Article Text

Abstract
Background: Superior vena cava (SVC) flow assesses blood flow from the upper body, and may provide a reliable assessment of systemic blood flow.
Aim: (i) To assess the relationship between SVC flow in first 24 h and adverse outcome in very low birthweight (VLBW) infants (ii) To assess correlation between SVC flow and left and right ventricular outputs and anterior cerebral artery (ACA) velocity measurements.
Methods: A prospective, observational cohort study. Neonates with birthweight <1500 g were eligible and those with congenital heart disease (excluding patent ductus arteriosus) or major congenital malformations were excluded. Echocardiographic evaluation of SVC flow, right and left ventricular outputs and ductal patency was done in the first 24 h of life. Capillary refill time, blood pressure and urine output were also measured simultaneously. The primary outcome was intraventricular haemorrhage (IVH) grade ⩾ II and/or early neonatal death (<7 days).
Results: 40 VLBW neonates were enrolled following parental consent. Two were excluded. 8 babies (21%) had low flow states. There was no difference between the cohorts in median birth weight (1.14 kg vs 1.17 kg; p = 0.76), gestational age (26.5 vs 28.0 weeks, respectively; p = 0.12) or hours of life at examination (18.5 h vs 21 h, respectively; p = 0.36). The incidence of primary outcome (IVH ⩾ grade II and/or early neonatal death) was 50% and 6.7%, respectively (p = 0.01). There was no correlation between SVC flow and right ventricular outputs and ACA velocity and blood pressure measurements.
Conclusions: 21% of our VLBW infants had low SVC flow in the first 24 h, and this was associated with early neonatal death and/or severe IVH.
Statistics from Altmetric.com
The diagnosis and management of circulatory compromise in the very low birthweight infant remains controversial.1 Many practitioners continue to rely on absolute blood pressure values to guide intervention.2 This is an inaccurate approach as evidenced by the large number of “normative” blood pressure ranges, the marked variation in the incidence of hypotension,3 and the even greater variation in those receiving treatment.4 End-organ perfusion is determined by a combination of perfusion pressure and vascular resistance, and reliance on absolute blood pressure values may result in inappropriate therapeutic intervention. More reliable methods of detecting end-organ blood flow would help identify patients for whom intervention may be appropriate.
Clinical evaluation at the bedside might provide more information than absolute blood pressure values alone. Concerns surrounding clinical assessment include lack of objectivity, relative importance or lack thereof of individual parameters assessed, lack of normative values and their reproducibility. We have previously shown that the inclusion of clinical parameters and blood pressure values in the management of hypotension reduced the number of infants treated with volume, inotropes and corticosteroids, and resulted in a similar short-term outcome.5
Functional echocardiography is a growing area of interest in the management of the preterm transitional circulation. It can provide objective evaluation of cardiac function and output, identify a significant patent ductus arteriosus and allow evaluation of therapeutic interventions.6 It has recently been used to measure vena cava blood (SVC) flow, of which approximately 80% is estimated to be venous return from the brain. The SVC fulfils the criteria for Doppler assessment, and a normal range has been produced and the technique has been shown to be reproducible. SVC blood flow has been previously associated with adverse short-term outcome.7 However the positive predictive value for estimating adverse outcome remains low, estimated to be of the order of 30%. Some studies have shown an association between low SVC flow measurements and adverse outcome.8 Numerous studies have shown an association between hypotension and adverse outcome.9 10
The present study aimed to assess the relationship between low SVC flow states and adverse outcome, defined as intraventricular haemorrhage (IVH) grade ⩾II and/or early neonatal death. A secondary objective was to assess the relationship between SVC flow and measures of cardiac output (right ventricular and left ventricular output) and end-organ perfusion (anterior cerebral artery (ACA) velocity parameters).
METHODS
We conducted a prospective, cohort observational study at a level III neonatal intensive care unit (Coombe Women’s Hospital, Dublin, Ireland) between November 2006 and June 2007. We included newborns with very low birth weight (<1500 g) who were admitted to neonatal intensive care unit in the first day of life. Parental consent was obtained. Newborns with congenital heart disease (except patent ductus arteriosus, non-complicated atrial septal defect and non-complicated muscular ventricular septal defect (VSD)) or major congenital malformations were excluded. This study was approved by the research ethics committee of the hospital. Low SVC flow on day 1 was defined as flow less than 40 ml/kg/min.
Ultrasound studies
All the neonates underwent echocardiography on day 1 together with cranial ultrasound. Cranial ultrasound was repeated between day 7 and day 14 of life and before discharge.
Echocardiographic data collection
We used Philips HD11XE ultrasound scanner with curved array transducer (5–8 MHz) incorporating colour flow and pulsed wave Doppler with adaptive Doppler technology. The scan was recorded on the hard disk of the ultrasound machine and measurements made at a later stage. Structural normality of the heart was established and the following measurements were taken, using protocols described in the literature.
SVC flow—using the method described by Kluckow et al.11 The mean velocity of blood flow was calculated from the integral of the Doppler velocity tracings and was averaged from five consecutive cardiac cycles. Diameter measurements were averaged from three cardiac cycles. The SVC flow was calculated using the formula:

Left and right ventricular output using the method described previously in the literature.12 The mean velocity of blood flow was calculated from the integral of the Doppler velocity tracings and was averaged from five consecutive cardiac cycles. Diameter measurements were averaged from three cardiac cycles.
Assessment (including the diameter) of patent ductus arteriosus.13
SVC flow and the left ventricular and right ventricular outputs were expressed in ml/kg/min.
Cranial ultrasound
We used a 7.5 MHz transducer for the cranial ultrasound, which was done after the echocardiographic exam on day 1 and any IVH was noted and classified according to Papile grading.14 The following velocity parameters were studied on day 1: peak systolic velocity, end-diastolic velocity, mean velocity and resistance index. All parameters were measured in the left ACA. Cranial scanning was repeated on day 7–14 without velocity measurements and then again prior to discharge.
Clinical and physiological data
Ventilatory support, surfactant treatment, blood pressure values (systolic, diastolic and mean) either invasive (peripheral or umbilical artery) or non-invasive (pressure cuff—Critikon soft-cuff sizes 1–4) and blood pressure support were recorded at the time of the scan. Arterial blood gas values were obtained prior to ultrasound examination. Urine output (ml/kg/h) from birth to scan time was calculated. Capillary refill time was assessed in three locations (forehead, mid-sternum and big toe) by a person unaware of other measured variables prior to the scan. This measurement was obtained by a standardised technique (mild pressure applied for 5 s and then released, duration of time for return of colour was obtained by stopwatch in 1/10 s).
We used a combination of blood pressure values, urine output, clinical assessment and biochemical parameters to determine the need for circulatory support. Management of hypotension included volume expansion (normal saline 10 ml/kg), followed by epinephrine (0.05–0.5 μg/kg/min) and/or dobutamine at doses up to 20 μg/kg/min. Hydrocortisone was added if there was no response to the above measures. We did not aim to investigate the response of blood flow to any type of blood pressure support agent used. Patent ductus arteriosus was treated when the diameter was more than 2 mm with left-to-right shunting on day 1 of life, and ibuprofen (10 mg/kg on day 1, 5 mg/kg day 2 and 3) was administered.
Statistical analyses
We analysed the data using a PC-based statistics package (StatsDirect version 2.6.1) using Fisher exact test, Mann–Whitney U test and Pearson correlation. p<0.05 was considered significant.
RESULTS
Between November 2006 and June 2007, 45 very low birthweight neonates were admitted to the neonatal intensive care unit. Consent was not obtained in five cases (investigator not available in all cases). Echocardiography was performed on 40 neonates. Two neonates were subsequently excluded (one had trisomy 21 and muscular VSD and a second had a large perimembranous VSD). The mean (SD) birth weight was 1.08 (0.28) kg, mean gestational age was 27.82 (2.14) weeks’ gestation and the mean hour of life at echocardiography was 19.05 (4.93) h. The cohorts were 68% female, and 95% of neonates received at least one dose of corticosteroids prior to delivery. In the first 24 h of life, 1% received surfactant (Poractant Alfa, Chiesi Pharmaceuticals, Parma, Italy), and 45% remained ventilated at the time of the study. Eight neonates (21%) had low SVC flow (defined as a flow less than 40 ml/kg/min) at the time of assessment.
There were no differences in perinatal variables in the low-flow group compared with those with normal flow (table 1). There was a trend towards more ventilatory support among infants with low SVC flow. Inotropes were being given to 50% of the low SVC flow group at the time of the study and only 3% from normal SVC flow group.
Outcome
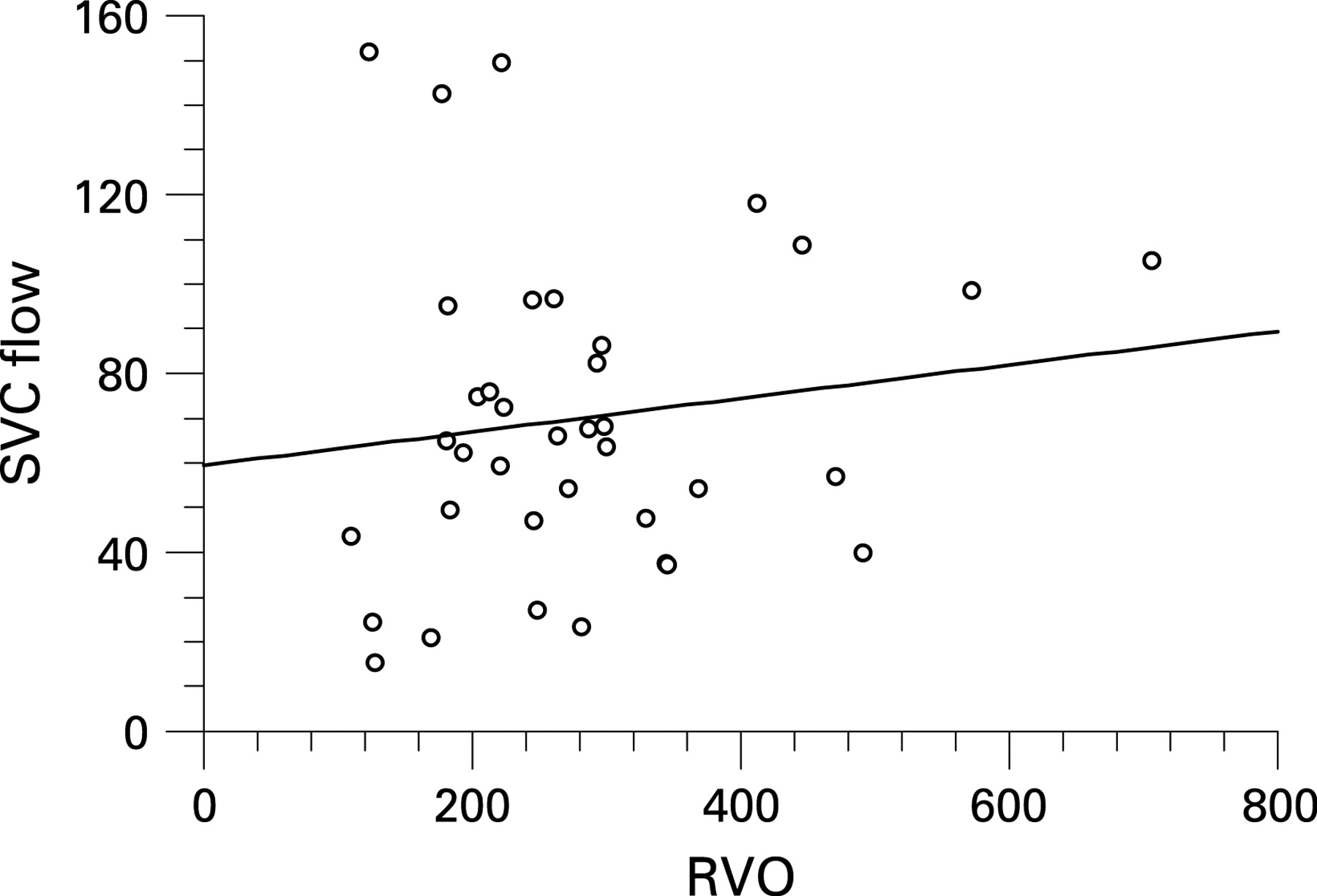
The incidence of our combined primary outcome (early neonatal death or severe early IVH—grade II or more) was 50% in the low SVC flow group and 6.7% in the normal SVC flow group (p = 0.012; odds ratio (OR) 14; 95% CI 1.3 to 182.3). Sensitivity of the SVC flow as a predictor for early neonatal death or severe IVH was 66.7%, and specificity was 87.5%. The two groups did not differ significantly in left ventricular output or right ventricular output. There was no significant difference in mean velocity in the ACA (table 2). There was a poor correlation between SVC flow and left and right ventricular output, as shown in figs 1 and 2. Incidence of patent ductus arteriosus at the time of echocardiography was 100% in the low SVC flow group and 83% in the normal SVC flow group (p = 0.56). There was a tendency towards higher incidence of severe IVH in the low right ventricular output (<150 ml/kg/min) group (table 3). However the sensitivity of low right ventricular output was only 33.3%.


{kind=link}
{kind=link}
Clinical assessment is highlighted in table 4. A capillary refill time of >4 s measured in the foot, combined with a low SVC flow measurement, predicted adverse outcome in 100% of neonates. The sensitivity of this combined measure was 66.7% and the specificity was 100%.
DISCUSSION
What is already known on this topic
Previous studies have identified an association between low superior vena cava blood flow and adverse outcome.
What this study adds
This study supports the association between low superior vena cava blood flow and adverse outcome.
Functional echocardiography combined with clinical parameters may identify neonates who truly have impaired end-organ perfusion and allow targeted therapy.
We found an incidence of 21% of low SVC flow states in this cohort of infants. This is similar to a recent study assessing the effectiveness of prophylactic milrinone for prevention of low flow states.15 We have shown that low SVC flow in the first 24 h of life in the very low birthweight infant is associated with adverse outcome (death or grade 2 or more IVH). Other echocardiographic measures of flow correlated poorly with short-term outcome, as did mean blood pressure values. SVC flow correlated poorly with the right and left ventricular outputs and blood pressure measurements. This is not surprising as left ventricular output is influenced by shunting via the ductus arteriosus (the majority of infants in this study had a patent ductus arteriosus on initial scan with left-to-right shunting), the right ventricular output is influenced by shunting via the patent foramen ovale and mean blood pressure values are a poor surrogate marker of end-organ blood flow.
However, despite the poor relationship between blood pressure values and end-organ perfusion, it still remains the primary reason for many clinicians to intervene.2 This is because there seems to be an association between lower blood pressure values and cerebral injury in preterm infants. However this association is far from consistent, and it is not possible from the published literature to define a threshold below which there is a markedly raised risk of cerebral injury.16 There does seem to be a consistent association between low SVC flow and adverse outcome,17 however, the positive predictive value for adverse outcome remains low. Using this criterion alone would mean that a large proportion of infants would be treated, for whom intervention may be inappropriate. This is important considering the major concerns surrounding therapeutic strategies and possible adverse effects.18 19
We have highlighted the association between low SVC flow and adverse outcome. However, low SVC flow values in isolation again poorly predicted those at risk of IVH. The inclusion of other parameters may help identify patients who may benefit from therapeutic interventions. We assessed capillary refill time in three different sites, mean blood pressure values and urine output. We identified prolonged capillary refill time in the foot (defined as greater than 4 s) as an important indicator of systemic perfusion. The inclusion of this parameter in conjunction with a low SVC flow improved the sensitivity, specificity and positive predictive value (100%) for predicting adverse outcome. Conflicting evidence exists in relation to the role of capillary refill times in assessing end-organ blood flow in the neonate.20 21 Values exist for the term neonate but there are limited data on capillary refill times in the preterm. Wodey et al have shown a significant relationship between cardiac index and capillary refill time in preterm neonates, albeit in those with a closed patent ductus arteriosus.22 Almost all patients in our cohort had a patent ductus arteriosus in the first 24 h of life. We could not identify any relationship between SVC flow and ACA measurements or any association between ACA measurements and IVH. There is conflicting evidence from previous studies on the role of cerebral Doppler in identifying impaired cerebral autoregulation and resultant abnormal cranial ultrasound findings.23–25
There are some limitations to our study. It is possible that we may have underestimated the incidence of low flow states as we performed one echo evaluation in the first 24 h and the timing of our scan was at a median of 18 h. Previous studies having documented changes temporally over the first 48 h of life. We may have identified a higher percentage if the examination was performed at an earlier time point in some cases. Although the present study had a small total number of neonates, the sample did include over 90% of all very low birthweight infants admitted to the intensive care unit during the study period. The remaining 10% who were not included had a normal short-term outcome.
Future studies assessing the effectiveness of interventions for circulatory compromise should focus on subgroups of patients who truly have impaired end-organ perfusion. This study highlights the association between low SVC flow and adverse outcome. It also highlights the possible role of clinical assessment in conjunction with functional echocardiography in the management of the preterm transitional circulation. The inclusion of clinical signs, in this case a prolonged capillary refill time (>4 s) in the foot, in conjunction with functional echo measurements could probably help to identify patients for whom therapeutic intervention is warranted and thereby target those patients who may benefit from intervention.
REFERENCES
Footnotes
Competing interests: None.
Ethics approval: This study was approved by the research ethics committee of the hospital.
Patient consent: Parental consent obtained.