Article Text

Abstract
Introduction: Many practitioners routinely treat infants whose mean arterial blood pressure in mm Hg is less than their gestational age in weeks (GA).
Objective: To assess the effectiveness of utilising a combined approach of clinical signs, metabolic acidosis and absolute blood pressure (BP) values when deciding to treat hypotension in the extremely low birthweight (ELBW) infant.
Methods: Retrospective cohort study of all live born ELBW infants admitted to our neonatal intensive care unit over a 4-year period. Patients were grouped as either normotensive (BP never less than GA), hypotensive and not treated (BP<GA but signs of good perfusion; we termed this permissive hypotension) and hypotensive treated (BP<GA with signs of poor perfusion).
Results: 118 patients were admitted during this period. Blood pressure data were available on 108 patients. 53% of patients were hypotensive (mean BP in mm Hg less than GA in weeks). Treated patients had lower birth weight and GA, and significantly lower blood pressure at 6, 12, 18 and 24 h. Normotensive patients and patients designated as having permissive hypotension had similar outcomes. Mean blood pressure in the permissive group increased from 26 mm Hg at 6 h to 31 mm Hg at 24 h. In a logistic regression model, treated hypotension is independently associated with mortality, odds ratio 8.0 (95% CI 2.3 to 28, p<0.001).
Conclusions: Blood pressure spontaneously improves in ELBW infants during the first 24 h. Infants hypotensive on GA criteria but with clinical evidence of good perfusion had as good an outcome as normotensive patients. Treated low blood pressure was associated with adverse outcome.
Statistics from Altmetric.com
Although acceptable blood pressure ranges are not known for the extremely low birthweight (ELBW) infant, many neonatologists routinely treat infants whose mean arterial blood pressure is less than their gestational age in weeks.1 This guideline2 is arbitrary and the approach seems difficult to justify as it neglects the considerable variation between published blood pressure standards,3–5 the normal spontaneous increase in blood pressure over the first few hours and days of life,3 and the very poor relationship between blood pressure and systemic blood flow.6 There is also conflicting evidence relating hypotension to adverse outcome.7
What is already known on this topic
Many extremely preterm infants receive treatment for hypotension.
Hypotension in newborn infants is usually defined as mean arterial blood pressure in mm Hg that is less than mean gestational age in weeks.
What this study adds
A blood pressure less than the gestational age does not necessarily need to be treated.
Global assessment of cardiovascular status and intervention for hypotension restricted to infants with poor perfusion may have good clinical outcomes and warrants further evaluation.
Global assessment of cardiovascular status includes assessment of other easily evaluable physical findings including capillary refill, skin colour, heart rate, urine output, level of activity and biochemical findings, in particular the degree of acidosis. Although this assessment of the adequacy of end organ perfusion is crude and not infallible, and each finding taken in isolation may be a poor indicator of perfusion, together they may provide more information than absolute blood pressure values alone. There is no evidence that attempts to achieve a “normal” blood pressure based on absolute reference values will improve outcomes, and the therapies available may be potentially toxic or dangerous.8–10
We have consistently relied upon the assessment of clinical signs and degree of acidosis, in addition to absolute blood pressure values, before intervening in the management of low blood pressure states. We evaluated this approach in the ELBW infant in the first 72 h of life. We hypothesised that patients with a blood pressure less than gestational age but who had evidence of good tissue perfusion and were not treated (permissive hypotension) had as good an outcome as patients with a lowest recorded blood pressure greater than gestational age. A secondary hypothesis was that infants who received therapy for low blood pressure had worse outcomes than those with low blood pressure but without symptoms.
METHODS
This was a retrospective review of all live born ELBW infants admitted to our neonatal intensive care unit (NICU) over a 4-year period from January 2000 to December 2003 inclusive. Patients were identified from a computer admission database in the NICU and were cross-referenced with an admission data book containing details of all admissions to the NICU. Patients were included if their birth weight was less than 1000 g and were excluded if they had any lethal congenital malformation. The individual patient records and patient flow sheets were reviewed by two of the authors (ED, FaH).
Gestational age was determined from date of last menstrual period (when accurate) or early dating ultrasound. Respiratory distress syndrome (RDS) was defined as the need for assisted ventilation (continuous positive airway pressure (CPAP) or mechanical ventilation) and a typical radiographic appearance. Severe intraventricular haemorrhage (IVH) implied either a large amount of intraventricular blood causing dilatation of the lateral ventricle or intracerebral haemorrhage. Periventricular leukomalacia (PVL) was defined as echolucent areas in the periventricular area on cranial ultrasound. Necrotising enterocolitis (NEC) was classified as the presence of intramural gas on abdominal radiograph, perforation or evidence of intestinal necrosis at surgery or autopsy. Patent ductus arteriosus (PDA) was diagnosed by clinical signs and echocardiography confirmation.
Data collected included blood pressure on admission and at 6-hourly intervals for the first 72 h, the lowest absolute mean blood pressure during the first 72 h and the mean value immediately prior to the administration of a volume bolus infusion or inotrope. Invasive blood pressure recordings from a calibrated transducer attached to an arterial catheter were used when available; in the remainder automated oscillometric cuff blood pressures were used. Illness severity was assessed by CRIB II scores.11
The approach to management of hypotension was individualised to each patient.
The decision to start any agent was made by the attending physician and was always based on a combination of absolute mean blood pressure values, clinical signs suggesting poor tissue perfusion (including colour, heart rate, capillary refill and urine output), and absolute and temporal change in acidosis. Patients with a blood pressure less than gestational age are started on inotropic agents if they have signs of poor tissue perfusion. We therefore grouped our cohort as follows: either normotensive (BP never less than GA), hypotensive and not treated (BP<GA but signs of good perfusion; we defined this as permissive hypotension), hypotensive treated (BP<GA with signs of poor perfusion) and hypotensive infants whose only intervention was a blood transfusion as they also had a low haemoglobin concentration.
An independent third party who had not been involved in the data collection performed data analysis. Comparison between groups was made using ANOVA and χ2 analysis. p Values less than 0.05 were considered statistically significant.
Univariate regression analysis and multivariate regression analysis were performed to identify risk factors associated with mortality at 7 days and overall mortality. Results are presented as p values and point estimate odds ratios and 95% confidence intervals. Statistical analysis was performed using SPSS software.
RESULTS
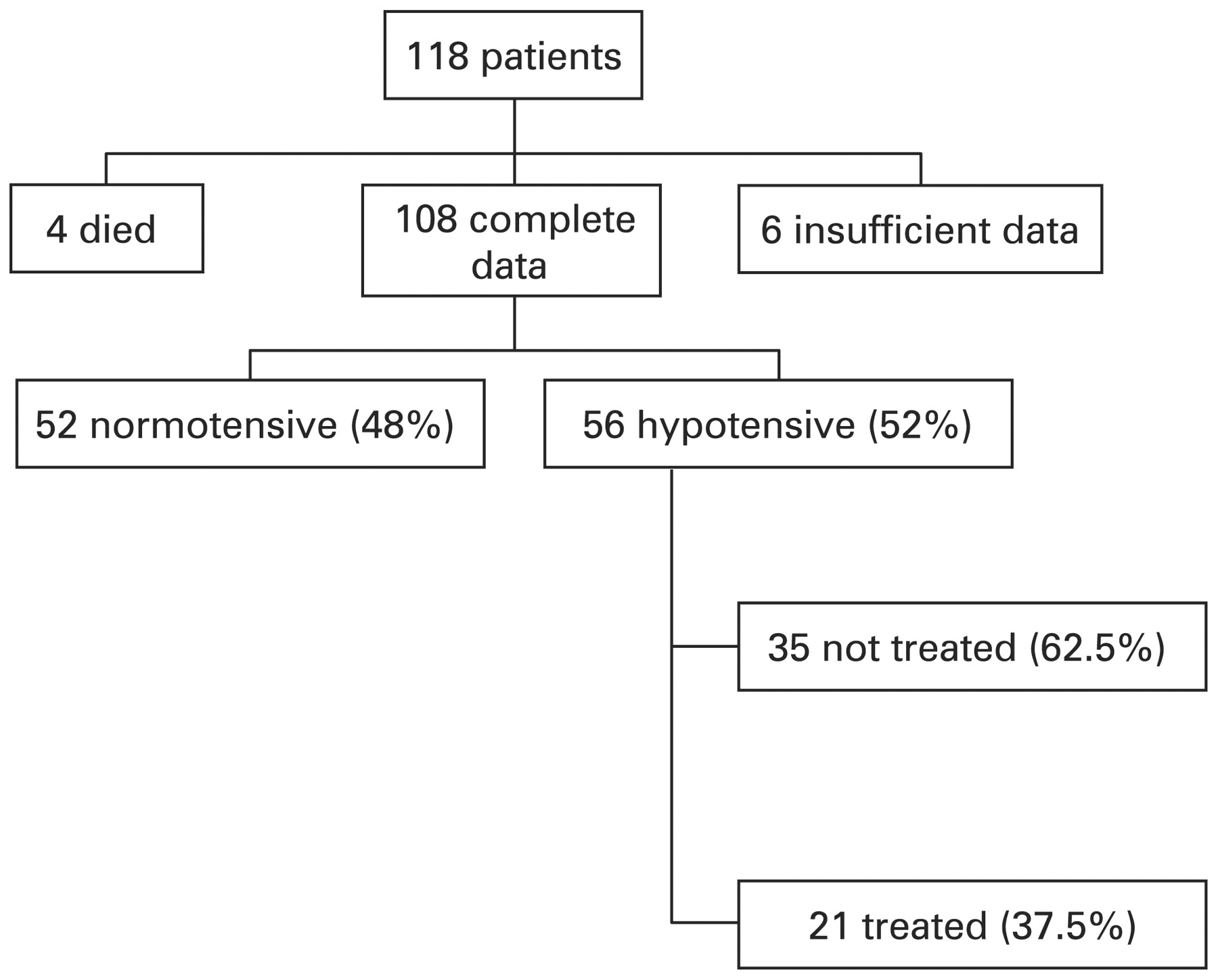
A total of 118 patients were admitted to the NICU during this period. Blood pressure data were available on 108 patients (91.5%). Four patients died within 4 h of admission and no blood pressure data were available. No recorded blood pressure data were available in another six patients, all of whom survived to discharge without serious complications. Invasive blood pressure recordings were available in 67 patients (62%). Hypotension, when defined as a blood pressure in mm Hg less than gestational age in weeks, was present in 56 patients (52%). Eighteen (16.6%) patients received either a fluid bolus or epinephrine infusion or both. A further four patients with hypotension received a blood transfusion (none given as boluses) during the first 3 days because of low haemoglobin and were infused over 2–3 h (fig 1). These patients are analysed both separately and as part of the permissive hypotension group.

{kind=link}
Flow diagram showing distribution of patients according to diagnosis and treatment of hypotension.
Therefore, 22 (39%) of the “hypotensive” patients had treatment to improve blood pressure. These patients were significantly more immature, of slightly lower birth weight (not significant) and had significantly higher illness severity scores than the permissive hypotension babies. Treatment consisted of inotrope alone in 10, inotrope and volume in four, and volume alone in three (normal saline bolus). The 14 patients (11.8%) who received an inotrope were treated with low dose epinephrine in all cases. The remaining 34 babies (61%) had no intervention as clinical evaluation showed tissue perfusion was adequate.
Patients who received intervention had significantly lower blood pressure at 6, 12, 18 and 24 h than the normotensive or permissive hypotension infants. Normotensive patients and patients designated as having permissive hypotension had similar short-term outcomes, including mortality, NEC (Bell stage 2 or more), spontaneous intestinal perforation, severe intracranial haemorrhage, cystic PVL, or the combined outcome of survival to discharge without any of these complications (table 1).
We analysed the outcomes of survival and survival without serious short-term complications (as listed above) with multivariate logistic regression models. On univariate analysis gestational age, CRIB score and treatment of hypotension were significantly associated with the two outcomes (table 2). For each of these two outcomes, the other factors were no longer significant when hypotension treatment was included in the model using a forward stepwise conditional technique (SPSS v 15.0). The adjusted ORs for mortality and for the combined outcome of mortality or NEC (Bell stage 2 or more), spontaneous intestinal perforation, severe intracranial haemorrhage or cystic PVL are shown in table 2.
If we include the four infants who only received a blood transfusion in the permissive hypotension group, the percentage of survival without serious short-term morbidity falls to 71%; this does not affect the significant differences between the groups.
DISCUSSION
This study addresses the role of clinical assessment of end organ perfusion when initiating treatment of hypotension, defined as blood pressure less than GA, in the ELBW infant during the first 72 h of life. Short-term outcome in patients who were hypotensive but had evidence of good perfusion was as good as in patients who were normotensive. This highlights a number of points. Firstly, absolute blood pressure values are only one indicator of circulatory status. Secondly, it confirms that a mean blood pressure less than gestational age in weeks alone is not a predictor of poor outcome. Thirdly, global assessment of cardiovascular status and intervention for hypotension restricted to infants with poor perfusion may be associated with good clinical outcomes and should be further evaluated.
In one report of data from six NICUs, 40–50% of very low birthweight infants received intervention for hypotension.12 Another study showed that between 29% and 98% of extremely low gestational age newborns received intervention; the main source of the variation was the NICU in which they were treated.13 Treatment typically consists of, often multiple, volume infusions, followed by inotrope infusions, predominantly dopamine. There is also a growing trend for the use of hydrocortisone therapy in hypotensive ELBW infants.14 15 A recent study has even addressed the potential role of prophylactic steroids to reduce the need for inotropic agents.16 The entry criteria for starting blood pressure support agents in the two randomised controlled trials14 16 mentioned above included a mean arterial pressure less than the gestational age. We could find no evidence to support the use of this entry criterion alone, which appears to have arisen without being adequately investigated. Furthermore, it neglects the normal spontaneous increase in blood pressure over the first few hours and days of life.3 Our data demonstrate that many of these babies may do well without any intervention at all. Only 11% of our ELBW infants received an inotrope, which consisted of low dose epinephrine in all cases. That these were the sickest babies was evidenced by their high CRIB II scores and subsequent outcome. Other authors have recently reported good outcomes with a similar restricted approach.17
Clinical signs are by nature subjective and may be variably assessed. Their reproducibility may also be questionable. Evidence in relation to the role of capillary refill times in assessing end organ blood flow in the neonate is conflicting.18 19 Values exist for the term neonate18 but there are limited data on capillary refill times in the preterm infant.19 Osborn et al have also shown that there is a weak relationship between capillary filling and superior vena cava flow.20 Because the normal urine output for an ELBW infant in the first 24 h is already very low, it is difficult to define low output. However, the presence of good urine output is reassuring. Previous investigations of the base deficit in ELBW infants have shown a correlation with poor outcome. Serum lactate measurements are probably preferable21 but were not routinely recorded in our infants. Currently, no validated clinical scoring system is available to guide intervention in hypotensive infants. However, inclusion of these factors in decision making appears to decrease the number of infants who receive treatment without putting them at increased risk.
There are some limitations to our retrospective study. Blood pressure values were generally recorded hourly so it is possible marked swings in blood pressure, which may be associated with IVH,22 may have been missed and some babies who were hypotensive between these readings may have been overlooked. Over one third of the blood pressure readings were made non-invasively. These recordings may have overestimated the true mean blood pressure, which may have been lower if measured invasively.23 However, there were similar percentages of non-invasive recordings in both the normotensive and the permissive hypotensive groups. For the purpose of this report, we have only looked at short-term outcomes, including morbidity and mortality. Data collection on long-term neurodevelopmental outcome in this cohort of patients is ongoing.
In summary, a blood pressure less than the gestational age does not necessarily need to be treated. We observed good outcomes in hypotensive infants with good clinical perfusion who were carefully observed rather than treated. Using the principle that less intervention with similar outcomes is preferable, we believe that our restricted approach to hypotension (permissive hypotension) warrants further evaluation. Prospective randomised studies of clinical outcomes with standard versus restricted treatment of hypotension are essential.
REFERENCES
Footnotes
Competing interests: None.
Funding: EMD was funded by the Department of Pediatrics, McGill University, Clinical/Research Fellowship in Academic Pediatrics.
Linked Articles
- Fantoms