beats per min (bpm) is considered normal.2
Immediately after birth HR is usually counted by auscultation or palpation of the umbilical cord. Both of these are imprecise and systematically underestimate the true HR.3 HR can also be measured by pulse oximeter (PO) or ECG. ECG is difficult to apply and not readily available in the delivery room (DR). However, PO is increasingly used during neonatal resuscitation.4 5 PO pulse rate is equivalent to HR except in cases of cardiac arrhythmia6 which are rare at birth. PO accurately measures HR in newly born infants even when the HR is low provided there is a good plethysmographic signal7 and there are no indicators of poor signal.6
There are several reports of oxygen saturation (SpO2) measurements recorded in the DR with a PO.8,–,16 However, there are few data on HR in the first minutes of life.
What is already known on this topic
Heart rate is the most important, objective clinical indicator of health in newly born infants.
The clinical methods for counting heart rate, auscultation or palpation of the umbilical cord are both imprecise and systematically underestimate the true heart rate.
Pulse oximetry accurately measures heart rate in newly born infants even when it is low provided there is a good plethysmographic signal.
What this study adds
Some healthy infants will have a heart rate less than 100 bpm in the first 2 min after birth.
Heart rate <100 bpm, in the first 2 min when breathing and tone are normal, and should not be an indicator for immediate ventilation.
We aimed to describe the HR changes in the first 10 min after birth of infants who did not receive any postnatal medical interventions. We sought to determine whether there were HR differences in subgroups according to gestational age, mode of delivery or maternal anaesthesia.
Patients and Methods
Three datasets were combined to form the dataset for analysis. These were: Kamlin,13 Dawson (unpublished) and Vento (unpublished). Infants who did not receive any medical interventions, supplemental oxygen or assisted ventilation immediately after birth were eligible for inclusion. Infants were excluded if they received any of the above interventions. Verbal parental consent for the study was obtained before delivery. The investigating team was not involved in the care of the infants in the DR. All resuscitation measures (eg, intubation, external cardiac massage, administration of oxygen and other drugs) were at the discretion of the clinical staff involved, following the Royal Women's Hospital protocols, which are based on the Australian Resuscitation Council guidelines.17 Vento's data were collected in 2005–2007, before the guidelines of the Committee for Resuscitation of the Spanish Neonatal Society recommended that babies ≤ 28 weeks gestation should receive initial treatment with continuous positive airway pressure.18 Before birth, parents gave verbal consent for their infant/s to participate. The study was endorsed by the relevant research and ethics committees at each hospital.
Immediately after birth a pulse oximetry sensor (LNOP Neo Masimo SET, California, USA) was placed on the infant's right hand or wrist and then connected to an oximeter (Radical 7, Masimo, California, USA).19 SpO2, HR and signal quality were stored by the oximeter, every 2 s. We used 2-s averaging and maximum sensitivity as this combination allows rapid detection of changes in SpO2 and HR during periods of low perfusion4 that may occur during the first minutes after birth.
After birth, data from the oximeter (time, HR, SpO2 and signal quality) were downloaded to a computer using the neO2M program20 (Girvan Malcolm, Royal Prince Alfred Hospital, Sydney, Australia). Using a customised Excel (Microsoft) macro we combined the PO data with the time of first data to enable time appropriate analysis by Stata (Intercooled 10.0, Statacorp Texas, USA). We only analysed HR measurements when the oximeter signal was normal, that is, no alarm messages (low IQ signal, low perfusion, sensor off, ambient light).
Demographic data are presented as numbers and proportions (%) for categorical variables, or means with SD for normally distributed continuous variables and median (interquartile range) when the distribution was skewed. A two-tailed Mann–Whitney U test was used to compare subgroups.
HR during the first 10 min is illustrated using centiles calculated using the ‘LMS’ method of Cole and Green,21 fitted using LMSChartmaker software.22 Fifty-five per cent of the babies were sampled consistently on even seconds, and the remainder consistently on odd seconds. To synchronise the two sets of HR traces, prior to analysis 1 s was added to each odd second. Centiles for HR were then fitted in the usual way (equivalent degrees of freedom for skewness (L) = 3, median (M) = 9 and, coefficient of variation (S) = 5 and, and transformed age power = 0.2).22 Centile graphs were plotted using Stata software.
Results
At the Royal Women's Hospital we attended 775 births; 345 infants were excluded. Infants were excluded for the following reasons: 27 infants had congenital anomalies; 11 infants received free flow oxygen; 290 received respiratory support including CPAP and/or IPPV; and we were unable to obtain or download data from 17 infants. Hospital La Fe contributed data from 29 infants. The final dataset comprised 61 650 HR measurements from 468 infants who did not receive any interventions other than warmth and stimulation. The median (range) gestation of the 306 term infants (≥37 weeks) and the 160 preterm infants (<37 weeks) was 40 (37–42) and 33 (25–36) weeks respectively. There were 22 infants <30 weeks gestation, three from the Dawson dataset and 19 from the Vento dataset. The characteristics of the infants are presented in table 1.
Infant characteristics
There were 181, 316, 342, 332, 336, 289, 274, 251, 243 and 230 individual infant HR observations at each minute from 1 to 10 min. The rise in HR of all infants, preterm and term infants is shown in figures 1, 2 and 3 respectively. At 1 min after birth the median HR (IQR) was 96 (65–127) bpm rising to 123 (91–153) at 1.5 min and 139 (110–166) bpm and 163 (146–178) bpm at 2 and 5 min respectively (table 2). In preterm infants the HR rose more slowly than term infants (table 2). HR also rose more slowly in infants born via caesarean section (table 3) and in those born to mothers who received anaesthetics (regional epidural/spinal or general) or narcotics during labour (data not shown).
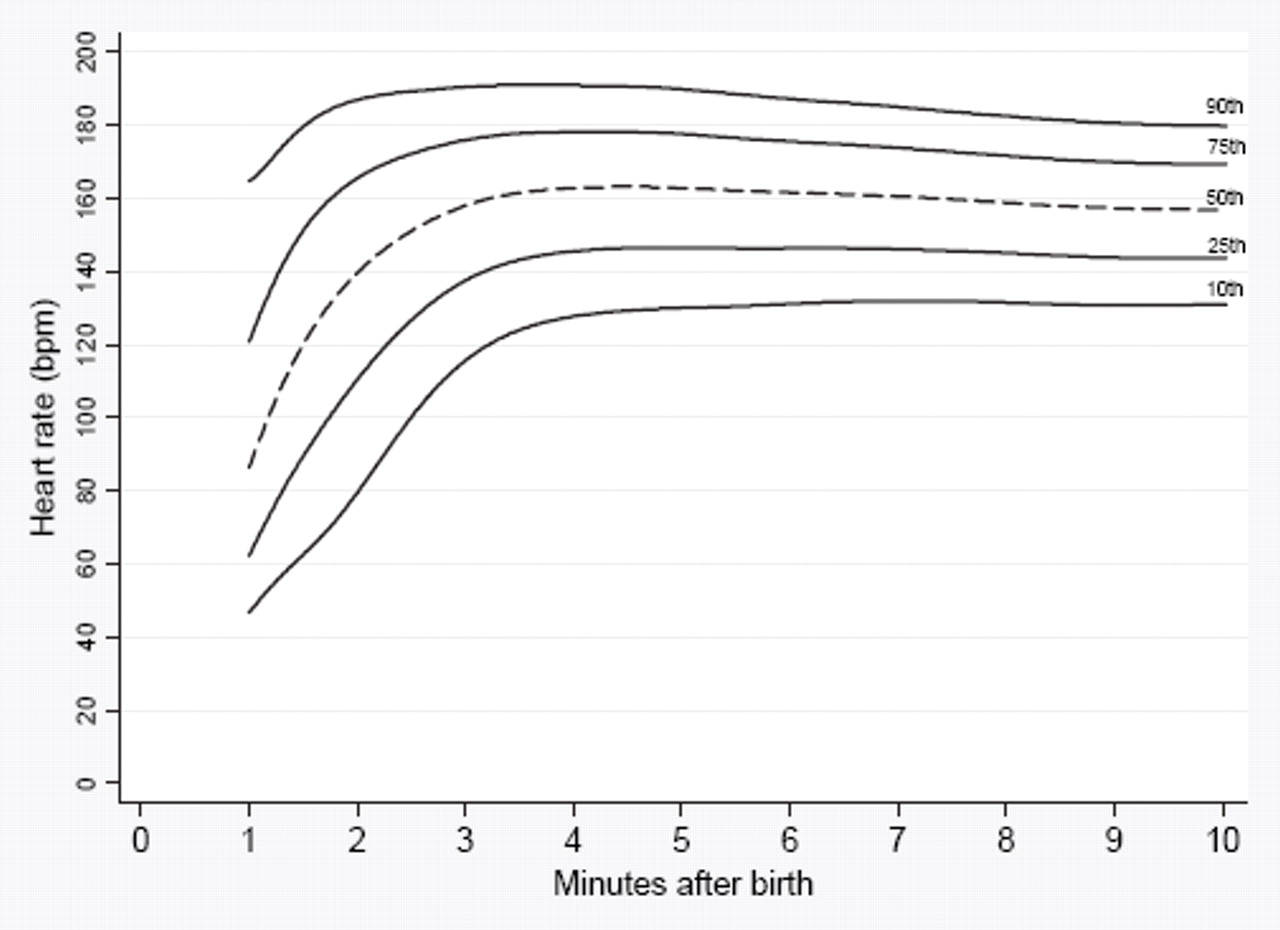
The 10th, 25th, 50th, 75th and 90th heart rate centiles for all infants with no medical intervention after birth. bpm, beats per minute.

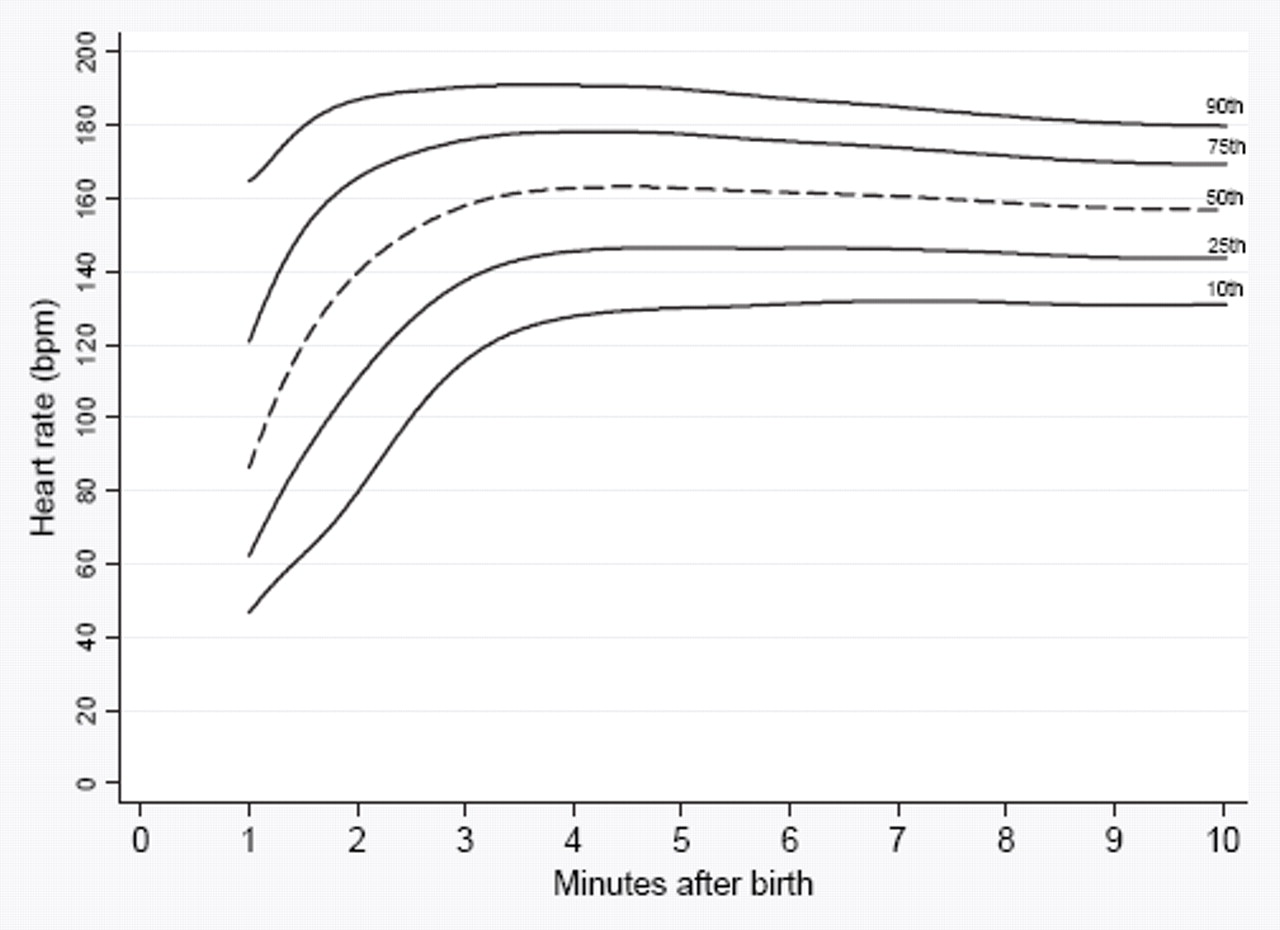
The 10th, 25th, 50th, 75th and 90th heart rate centiles for infants <37 weeks gestation with no medical intervention after birth. bpm, beats per minute.

{kind=link}
{kind=link}
{kind=link}
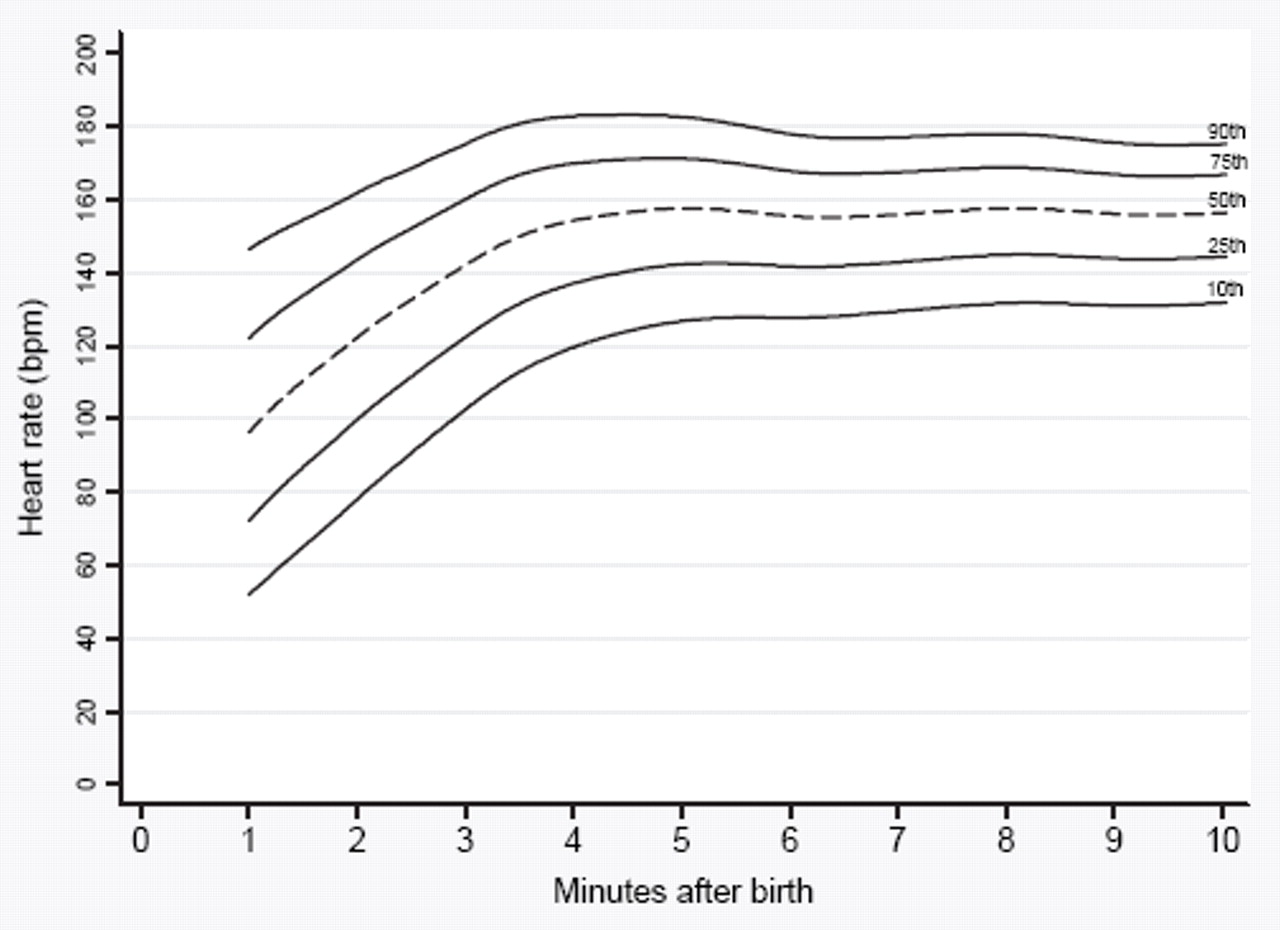
The 10th, 25th, 50th, 75th and 90th heart rate centiles for term infants with no medical intervention after birth. bpm, beats per minute.
Comparison of heart rate (bpm) measurements from 1 to 10 min after birth in preterm (<37 weeks) versus term births.
Comparison of heart rate (bpm) measurements from 1 to 10 min after birth in caesarean versus vaginal births
At 1 min 17% (n=30) of the infants had a HR <60 bpm and at 2 min there were 7% (n=20) with a HR <60 bpm. Of the 30 infants with a HR <60 bpm at 1 min 66% (n=20) were <37 weeks gestation. After 2 min only a very small percentage of infants had a HR <100 bpm (table 4).
Percentage (number) of infants with HR< 60 bpm or HR <100 bpm in the first 10 min after birth
There is a small difference in the values in table 4 and the centile charts (figures 1 to 3). This is because the table includes data collected exactly at each minute whereas the centile chart includes smoothed data from all time points. During the first 90 s we observed that for some infant, although the signal quality was satisfactory the HR fluctuated rapidly. These measurements were usually adjacent to data with an unsatisfactory signal. We have included oximetry data where no error message was seen.
Discussion
This is the first study to report detailed changes in HR in the first minutes after birth of human infants who did not receive any medical interventions. In 1953 Virginia Apgar stated “heart rate was found to be the most important diagnostic and prognostic of the five signs” that now form the basis of the Apgar score.1 Information on the normal range of HR in the minutes immediately after birth and how it changes with time could be useful for those caring for the infants in the DR.
In our cohort of infants not receiving resuscitation interventions in the DR, we found the median HR was <100 bpm at 1 min. The low HR in the first minutes in some infants is interesting because the standard teaching is that infants with a HR <100 bpm after birth should receive positive-pressure ventilation.23 However, our study shows that a HR <100 bpm occurs in some infants who were judged not to require oxygen or ventilation after birth. At 1 min, half of these infants had a HR <100 bpm and 17% had a HR <60 bpm. By 2 min only 14% had a HR <100 bpm.
A HR of <100 bpm after birth is usually considered to be due to hypoxia and acidosis.24 However, in 1962 Brady25 reported HR changes in the fetus, and newborn infant during labour, delivery and the immediate newborn period using ECG and reviewed the literature at that time. She commented,
A prompt fall in rate was consistently seen when the cord was clamped before the onset of respiration, while no such change was seen in vigorous infants who began breathing before cord occlusion. A fall in rate was also seen in mildly depressed infants who cried only occasionally and were not breathing when the cord was clamped. The rapidity of change suggests that the mechanism is reflex in nature.
Barcroft26 studied goats and concluded that there were two mechanisms responsible for the bradycardia, one reflex due to vagal stimulation and the other a direct effect of asphyxia on cardiac muscle. Bradycardia after birth was considered to be due to vagal stimuli especially if the cord was cut before the infant had taken a breath. Intrauterine hypoxia and acidosis may be the cause of bradycardia at birth in some infants. However, in our study none of the infants were asphyxiated on the basis of assessment by the clinicians present or the median (IQR) Apgar scores at 1 min 8 (8–9). It is likely that their early ‘bradycardia’ is due to vagal stimulation.
A proposed cause for reflex bradycardia is a reduction in venous return to the heart. During fetal life, the placental circulation acts as a low resistance shunt receiving approximately half the combined ventricular output.27 Following clamping of the cord, venous return to the right side of the heart transiently decreases, due to the sudden absence of blood flow returning from the placental circulation via the liver and ductus venosus.28 Furthermore, if the cord is cut before the lung has aerated and pulmonary blood flow has increased,29 30 venous return to the left side of the heart will also be low. The resulting reduction in venous return to both sides of the heart causes a reflex decrease in ventricular output, resulting in a reduction in HR. In our studies we did not record HR in relation to cord occlusion and the onset of breathing, and so cannot comment on whether a reduction in venous return may be a contributing factor to the early bradycardia seen immediately after birth.
The studies of Dawes using an animal model of acute neonatal asphyxia are landmarks in the field.31 The ‘bradycardia’ he observed is often assumed to be due to hypoxia and acidosis. However his graph of HR31 shows the fall in HR after cord occlusion occurred very rapidly. This is most likely to be due to a vagal reflex that is rapid in onset and has been well described in other physiological studies.32
Our results on the effect of delivery confirm the findings of Gonzales and Salirrosas10 who reported that infants born via caesarean had a significantly lower HR than vaginal births at 1–5 min of life. They measured HR from the left foot immediately after birth with a PO in infants >28 weeks gestation. The mean (SD) HR at 1 and 10 min after vaginal delivery were 133 (36) and 150 (22), and from 1 and 10 min after caesarean section the HR was 108 (36) and 148 (26) bpm. Infants born by vaginal delivery had a significantly higher HR than those born by caesarean from 1 to 5 min after birth (p<0.02 to p<0.05).10 Toth33 measured HR in 50 infants born at term not requiring interventions in the DR. He did not report HR at 1 min; after 2 min the median (range) HR was 157 (89–199) bpm decreasing after 10 min to 148 (110–191) bpm. In the 16 infants whose mothers received epidural anaesthesia there was a significant increase in HR. In Toth's sub group receiving epidural anaesthesia the median HR was 166 bpm versus 153 bpm in the group without analgesia (p<0.05).33 In contrast our infants born to mothers receiving anaesthesia (regional or general) had a similar median HR in the first 1 to 10 min to those with no anaesthesia.
We found infants born preterm, but not receiving resuscitation, had a lower HR in the first 10 min of life than term infants. Kopotic14 measured HR by PO in 15 infants <30 weeks gestation who were actively resuscitated. He reported it took a median (range) of 2.8 (2.2–5.5) min to reach a HR ≥100 bpm, in these infants. In our study 22 infants <30 weeks gestation not receiving resuscitation in the DR took a median (range) 1.9 (1–2.9) min to reach a HR ≥100 bpm.
A measure of HR by auscultation or palpation every 30 s during neonatal resuscitation interventions is less informative than a continuous display of measurements, taken every 2 s. For example, a HR of 58 bpm that is rising rapidly probably does not need intervention. However, a HR of 58 bpm that is not rising needs urgent treatment.
One novel finding of our study was the unexpectedly high proportion of infants with a HR <100 bpm in the first minutes after birth. Therefore it is important to consider the accuracy of PO in measuring low HRs immediately after birth. Evidence indicating that the low HR values are accurate comes from a number of sources. Bradycardia occurs normally after birth in some infants in the first 2 min of life.25 Kamlin7 found that the same PO, used in our study, produced readings that correlated well with simultaneous ECG measurements even when the HR was <100 bpm. The sensitivity and specificity of PO for detecting a HR <100 bpm compared to HR measured by ECG were 89% and 99%, respectively.
In the present study, HR data were only used if there were no alarm message on the PO and therefore the possibility that the data includes artefact is low. Also the low HR values were part of a changing sequence, not randomly variable as they might be if they were artefact, and all rose with time. There are no reasons to consider that the low HRs were abnormal and the high rates, measured with the same machine a short time later were accurate.
The Neonatal Resuscitation Textbook23 suggests that if the HR is <100 bpm during the first minute of life, positive pressure ventilation should be provided. However Milner and Greenough34 point out that there are no human or animal data to support this recommendation. The data from our study suggests that many healthy infants have a HR <100 bpm at 1 min of age and 21% at 2 min. It should be noted that a HR <60 bpm was measured in these infants with good muscle tone and normal respiratory effort at 1 min and 2 min, in 17% and 7% respectively. Therefore low HRs in the first 2 min may be considered ‘normal’ and in isolation from other signs, should not be an indication for immediate ventilation. One of the benefits of PO is that the change of HR with time can be part of the rapidly dynamic assessment of an infant immediately after birth.
We speculate that although the graphs are constructed using only ‘good signal’ data points the PO measurements may be erratic particularly in the first 60–90 s when HR is changing rapidly without displaying a ‘poor signal’. In some of our recordings we noticed highly variable HRs in the first 2 mins. We used 2-s averaging to measure HR. These HR measurements might have been more stable if we had used a longer averaging time.6 It is important to realise that the PO HR is only a tool to assist the resuscitators and they should verify the data clinically if they doubt its validity.
What should clinicians do if the PO indicates that an infant has a HR <100 bpm in the first 2 min of life? We believe that if the infant is breathing and has good tone then the HR can be carefully watched without intervention. However, if the infant is apnoeic or flaccid then the bradycardia should be considered an indication of possible asphyxia and the infant given respiratory support.
By 3 min it was very uncommon for the HR to be below 100 bpm suggesting that the cut off of 100 bpm for abnormal HR is appropriate at this time. The HR changes after birth were quite similar in preterm and term infants and those born vaginally or by caesarean section delivery.
In summary, half of those infants who did not receive any medical intervention immediately after birth had a HR less than 100 bpm in the first minute of life and about a tenth by 3 min. This suggests that a low HR alone does not always require assisted ventilation.
Acknowledgments
We thank Dr Girvan Malcolm, Royal Prince Alfred Hospital Sydney, Australia for assistance with his NeO2M program. We thank Marta Aguar MD and María Brugada MD, research fellows of the Hospital La Fe Research Foundation Fellow Program Valencia, Spain for their assistance in recruiting babies in the DR and collecting data.
References
Footnotes
-
Funding JAD, COFK and ATB are past recipients of a RWH Postgraduate Scholarship. ATP is recipient of a Ter Meulen Fund grant for working visits, Royal Netherlands Academy of Arts and Sciences, The Netherlands. PGD is a recipient of an NHMRC Practitioner Fellowship. PGD, SBH and CJM hold an Australian National Health and Medical Research Council Program Grant No. 384100. TJC received funding from the UKMRC.
-
Competing interests None.
-
Ethics approval This study was conducted with the approval of the Study endorsed by The Royal Women's Hospital Research Committee.
Detail has been removed from these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
-
Provenance and peer review Not commissioned; externally peer reviewed.