Article Text

Abstract
Background: Because ethical decision making in the care of extremely preterm infants varies widely across Europe, the Swiss Society of Neonatology decided to publish its own guidelines on the care of infants born at the limit of viability in 2002.
Objective: To examine the potential impact of the guidelines on survival rates, short-term complication rates and centre-to-centre outcome differences of extremely preterm infants (22–25 completed weeks).
Design: Population-based, retrospective cohort study.
Setting: All nine level III neonatal intensive care units (NICU) and affiliated paediatric hospitals in Switzerland.
Patients: 516 extremely preterm infants born alive between 1 January 2000 and 31 December 2004.
Main outcome measures: Delivery room and NICU mortality rates, survival to hospital discharge and incidence of short-term complications in survivors were assessed. To study the impact of the guidelines, two cohorts from two different time periods were compared (years 2000/2001, n = 220; years 2003/2004, n = 204) whereas patients born in the year of the publication (2002, n = 92) were excluded. For centre-to-centre comparisons, the entire population (n = 516) was analysed.
Results: There was a significant increase in survival rates of extremely preterm infants from 31% to 40% (RR 1.24, 95% CI 1.02, 1.50) after the publication of the Swiss guidelines. This improvement was largely explained by significantly improved survival from 42% to 60% (p = 0.01) among infants born at 25 completed weeks because of decreased NICU mortality. Improved survival was not associated with statistically significant changes in the incidence of short-term complications. Despite national guidelines, considerable centre-to-centre outcome differences have persisted.
Conclusions: The publication of the Swiss guidelines was followed by significantly improved survival of extremely preterm infants but had no impact on centre-to-centre differences.
Statistics from Altmetric.com
Technological advances in the last 30 years have lead to unprecedented survival rates for extremely premature infants. Survival of infants who were considered to be marginally viable 20 years ago has now become the rule rather than the exception.1 2 3 4 Over the same time period, neonatologists continued to push the limit of viability to lower and lower gestational ages. Survival of infants with a gestational age of only 22 0/7 weeks5 or a birth weight of only 280 g6 has been reported. However, this success has its price and the burden of intensive care imposed on borderline viable infants who ultimately do not survive, and high rates of neurosensory impairments among survivors have raised serious ethical questions.7 8 9 10 11 Many national paediatric and neonatal societies have responded to these concerns with the publication of guidelines to support ethical decision making in the care of infants born at the limit of viability.12 13 14 15 16 17 18
The Swiss Society of Neonatology published its recommendations for the care of infants born at the limit of viability (gestational age between 22 0/7 weeks and 25 6/7 weeks) in 2002.13
Briefly, the Swiss recommendations suggest that in extremely preterm infants, with a gestational age <24 0/7 weeks, preference should in general be given to comfort care, whereas provisional intensive care becomes a valid option in borderline viable infants with a gestational age ⩾24 0/7 weeks. The recommendations emphasise that a priori restrictions of intensive care measures used during provisional intensive care should be avoided.13
Because the Swiss recommendations leave considerable room for individualised decision making, stressing the limited precision of gestational age determination, the importance of biologic variability and emphasising parental participation in ethical decision making, it is conceivable that there are local differences in how these guidelines are interpreted and applied to clinical practice.
With this study, we wanted to assess if the publication of the Swiss guidelines on the care of infants born at the limit of viability have had an impact on their survival and short term complication rates. In addition, we wanted to investigate whether the approach to these patients has become more uniform among the nine neonatal intensive care units (NICUs) that care for these infants in Switzerland.
Methods
We used the well established Swiss Minimal Neonatal Data Set to collect data on all live born extremely preterm infants with a gestational age between 22 0/7 and 25 6/7 weeks (ie, 22–25 completed weeks) born between 1 January 2000 and 31 December 2004. All nine NICUs and their affiliated paediatric units in Switzerland that manage extremely preterm infants participated in this study. Data were collected prospectively through a computerised questionnaire distributed to collaborators from each centre. The questionnaire was constructed to obtain basic demographics, survival data and short term complications, including periventricular/intraventricular haemorrhage (PIVH), cystic periventricular leukomalacia (PVL), retinopathy of prematurity (ROP) and moderate/severe bronchopulmonary dysplasia (BPD). Gestational age was calculated based on obstetric expected due dates if the mother’s dates were consistent with ultrasound examinations during the first trimester of pregnancy. Across all participating centres, gestational age was defined according to the International classification of disease19 as the postmenstrual age in weeks and days. The time period between 25 weeks and 0 days and 25 weeks and 6 days, for example, is termed 25 completed weeks of gestation; the fetus has completed 25 weeks and is in the 26th week of gestation. PIVH was classified according to Papile et al,20 ROP was staged as described by the Committee for the Classification of Retinopathy of Prematurity,21 and BPD severity was graded according to the NICHD consensus conference paper.22 Completed data forms were sent to a central site (Department of Neonatology, University Women’s Hospital, Zurich, Switzerland) where they were collected and evaluated. To verify that the outcome of all live born infants, including those who had died in the delivery room (DR), could be analysed, the birthing log books or electronic data bases at all participating hospitals were reviewed by one of us (NF).
To evaluate if the 2002 publication of the Swiss guidelines on the care of infants born at the limit of viability have had an impact on the outcome of infants with a gestational age between 22–25 completed weeks, pooled data of the years 2000/2001 were compared with pooled data of the years 2003/2004. For these analyses, extremely preterm infants born in 2002 were excluded since we considered this year a transitional period.
In order to explore the variability of outcomes among extremely preterm infants, we performed a centre-to-centre comparison of delivery room and NICU mortality rates of all live born infants with a gestational age between 22 0/7 and 25 6/7 weeks over the entire five-year study period (2000–4). In addition, we compared the incidence of PIVH III/IV, cystic PVL, severe ROP (⩾ stage III) and moderate to severe BPD in survivors.
Statistical analyses were performed with GraphPad Prism 5 and GraphPad Instat (GraphPad Software Inc., San Diego, USA). Logistic regression analyses were performed using Stata10 (StataCorp LP, College Station, Texas, USA). Normally distributed continuous data are presented as mean with standard deviation. To compare groups Student t test was used. Comparisons of proportions were performed calculating relative risks (RR) or odds ratios (ORs) with 95% confidence intervals (CIs) or Fisher’s exact test for smaller groups. Two-sided p values<0.05 were considered significant.
Nonparametric correlation between two random variables was quantified by the Spearman correlation coefficient r. Linear regression analyses were done to show the dependence of centre-specific survival rates from centre-specific intubation rates. The centres were weighted to adjust for the sample sizes and multiple regressions were calculated to adjust for gestational age and birth weight.
To compare centre-to-centre variation in survival rates an overall logistic regression equation was calculated including birth weight (in grams), gestational age (in days), sex and singleton/multiple birth as predictor variables (antenatal corticosteroid treatment had to be excluded due to high proportion of missing data). Based on this regression equation the expected mortality rates for each centre were computed and compared with the observed mortality rates.
Results
Trends in survival and short-term complication rates
Over the entire five-year study period, there were 516 live births of borderline viable infants with a gestational age between 22–25 completed weeks in Switzerland. Following exclusion of the 2002 cohort (n = 92), the outcome of 220 infants born in the years 2000/2001 (period 1 = prior to the publication of the Swiss recommendations) could be compared with the outcome of 204 infants born in the years 2003/2004 (period 2 = following the publication of the Swiss recommendations) (fig 1). Mean gestational age and mean birth weight of infants studied in period 1 and 2 remained constant except for an increase in birth weight among infants born at a gestational age of 23 0/7 to 23 6/7 weeks (table 1). In addition, there was no significant change in the rate of caesarean sections (period 1: 56%, period 2: 46%, p = 0.065).
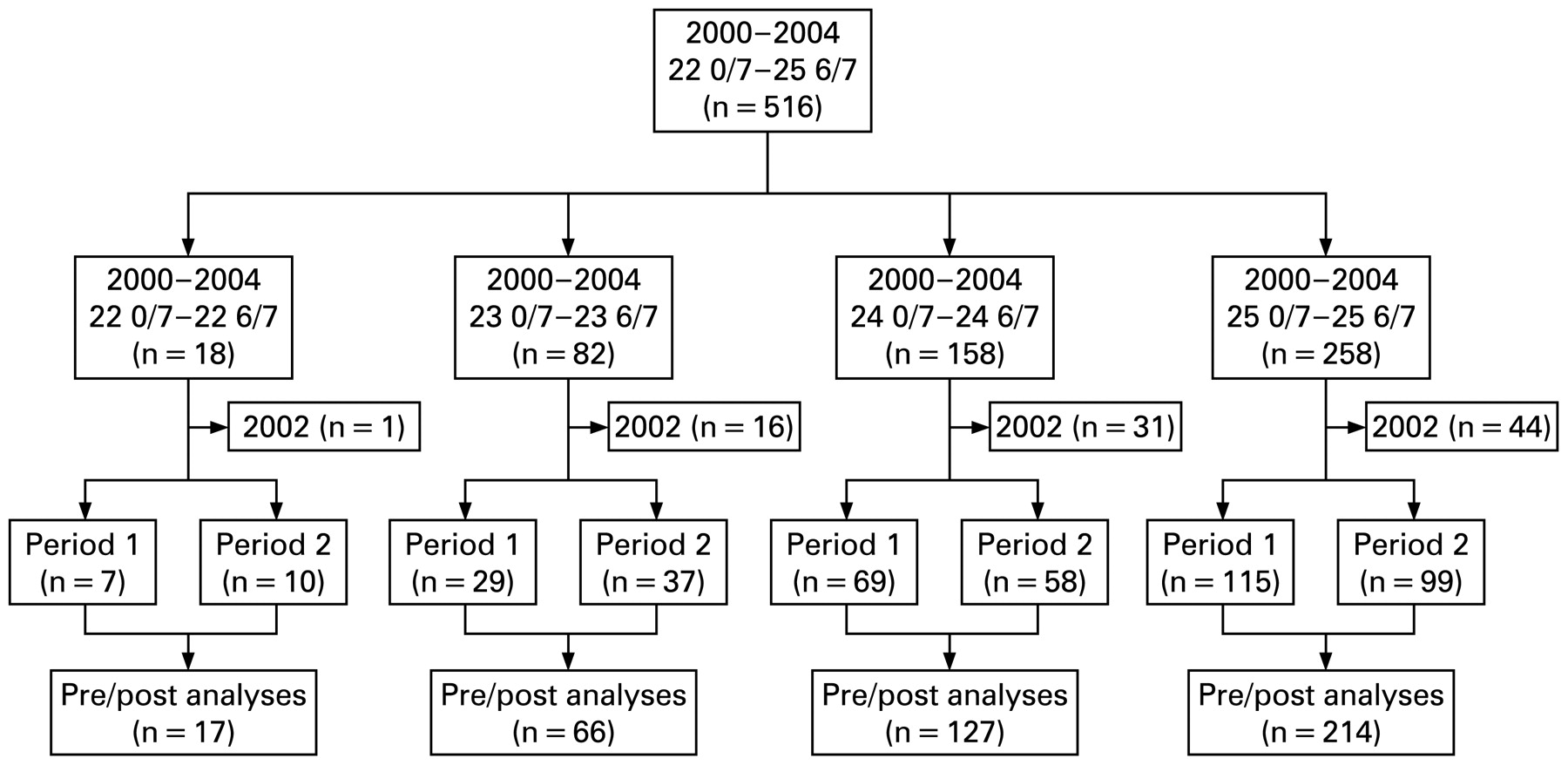
Study population. Patients born in 2002 (n = 92) were excluded in the pre/post analyses (n = 424; period 1: 2000/2001, period 2: 2003/2004); for analyses of centre-to-centre variations, all patients (n = 516) were included.
Mean gestational age (GA) in weeks and mean birth weight (BW) in grams (g) of infants studied in period 1 and period 2
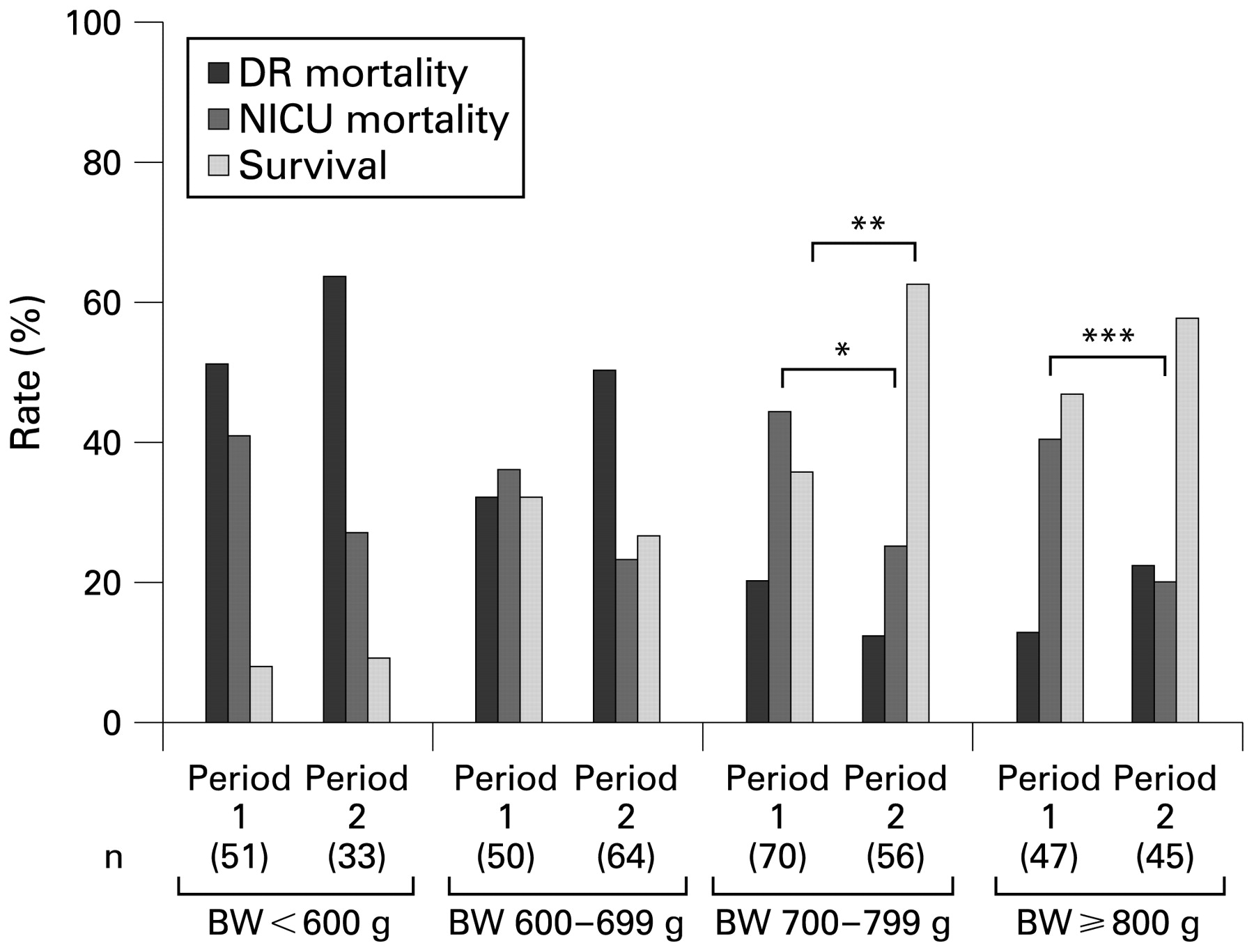
From period 1 to period 2, the survival rate of extremely preterm infants with a gestational age between 22–25 completed weeks increased significantly from 31% to 40% (RR 1.24, 95% CI 1.02, 1.50). Subgroup analyses (figs 2, 3) revealed that the overall improvement in survival was largely explained by significantly improved survival in the more mature extremely preterm infants with a gestational age of 25 completed weeks from 42% in period 1 to 60% in period 2 (p = 0.01) because of a decrease in their NICU mortality rate from 49% to 27% (p = 0.002). DR mortality rates remained unchanged among all four gestational age categories (fig 2). Consistent with these observations, analyses of birth weight-specific survival rates showed a statistically significant improvement among infants with a birth weight between 700 and 799 g (p = 0.004) as well as a trend towards improved survival among infants with a birth weight >800 g (fig 3).

Gestational age (GA) specific delivery room (DR), neonatal intensive care unit (NICU) mortality and survival rates before (period 1) and after (period 2) the publication of the Swiss recommendations (*p = 0.002, **p = 0.01).

Birth weight (BW) specific delivery room (DR), neonatal intensive care unit (NICU) mortality and survival rates before (period 1) and after (period 2) the publication of the Swiss recommendations. (BW missing in n = 2 in period 1 and in n = 6 in period 2) (*p = 0.027, **p = 0.004, ***p = 0.042).
From period 1 to period 2, centre-specific survival rates of extremely preterm infants increased in six centres, remained constant in two, and decreased in one. Due to the relatively small numbers of patients cared for in the individual centres, these changes were not statistically significant in any of the centres. The range of centre-specific survival rates remained substantial (period 1: 0–55%, period 2: 0–64%).
Improved survival rates were not associated with prolonged hospital stays. Among infants who were admitted to the NICU for provisional intensive care but ultimately died, the average length of stay in the NICU was 17 days in period 1 and 12 days in period 2 (p = 0.42). Similarly, average length of hospital stay among survivors did not change significantly (122 days and 111 days in period 1 and 2, respectively, p = 0.15).
Based on available data, improved survival of extremely preterm infants was not associated with statistically significant changes in the incidence of PIVH III/IV, cystic PVL, ROP⩾stage III and/or moderate to severe BPD in survivors (table 2). Of importance, in both time periods, there were no patients with threshold ROP and no patient required laser therapy. PIVH III/IV rates were much higher in non-survivors (27% and 35% in period 1 and period 2, respectively; OR 1.49, 95% CI 0.69, 3.16), suggesting that high grade PIVH may have been important in redirection of care decisions.
Comparison of the incidence of short-term complications in survivors before (period 1) and after (period 2) the publication of the Swiss recommendations
Centre-to-centre variations
The number of extremely preterm infants with a gestational age between 22 0/7 and 25 6/7 weeks cared for at the nine centres over the entire five-year study period varied between 14 and 117 (median 51). DR mortality rates ranged between 11% and 65% and NICU mortality rates between 32% and 65%, resulting in overall survival rates ranging between 16% and 53%.
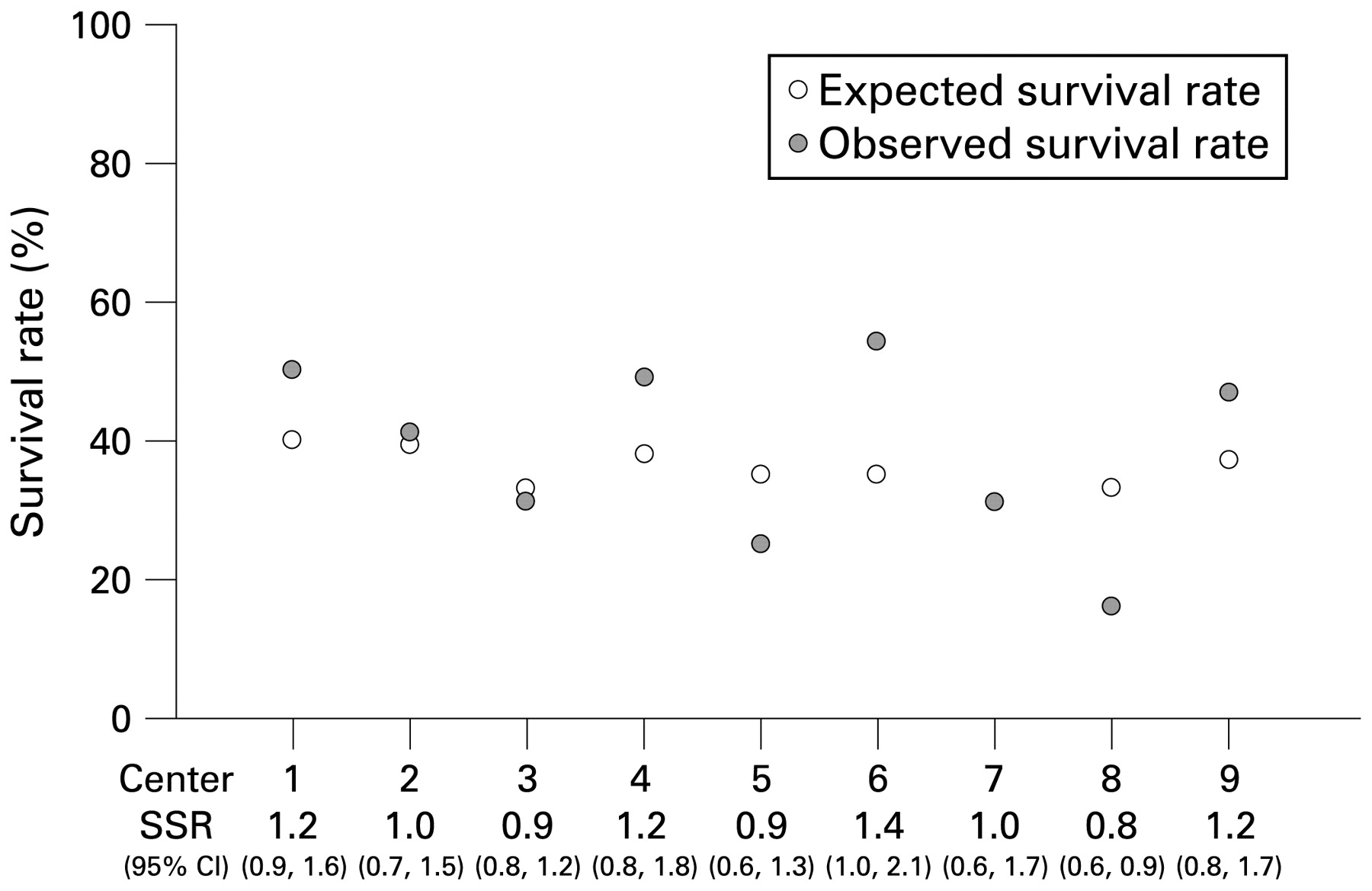
To adjust for potential baseline population differences, an overall logistic regression equation was calculated including birth weight (in grams), gestational age (in days), sex and singleton/multiple birth as predictor variables. Based on this regression equation the expected mortality rates for each centre were computed and compared with the observed mortality rates. The standardised survival ratio varied between 0.8 and 1.4 (fig 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Expected and observed survival rates in the nine participating centres over the five-year study period (2000–4). SSR: standardised survival ratio.
To further analyse these differences, we compared intubation rates with survival rates using the former as a proxy for a proactive approach, that is, the willingness to provide provisional intensive care. For this analysis, 9% of cases had to be excluded because information on intubation was not available. Survival rates correlated closely with intubation rates in a multiple regression model (r = +0.83, p<0.001) after adjusting for gestational age and birth weight (R2 = 69.5%). The centre with the lowest intubation rate had the lowest survival rate (17% and 16%, respectively); in contrast, the centre with the highest intubation rate had the highest survival rate (81% and 51%, respectively). An almost identical association was found between surfactant administration rates and survival rates (data not shown).
Finally, we investigated whether higher survival rates would be associated with larger numbers of survivors with clinically significant short term complications. Because information on the incidence of ROP and cystic PVL was missing in 24% and 11%, respectively, this analysis had to be restricted to the incidence of moderate to severe BPD (data missing in 8% of survivors). We found a negative correlation between survival and BPD rates (Spearman r = −0.89). Importantly, the proportion of survivors without any major morbidity (PIVH III-IV, cystic PVL, ROP III-V or moderate/severe BPD) was much higher in the centre that was most aggressive in providing provisional intensive care compared to the centre with the lowest intubation rate (68% versus 21%, RR 0.29, 95% CI 0.16, 0.74).
Discussion
The main purpose of the publication of the Swiss recommendations on the care of infants born at the limit of viability in the year 2002 was to provide up-to-date information on outcomes of extremely preterm infants, to offer guidance in ethical decision making and to ensure that the management of these infants became more uniform across the country. In addition, the recommendations highlighted the importance of quality assessment including the collection of both short-term and long-term outcome data.
The current study provides complete information on survival rates of infants born at the limit of viability between 2000 and 2004 in Switzerland. Comparison of two two-year cohorts born before and after the year of publication allowed us to assess a temporal trend both for the entire country as well as for individual centres. Using data from the entire five-year study period, we analysed centre-to-centre differences of survival rates and explored possible explanations for the observed outcome variability.
Impact of guidelines on survival and short-term complication rates
Overall, gestational age-specific survival rates of extremely preterm infants in Switzerland are comparable to previous population-based reports from the UK,23 France24 and Belgium,25 but significantly lower than in Canada,26 Scandinavia27 28 and Australia (table 3).29
Comparison of survival rates of extremely preterm infants in Switzerland with survival rates in several other European countries, Canada and Australia
Following the publication of the Swiss recommendations for the care of infants born at the limit of viability,13 survival of extremely preterm infants with a gestational age between 22–25 completed weeks improved significantly from 31% to 40%, mainly because of a statistically significant decrease in NICU mortality rates among the more mature infants with a gestational age of 25 completed weeks. These findings are remarkably similar to the observations made by Field et al for the Trent health region in the UK between 1994–1999 and 2000–2005.30 In their population-based study, improved survival of infants born at 22–25 completed weeks of gestation from 36% to 47% was attributable to substantial improvements in survival of infants born at 24 and 25 completed weeks, whereas survival rates of less mature infants remained unchanged. Riley et al described a similar trend in a single centre setting between the early and late 1990s but with significantly higher survival rates in both time periods (table 4).31
Comparison of trends in survival rates of extremely preterm infants in the UK (Trent health region, London) and Switzerland
The Swiss recommendations may have affected the extent to which provisional intensive care was provided, since they emphasise that a priori restrictions of intensive care measures should be avoided. In addition, the recommendations may also have had an impact on redirection of care decisions. In contrast, since DR mortality rates remained unchanged, the Swiss recommendations apparently had no or minimal impact on decisions regarding the initiation of intensive care in the DR. Several authors have shown that proactive DR management of extremely preterm infants improves survival.32 33 34
The observation that the proportion of infants with a gestational age of less than 24 weeks was larger in period 2 than in period 1 (23% and 16%, respectively) (table 1) could either be due to chance or suggest that some patients were misclassified on purpose to avoid the use of intensive care measures. However, this would not challenge our main findings because the significant increase in survival from period 1 to period 2 is largely explained by improved survival in the highest gestational age category the proportion of which did not change from period 1 to period 2 (52% and 49%, respectively).
The recorded average NICU stays in non-survivors and the average length of hospital stays in survivors suggest that a more proactive treatment among infants admitted to the NICU neither lead to prolonged suffering in doomed infants nor prolonged hospital stays in survivors.
Only limited conclusions can be drawn from our data on the incidence of short-term complications because of missing data (PIVH III/IV: 9%, cystic PVL: 9%, ROP III-V: 25% and moderate to severe BPD: 8%). Nevertheless, these rates are comparable to those reported in other population-based studies of extremely preterm infants.25 26 27 With regards to ethical decision making, rates of short-term complications are of limited value and ascertainment of comprehensive long-term outcome data is essential. Some reports claim that improved survival is not associated with an increased risk of severe disability,32 34 while others have described that proactive management strategies improve survival but also increase the number of survivors with disabling cerebral palsy.35 36
Centre-to-centre variations
Our study shows that the outcome of extremely preterm infants varies substantially between centres in Switzerland. These variations persisted after the publication of national guidelines. Some of the observed variation may have occurred by chance because in some centres the number of extremely preterm infants cared for is very small (median 51, range 14–117). We did not find any significant differences in baseline population demographics (gestational age, birth weight, sex, singleton/multiple birth) between centres. It seems likely that the observed differences are at least in part due to variations in ethical decision making. The centre-to-centre differences were observed for both DR and NICU mortality rates (data not shown). Since DR mortality most frequently is the result of primary non-intervention rather than failed resuscitation, the centres may differ in their attitude towards providing provisional intensive care. This interpretation is also supported by the observation that intubation rates vary widely and correlate with survival rates. Differences in NICU mortality rates may be related to differences in illness severity; alternatively, centres may have different thresholds to consider redirection of care following provisional intensive care.
While average survival rates of these infants in Switzerland are comparable to those reported from other population-based studies,23 24 25 in some Swiss centres survival rates are much higher and close to those reported from Canada,26 Scandinavia27 28 and Australia29 but still well below single-centre experiences published from the USA37 and Germany (table 3).32
Tommiska et al have made similar observations for NICUs in Finland.38 In a 1996/1997 cohort of 349 live born ELBW infants (birth weight <1000 g, gestational age at least 22 weeks), they noted a two-fold difference in neonatal mortality rates between secondary and tertiary level hospitals (59% vs 32%, p<0.001). When the authors analysed a second cohort of ELBW infants born three years later (1999/2000), they found no improvement in mortality rates and a persistence of centre-to-centre differences.39 In a report on 2478 live born ELBW infants from the Neonatal Research Network of the National Institute of Child Health and Human Development (NICHD 1993/1994), Vohr et al found striking differences in centre outcomes after adjusting for demographics and antenatal interventions.40 They suggested that variations in active resuscitation (5%–28%) and in survival rates (51%–72%) reflect in part differences in management styles. Finally, Lee et al evaluated outcomes of infants of 22 to 25 weeks’ gestation in 12 hospitals in the Canadian NICU Network.41 They found that delivery room deaths ranged from 9% to 57% and neonatal survival ranged from 32% to 79%.
Limitations of the study
The present population-based study has examined the temporal trend of survival rates in infants born at the limit of viability in Switzerland over a five-year period. In addition, centre-to-centre differences both with regards to management strategies and outcome could be examined. The study has several limitations. Although we have included all live born infants cared for at the nine participating centres (including all DR deaths) and their affiliated paediatric units, there may have been extremely preterm infants who were born alive but then died in delivery rooms of smaller hospitals. At least for infants born after 23 weeks’ gestation, this number is likely to be small because antenatal transfer of high risk pregnancies is well established in Switzerland. Finally, because the information on short-term complication rates in survivors is incomplete and, most importantly, long-term outcome data is not yet available, it is difficult to asses the overall impact of the observed trend in survival rates as well as the observed centre-to-centre differences. These studies are under way and will provide important complementary information to guide ethical decision making.
Conclusions
In Switzerland, overall survival rates of extremely preterm infants with a gestational age between 22 and 25 completed weeks are comparable to those reported in population-based studies from England, France and Belgium, but significantly lower than in Canada, Scandinavia and Australia. Improved survival following the publication of the Swiss guidelines on the care of infants born at the limit of viability was restricted to infants with a gestational age of 25 completed weeks. There are large centre-to-centre differences in survival rates of extremely preterm infants in Switzerland which can at least in part be explained by different management approaches to these infants. Variations in practice have persisted after the publication of the Swiss guidelines. It will be crucial to comprehensively assess long-term outcomes in all survivors to fully evaluate the different approaches to infants born at the limit of viability in Switzerland.
What is already known on this topic
Ethical decision making in extremely preterm infants at the limit of viability varies widely across Europe.
There are large differences in survival rates of extremely preterm infants between countries and even between centres within the same country.
What this study adds
The publication of the Swiss guidelines for the care of infants at the limit of viability (22–25 completed weeks) was followed by increased survival rates in the more mature extremely preterm infants (25 completed weeks) without increasing the rate of short-term complications.
In Switzerland, there are considerable centre-to-centre differences in survival rates that have persisted after the publication of national guidelines.
Acknowledgments
We would like to acknowledge the following centres for providing their data to the Swiss MNDS: Aarau: Kantonsspital Aarau, Kinderklinik (G Zeilinger); Basel: Universitäts-Kinderspital beider Basel, Abteilung für Neonatologie (C Bührer); Bern: Frauenklinik und Medizinische Kinderklinik, Abteilung für Neonatologie (M Nelle), Inselspital, Abt. für Intensivpflege, Universitätskinderklinik (B Wagner); Chur: Rätisches Kantons- und Regionalspital, Kinderklinik (W Bär); Genève: HUG, Clinique de pédiatrie, Département de pédiatrie/Hôpital des Enfants (Michel-Eric Berner); Lausanne: CHUV, Département de pédiatrie (A Moessinger), CHUV, SI pédiatriques, médico-chirurgicaux (J Cotting); Luzern: Kantonsspital Luzern, Kinderspital Pädiatrie (TM Berger); St. Gallen: Kantonsspital St. Gallen, Klinik für Geburtshilfe und Gynäkologie (A Malzacher), Ostschweizer Kinderspital, Intensivpflege- und Frühgeburtenstation (J P Micallef); Zürich: USZ, Klinik für Neonatologie, Departement Frauenheilkunde (H-U Bucher), Abteilung für Intensivmedizin und Neonatologie, Universitätskinderklinik Zürich (O Bänziger).
REFERENCES
Footnotes
Competing interests None.
Provenance and Peer review Not commissioned; externally peer reviewed.
Linked Articles
- Fantoms