Article Text

Abstract
A considerable body of human and animal experimental evidence links antenatal inflammation to both accelerated maturation and adverse development of the lung. Initial reports suggest that in preterm infants histological chorioamnionitis is associated with a decreased incidence of respiratory distress syndrome (RDS), while the incidence of bronchopulmonary dysplasia (BPD) is increased. Considerable variation exists in the findings of subsequent human studies, largely dependent on differences in inclusion and exclusion criteria. Taking these differences into account, recent studies generally seem to confirm the effect of chorioamnionitis on RDS incidence, while no effect on BPD is seen. The increased use of antenatal steroids and the diminished effects of secondary pro-inflammatory hits seem to explain part of this change. Additional research is needed to explore these complex interactions and their underlying mechanisms, and evaluate the long term pulmonary effects of antenatal inflammation.
Statistics from Altmetric.com
The effects of antenatal inflammation on both short and long term outcome in preterm infants have received increasing attention over the last few years. Chorioamnionitis is clearly associated with preterm birth and its incidence in preterm infants increases with decreasing gestational age.1–3 The primary process in the aetiology of intrauterine inflammation is believed to be ascending bacterial invasion from the cervicovaginal tract,4 5 although several other routes have been postulated.5 Bacteria may then spread across the chorioamniotic membranes and cause chorioamnionitis.4 5 In a subset of patients intrauterine inflammation is accompanied by a fetal response, believed to reflect the more serious end of the continuum. Initial signs of fetal inflammation in preterm infants are seen in the chorionic plate, followed by involvement of the umbilical cord vessels, often referred to as “funisitis”.4
Both clinical and histopathological definitions of chorioamnionitis have been used as indicators of intrauterine inflammation, but numerous studies have shown these to be poorly correlated. Clinical indicators of maternal inflammation are unspecific and probably mainly identify cases of acute chorioamnionitis. Conversely, histological criteria for chorioamnionitis based upon the identification of polymorphonuclear cellular infiltrates, are clearly defined, although different grading systems exist. It is generally felt that a histological definition of intrauterine inflammation more closely reflects antenatal inflammatory exposure than the clinical definition.5
Exposure to antenatal inflammation has mainly been associated with alterations in brain and lung development. Intrauterine inflammation has quite consistently been shown to adversely affect short term neurological outcome by increasing the incidences of intraventricular haemorrhage, white matter abnormalities, cystic periventricular leucomalacia and cerebral palsy, as reviewed in Dammann et al.6 While several follow-up studies show neurodevelopmental outcome to be unaffected,7–11 others have reported histological chorioamnionitis to be associated with developmental delay,12 13 abnormal neurological outcome,14 speech delay15 and autism.16 As regards pulmonary outcome, Watterberg and colleagues were the first to report a decrease in the incidence of respiratory distress syndrome (RDS), while the incidence of chronic lung injury, marked by the presence of bronchopulmonary dysplasia (BPD), was increased in infants with chorioamnionitis.17 This paradoxical effect of prenatal inflammation on pulmonary outcome has been referred to as the “Watterberg effect”. Numerous larger cohort studies in preterm infants have since tried to reproduce and explain these findings, yielding seemingly inconsistent results. The interpretation of many of these studies is further complicated by the fact that important confounders such as gestational age have not been adjusted for in the analyses.
The purpose of this review is to provide a synopsis of the human evidence on pulmonary outcome after exposure to intrauterine inflammation defined solely on histopathological grounds. Findings of cohort studies will be summarised, with special emphasis on identifying differences and similarities, and exploring potential explanations for paradoxical findings among these studies. Separation of the effects of chorioamnionitis with and without fetal involvement, and the interaction with antenatal steroid administration will receive special attention.
RESPIRATORY OUTCOME AFTER CHORIOAMNIONITIS
In the Watterberg study, 53 mechanically ventilated infants with a birth weight below 2000 g were divided into two groups based on the presence or absence of RDS.17 None of the infants received surfactant or antenatal steroids. The incidence of chorioamnionitis was significantly higher in the group without RDS. Conversely, chorioamnionitis-exposed patients who survived were more likely to develop BPD. Although infants with chorioamnionitis were of significantly lower gestational age, possibly explaining the increased incidence of BPD, the data were not adjusted for this. On the other hand, gestational age adjustment would probably have augmented the decreased RDS risk.
These observations have led many research groups to conduct cohort studies on respiratory outcome in preterm newborns exposed to histological chorioamnionitis. The general characteristics of these studies are summarised in table 1.
Incidences of histological chorioamnionitis varied between 33% and 71%, largely depending on variation in criteria used for inclusion and exclusion. Two studies comprised patients included in randomised controlled trials. One was designed to evaluate the effect of antenatal MgSO4 on the development of cerebral palsy,26 while the other randomised mechanically ventilated infants to either hydrocortisone or placebo to evaluate the effect on BPD development.24 While antenatal MgSO4 was shown not to alter respiratory outcome in preterm infants,33 the hydrocortisone trial should obviously be interpreted with care.
The association of chorioamnionitis with relevant respiratory outcome parameters is shown in table 2.
Chorioamnionitis-exposed patients had either similar7 21 23 25 29 30 or decreased2 3 19 32 RDS incidences in most studies. While Elimian and colleagues reported an increase in RDS incidence, the difference disappeared after multivariate analysis.18 Interpretation of this study is further complicated by the exclusion of patients with clinical chorioamnionitis. Four other large reports adjusted their data for confounding factors, invariably showing chorioamnionitis to be associated with significantly decreased RDS risk.2 3 27 32
Data on the need for respiratory support after chorioamnionitis differ greatly between studies. Often parallel to RDS incidence, chorioamnionitis has been reported to increase18 30 and decrease,19 as well as not to affect the need for surfactant administration.22 Moreover, while some report no effect on the need for mechanical ventilation,19 30 time spent on the ventilator,7 and time on additional oxygen supplementation,7 others report increased need for ventilatory support or oxygen.25 30
The increased incidence of BPD was reproduced in six of the 18 studies.21 25 26 28–30 However, gestational age adjustment was performed in only one of these.30 Curiously, the risk remained although gestational age was significantly lower in chorioamnionitis infants.30 Moreover, two of these studies used the old BPD definition of oxygen need at 28 days postnatally.25 26 In the remaining reports, multivariate adjustment generally showed no difference in BPD risk or BPD-free survival,3 22 24 27 32 while chorioamnionitis even decreased BPD risk in one study.20
Incidental reports suggest that chorioamnionitis may be associated with increased risks for neonatal pneumonia3 and severe pulmonary haemorrhage.34 Additional studies are needed to investigate these potential associations.
RESPIRATORY OUTCOME AFTER FETAL INVOLVEMENT
Fetal signs of inflammation accompanying chorioamnionitis are generally felt to reflect a more serious inflammatory state. Recent evidence suggests that amnionitis may be another marker of severe intrauterine inflammation, although data linking amnionitis to neonatal respiratory outcome are currently lacking.35 Matsuda and colleagues were the first to link severe fetal inflammation to BPD development.36 Several studies have since addressed the question as to whether fetal inflammation may have additional consequences for neonatal outcome. Reported differences in respiratory outcome parameters between chorioamnionitis-exposed patients with and without fetal involvement are shown in table 3.
Fetal inflammation was defined as either chorionic vasculitis,28 umbilical vasculitis,2 funisitis,22 23 26 29 “fetal response”,20 or subdivided into polymorphonuclear leukocyte (PMN) infiltration of the chorionic plate or the umbilical cord.27 Two studies showed that RDS incidence was further decreased in infants with fetal involvement when compared to those with only maternal signs of inflammation,2 23 while no additional effect was seen in another.29 Multivariate analysis invariably confirmed the association between fetal inflammation and decreased RDS incidence,2 27 29 an effect that appears to be additive to that of chorioamnionitis alone.2 None of the studies found fetal inflammation to increase the risk of developing BPD when compared to only maternal inflammation. Also, no overall effect of fetal involvement on BPD risk was seen after adjustment for potential confounders,20 27 although in non-white infants severe fetal involvement was associated with decreased BPD risk in one study.20
Not included in the table is a small case–control study comparing the effects of severe acute chorioamnionitis, severe subacute chorioamnionitis (defined by the presence of additional mononuclear cells) and subacute necrotising funisitis on neonatal outcome.37 Each of these histological states was associated with decreased RDS incidence when compared to matched patients without placental inflammation. Interestingly, BPD incidence was greatly increased only in the subacute chorioamnionitis group.37 This suggests that both the timing and duration of intrauterine exposure to inflammation may modulate its effect on neonatal respiratory outcome. However, the definition of BPD used was not mentioned, complicating interpretation of the data. Moreover, others have found no association between mononuclear infiltrates and neonatal outcome.27
CHORIOAMNIONITIS AND STEROIDS
Antenatal steroids
Although chorioamnionitis is an inflammatory state while steroids have an anti-inflammatory effect, both are capable of enhancing lung maturation, probably partly through distinct mechanisms.38 39 Concerns that maternal administration of corticosteroids would aggravate the alleged harmful response to intrauterine inflammation have initially limited their use in suspected chorioamnionitis. Over recent years, both animal experimental studies and clinical studies have provided support for the use of antenatal steroids in imminent preterm birth with suspected chorioamnionitis. The human evidence is discussed here, while animal experimental evidence has been reviewed recently.38
None of the patients reported in the initial Watterberg study received antenatal steroids.17 It has been suggested that the inability of many later studies to confirm the increased BPD risk, may be attributed to the increased use of antenatal steroids over the last 15 years. Several of the aforementioned cohort studies have explored the effect of antenatal steroids in patients with histological chorioamnionitis to try to address this issue.
In line with their established effects in the overall preterm population, antenatal steroids also seem to decrease RDS incidence in infants with histological chorioamnionitis. Although only Elimian and colleagues found the decrease to be significant,18 a similar trend is clearly present in other reports as well.3 40 These observations are supported by molecular studies showing increased surfactant protein B in amniotic fluid after antenatal steroids in women with intra-amniotic infection.41 In addition, antenatal steroids seem to decrease neonatal mortality3 18 and the incidence of the systemic inflammatory response syndrome (SIRS)40 in chorioamnionitis-exposed infants.
Despite an apparent reduction in RDS, no significant effect of antenatal steroids on BPD incidence has been reported.40 In a logistic regression model to identify risk factors for BPD, Kent and Dahlstrom found neither chorioamnionitis nor antenatal steroids to be significant predictors.22 On the other hand, all cohort studies with documented antenatal steroid exposure rates above 55% have reported either decreased or unchanged incidences of RDS and BPD at 36 weeks post-menstrual age (PMA) after chorioamnionitis (table 1).2 3 20 22 24 27 32 Thus, current high rates of prenatal steroid administration may partly explain why the initial observation of an association between chorioamnionitis and BPD is no longer reproduced. Taken together, these data further support liberal administration of antenatal steroids in case of imminent preterm birth,42 and also when chorioamnionitis is present.
Postnatal steroids
In light of the association between steroid exposure, chorioamnionitis and respiratory outcome, the findings of the hydrocortisone trial are of particular interest. Although hydrocortisone did not improve outcome in the general population, subgroup analysis of infants with chorioamnionitis showed increased BPD-free survival and decreased mortality with postnatal hydrocortisone.24 The effect remained after multivariate analysis and was most prominent in infants with fetal signs of inflammation. Thus, anti-inflammatory treatment may positively affect pulmonary outcome after antenatal exposure to inflammation. However, the particular study was stopped because of an increased incidence of spontaneous gastrointestinal perforations in the treatment group, complicating future exploration of this therapeutic option.
CHORIOAMNIONITIS AND LONG TERM RESPIRATORY OUTCOME
We are aware of only two human studies investigating the association between chorioamnionitis and pulmonary outcome beyond the neonatal period. No significant differences in the use of supplemental oxygen, bronchodilators and systemic or inhaled steroids were reported between patients with and without chorioamnionitis at 18–22 months’ corrected age in the hydrocortisone trial, irrespective of neonatal hydrocortisone treatment.43 A prospective study by Kumar and colleagues was specifically designed to investigate the effect of chorioamnionitis on respiratory outcome in early childhood.44 Chorioamnionitis and prematurity were shown to have a joint predisposing effect on recurrent wheezing and physician-diagnosed asthma at a mean age of 2.2 years. The effect was most prominent in former extremely preterm infants and in African-American children. Chorioamnionitis was defined as the presence of either maternal fever or histological chorioamnionitis, complicating comparison with studies reporting only histological inflammation. Still this study suggests that antenatal inflammation may affect lung development beyond the neonatal period and further investigation of the long term pulmonary effects of antenatal exposure to inflammation is warranted.45
EXPLAINING THE INCONSISTENCIES
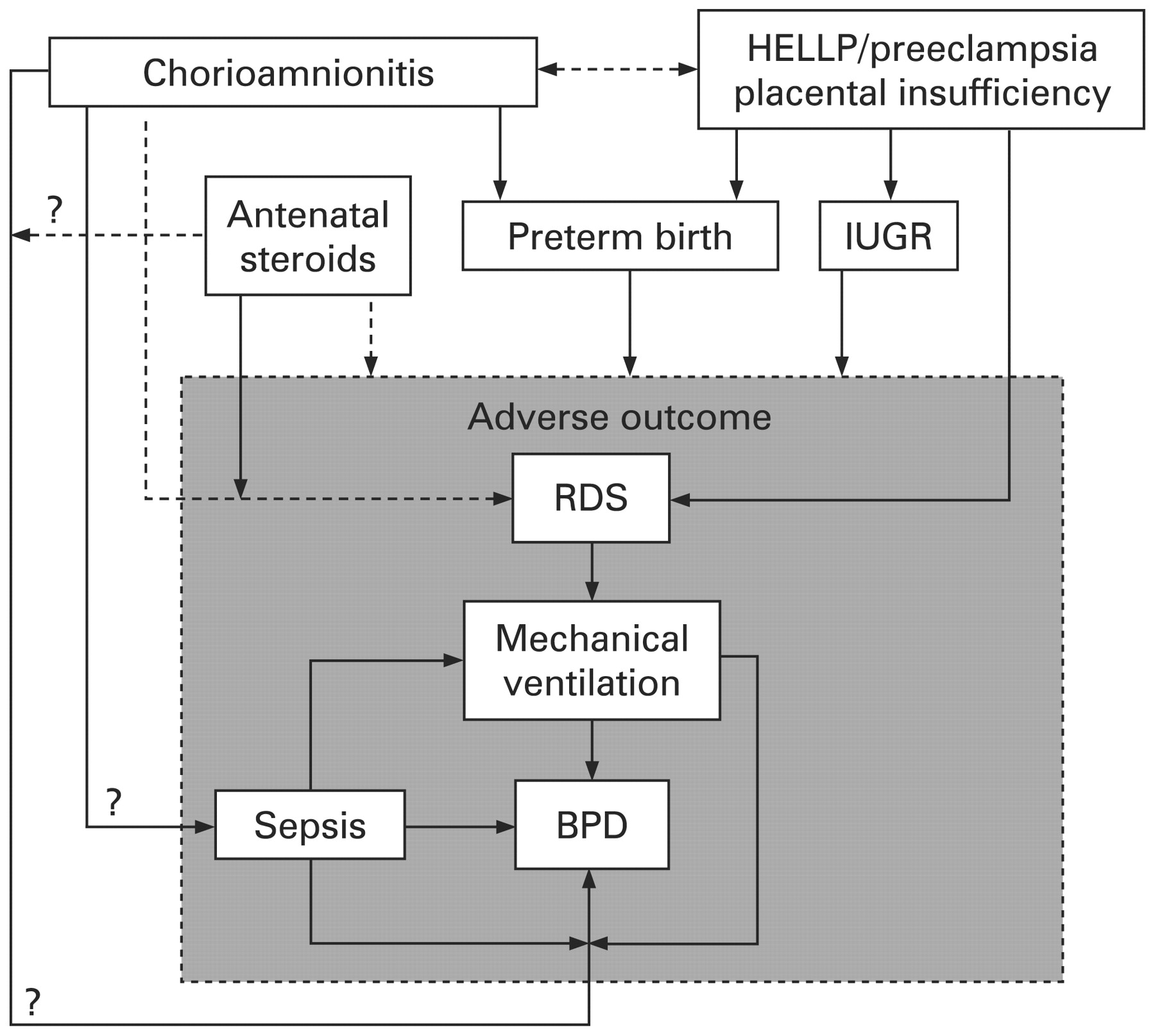
Reported effects of antenatal inflammation on respiratory outcome differ greatly between studies published to date. Figure 1 illustrates how numerous factors complicate interpretation of these associations and may explain at least part of the paradoxical nature of findings among different studies. Their potential contributions are discussed in order to try to explain the apparent inconsistencies.
{kind=link}
Diagram showing positive (––) and negative (– – – –) correlations between clinical entities that complicate interpretation of reported associations between chorioamnionitis and neonatal respiratory outcome. BPD, bronchopulmonary dysplasia; HELLP, haemolysis, elevated liver enzymes and low platelets; IUGR, intrauterine growth retardation; RDS, respiratory distress syndrome.
Inclusion and exclusion criteria
Firstly, inclusion criteria differ greatly between studies. Differences in gestational age and the birth weight distributions of the study groups are likely to affect both adverse respiratory outcome and its association with chorioamnionitis, since the incidence of both is inversely related to gestational age (fig 1). Some studies further selected their cohort by including only ventilated infants,17 24 or patients with premature prolonged rupture of membranes (PPROM),7 preterm labour,7 26 29 36 and suspected clinical chorioamnionitis.29 36 In contrast, cases of clinical chorioamnionitis or suspected maternal infection were excluded by others.18 26 The resultant plausible exclusion of more seriously affected chorioamnionitis infants46 may underestimate the effect of chorioamnionitis on RDS reduction, since fetal inflammation has been shown to be associated with a more prominent reduction in RDS than maternal inflammation alone.2 On the other hand, inclusion of mothers based on the presence of preterm labour will preselect mainly patients with histological chorioamnionitis, largely excluding the group of indicated preterm delivery consisting primarily of mothers with preeclampsia, HELLP syndrome (haemolysis, elevated liver enzymes and low platelets) and vaginal bleeding. This too is importance since these entities have been associated with increased RDS incidence (fig 1).47–50 Excluding these patients may thus underestimate the association between chorioamnionitis and RDS reduction and explain why studies doing so have failed to identify this association.7 29
The fact that preeclampsia and HELLP syndrome are associated with increased RDS incidence raises another fundamental question. Since these entities and chorioamnionitis rarely co-exist, their high incidence in the reference group is an important confounder when assessing the effect of chorioamnionitis on respiratory outcome. It raises the question as to whether the decrease in RDS incidence seen after chorioamnionitis may in fact reflect an increased risk in patients exposed to preeclampsia or HELLP syndrome. The notion that markers of lung maturation are decreased in patients with HELLP syndrome,51 while animal studies invariably confirm the lung maturational effects of antenatal inflammation,38 52 suggests that the effect is bidirectional.
Disease definitions
Various histopathological criteria and grading systems for diagnosing chorioamnionitis or fetal inflammation exist and likewise, differ importantly between studies. Furthermore, the old definition of BPD used by some complicates comparison of this outcome parameter between studies.25 26 Since the incidence of BPD defined as oxygen need at 28 days postnatally is more closely related to gestational age than is the more suitable definition of BPD at 36 weeks postconceptional age (PCA), the use of the former may account for the increased BPD incidence in the chorioamnionitis group through their lower gestational age in these studies.25 26
Confounding factors and covariates
Since both chorioamnionitis and adverse neonatal outcome are inversely related to gestational age, adjusting for gestational age differences when exploring associations between the two is invaluable. Only a limited number of studies have appreciated this and performed multivariate adjustment to account for this effect.2 3 20 22 27 29 30 32 Although additional inclusion of other confounding factors in multivariate models may have increased the relevance of the findings in individual studies,2 3 20 22 27 29 it further complicates comparison of the data between them, as does the lack of mentioning the factors included in the model.18 Although the fact that gestational age in itself is dependent on many additional confounding factors somewhat limits the accuracy of its use in multivariate models,53 the magnitude of its confounding nature justifies its use as such.
Racial differences in chorioamnionitis prevalence and the pulmonary response to intrauterine inflammation may account for additional inconsistencies between studies. Chorioamnionitis and vaginal bacterial colonisation are more prevalent in non-white infants,20 54 55 while white race is a risk factor for BPD.20 56 Redline and colleagues showed that in non-white infants, chorioamnionitis was associated with decreased BPD incidence, most prominently in infants still ventilated on day 2.20 Conversely, black race augmented the increased risk of wheezing and asthma after chorioamnionitis in a follow-up study.44 Other important potential confounding variables have been shown to differ importantly between white and black mothers and complicate interpretation of the association between race, chorioamnionitis prevalence and neonatal outcome.20 55
Over the time period the cohort study data have been collected, important changes in general practice in neonatal intensive care have taken place. The widespread implementation of antenatal steroids is the most obvious and probably the most influential example.42 Other practice changes include the increased use of exogenous surfactant57 and non-invasive modes of ventilatory support such as continuous positive airway pressure (CPAP).58 These may reduce secondary lung injury in chorioamnionitis-exposed infants and partly account for the apparently diminishing association between chorioamnionitis and BPD over time.59
EXPLORING THE MECHANISMS
Sufficient evidence links chorioamnionitis to altered lung maturation and development. In animals, antenatal inflammation clearly enhances lung maturation.38 52 The effect has been shown to be much greater than that of antenatal steroids, suggesting that at least partly distinct mechanisms play a role.39 60 On the other hand, normal lung development is disrupted and architectural changes resemble the pathological picture of new BPD currently seen in preterm infants.38 61–63 Both inflammatory mediators and growth factors have been shown to play a role in this process.38 64 65
As for human data two levels of mechanistic evidence may be considered: indirect data, investigating associations between covariables and the effect of chorioamnionitis on respiratory outcome, and direct data, investigating effects of chorioamnionitis on a functional, molecular or cellular level.
Indirect mechanistic evidence
Probably the most informative study concerning indirect mechanistic evidence is that reported by Van Marter and colleagues.59 In a case–control design, very low birthweight infants with BPD were matched with infants without BPD on gestational age, birth weight and hospital specific treatment strategies. In these infants chorioamnionitis was associated with a decreased risk for BPD if infants were ventilated for less than 7 days. However, when infants were exposed to mechanical ventilation for more than 7 days or had sepsis, chorioamnionitis significantly increased BPD risk, the effect being most prominent in infants with all three risk factors present (fig 1). This suggests that, while antenatal exposure to inflammation in itself may reduce BPD risk, it increases the susceptibility of the lung to postnatal injurious events. This too may explain part of the Watterberg effect on BPD, since only ventilated children were included in their initial study.17 Interestingly, in the Watterberg study mean airway pressures needed to ventilate infants were lower initially in those exposed to chorioamnionitis but rose above values for non-exposed infants over the second week.17 This too is indicative of worsening pulmonary status during mechanical ventilation despite an apparently healthier initial condition.
Pointing in the same direction is the simple observation that chorioamnionitis probably lowers RDS risk without consistently affecting BPD incidence. In other words, given the better initial respiratory status reasonably requiring less invasive intervention, one would expect BPD risk to diminish as well, since invasive interventional strategies are clearly associated with BPD development.66 The notion that this does not happen further supports the concept of increased susceptibility of the developing lung to secondary hits in the neonatal period following intrauterine exposure to inflammation.67
Direct mechanistic evidence
Not surprisingly, many studies have reported increased levels of pro-inflammatory cytokines, chemokines and other markers of inflammation in cord blood, fetal placental capillaries and lung-derived specimens in patients with histological evidence of intrauterine inflammation.14 17 26 32 36 68–72 Chorioamnionitis and funisitis have also been associated with increased numbers of macrophages and lymphocytes in the lung.73–75 Moreover, both maternal and fetal polymorphisms of immunoregulatory genes have been associated with both histological chorioamnionitis76–82 and neonatal sepsis,77 while no association with neonatal pulmonary outcome was found.77
A considerable body of evidence links Ureaplasma urealyticum to chorioamnionitis, preterm birth and the development of chronic lung disease,83 84 as reviewed elsewhere.85 86 Awareness of the role of Ureaplasma species is invaluable, since its in vitro cultivation needs specific and complex nutritional requirements and regular culture techniques will often miss the organism. Molecular techniques may improve the detection of chorioamnionitis-associated pathogens including Ureaplasma.87 88 The ability of Ureaplasma species to induce both lung maturation and injury has been confirmed in animal models.89 90 However, antibiotic treatment aimed at eradicating Ureaplasma does not seem to improve respiratory outcome in preterm infants.91 Worryingly, in women in threatened preterm labour antibiotic treatment is associated with an increased risk of cerebral palsy.92 No difference in outcome is seen in a similar trial in women with PPROM.93
In preterm infants not exposed to antenatal steroids, Watterberg and colleagues showed that chorioamnionitis was associated with increased serum cortisol levels.94 Since corticoids are known stimulants of surfactant synthesis and lung maturation, this could partly account for the reduction in respiratory distress in these infants,94 although animal data do not support this concept.39
In a pathological study in stillborn fetuses, those with chorioamnionitis had decreased pulmonary expression of serum and glucocorticoid-inducible kinase (SGK1), a known regulator of epithelial Na+ channel (EnaC) and Na+-K+-ATPase.73 The authors suggest that this may decrease pulmonary fluid clearance and consequently affect gas exchange, predisposing infants to increased ventilatory support. The same group showed that proliferation of epithelial cells, endothelial cells and fibroblasts was decreased while apoptosis of distal lung epithelial cells was increased in fetuses with chorioamnionitis.95 This provides a potential human link between chorioamnionitis and adverse lung development. Matrix metalloproteinase-8 and -9, neutrophil products capable of cleaving important matrix components, may also play a role in this process. Increased levels in cord blood and lung-derived fluid have been linked to both chorioamnionitis32 96 97 and the development of BPD.97–101 Taken together, human studies on mechanistic evidence are scarce when compared to animal experimental studies. Additional human data are indispensable in exploring the underlying mechanisms of pulmonary developmental changes after chorioamnionitis.
CONCLUSION
Evidence is increasing that intrauterine inflammation decreases RDS risk in preterm infants through stimulation of lung maturation. Despite a reduction in RDS, the incidence of BPD is unchanged, while recent data suggest the susceptibility for subsequent asthma development to be increased. Both altered lung development and enhanced susceptibility to secondary injury may account for this effect. Antenatal steroids further decrease the incidence of RDS and possibly also that of BPD in chorioamnionitis-exposed infants.
Although current treatment strategies seem to diminish the adverse effects chorioamnionitis has on neonatal outcome in preterm infants, its impact on adverse outcome obviously remains substantial through its causal relationship with preterm birth itself. Future research should focus on the mechanisms of inflammation-induced lung injury, long term follow-up of pulmonary outcome after chorioamnionitis and ways to reduce its adverse effects on lung development and injury repair.
REFERENCES
Footnotes
Funding: Jasper Been is funded by a “Profileringsfonds” grant from the Maastricht University Medical Centre.
Competing interests: None.