Article Text

Abstract
Objectives: To monitor preterm infants in a cot and a car seat and compare an observed car seat trial with polysomnography (PSG).
Design: Non-randomised controlled trial.
Setting: Regional neonatal unit.
Patients: Preterm infants before discharge.
Interventions: Nap PSG respiratory and sleep variables were measured including gastro-oesophageal pH. Nurse observations included respiratory distress, apnoea measured by apnoea alarm, oxygen saturation and heart rate. Infants were studied supine in a cot and then in a car seat. Nursing observations were compared with PSG during the car seat trial only. Criteria for failure of the PSG and observed tests were predefined.
Main outcome measures: Difference in respiratory instability between cot and car seat. Concurrence regarding failure of the car seat trial between nurse-observed data and PSG.
Results: 20 infants (median gestation 33 weeks (range 28–35 weeks; median postmenstrual age (PMA) at study 36.5 weeks (range 35–38 weeks)) were studied. There were sufficient car seat data on 18 infants for comparison. There were fewer central apnoeas and arousals in the cot than the car seat (p = 0.047 and p = 0.024, respectively). Airway obstruction was not more common in the car seat. Younger PMA at time of study predicted failure in both car seat (p = 0.022) and cot (p = 0.022). The nurse-observed test had low sensitivity for predicting PSG failure but more accurately predicted airway obstruction on PSG.
Conclusions: Immature infants exhibit respiratory instability in cots and car seats. A car seat test does not accurately detect all adverse events during sleep in the seat.
Statistics from Altmetric.com
Since concerns were first raised about the vulnerability of preterm infants during transportation,1 2 several studies have attempted to quantify the respiratory compromise experienced by these infants while in car seats.3–13 Many of these studies had methodological limitations as not all measured the sleep state, or used a supine position for comparison or airflow measures to detect obstructive apnoea, or allowed for differences in postmenstrual age (PMA) at study.
Although car seat trial before discharge has been incorporated into many neonatal discharge practices it has not been universally accepted as the gold standard test for assessing risk of respiratory compromise in a car seat after discharge.14–16 Despite many neonatal nurseries implementing variations of the practice,14 criteria defining how premature infants should be monitored, how long to monitor or what constitutes failure of the test are lacking.15 17 18 Neonatal unit car seat testing programmes therefore vary in equipment type, quality, time and outcome data.14
The present study aimed to examine respiratory variables during active and quiet sleep in preterm infants ready for discharge and compare variables recorded supine in a cot with those recorded supine in a car seat, in particular, to determine whether more obstructive events occurred after transfer to the car seat. A second aim was to compare car seat testing before discharge with concurrent polysomnography (PSG) recording to determine if a nurse-observed test was a sensitive enough predictor of respiratory instability, and in particular airway obstruction, found on PSG.
METHODS
Infants
Eligible infants were born ⩾24 and ⩽36 weeks’ gestation, ready for discharge with a parent-provided car seat meeting the Australian and New Zealand safety standard AS/NZS 1754. We excluded infants with congenital abnormalities interfering with cardiorespiratory function, oxygen requirement at discharge and apnoea beyond 35 weeks postmenstrual age (PMA). Oral caffeine and cardiorespiratory monitoring were discontinued on all infants. Infants routinely slept supine according to nursery policy. Gestational age was determined from maternal dates if certain, or ultrasound at 18 weeks. Demographic and perinatal outcome variables were collated from the medical record.
Study protocol
We studied the infants within 1–2 days of discharge, following feeding, supine in a cot, for at least two sleep cycles, and then transferred to the car seat. Maximum time in the car seat was 2 h. The infant was not fed again before transfer to the car seat to comply with unit policy. A neonatal nurse (LR) monitored the infant while in the seat and a paediatric sleep technician (DS) monitored the PSG recording. Criteria were predefined for terminating the car seat study for patient safety.
Nursing observation and monitoring
Nursing observations were: monitoring of heart rate and oxygen saturation by pulse oximeter (Ohmeda Biox 3740 pulse oximeter, Ohmeda, USA) and apnoea by alarm (Graseby MR10 Neonatal respiration monitor, SIMS Graseby Ltd, UK). The apnoea alarm with abdominal sensor was set to alarm for apnoea ⩾20 s. Respiratory rate, distress and effort were also documented.
Polysomnography
PSG data were obtained using the P series Plus Sleep system (Compumedics P/L, Melbourne, Australia) and the following were recorded simultaneously: electroencephalogram (EEG) (C4/A1, C3/A2 gold cup electrodes, Grass Technologies, West Warwick RI, USA), electrooculogram (EOG), diaphragmatic effort (electromyography (EMG)), nasal pressure (nasal prongs attached to a pressure transducer), nasal airflow (thermistor, Compumedics P/L Melbourne Australia), chest and abdominal effort (piezo bands, Sleepmate, Virginia USA), Spo2 (pulse oximetry oxygen saturation measured at 1 sample/s—Nonin sensor attached to built-in oximeter in the Compumedics P series Plus sleep system) ECG and lower oesophageal pH (Synectics Medical, Stockholm, Sweden). The pH sensor was inserted orally to a distance calculated by the formula (body length ×0.252) +5 cm and then withdrawn 2 cm to rest in the lower oesophagus. We did not confirm the sensor position with x rays.
Data analysis
We carried out the sleep study analysis with Profusion PSG software (Compumedics P/L Australia). Sleep state was manually scored using behavioural observations and EEG, EOG and EMG channels.19 Each epoch was scored as awake, quiet sleep or active sleep. Time in each sleep state was expressed as a percentage of total sleep time. The attending technician scored arousal from sleep based on observation of behaviour (excessive body movements >10 s and/or eyes open and/or crying).20 An arousal index was calculated as the total number of arousals/h of sleep.
We defined apnoea as cessation of nasal/oral airflow for ⩾5 s and classified it as:
obstructive—if respiratory effort continued;
central—if no respiratory effort;
mixed—if a combination of obstructive and central.
We included all apnoeas fitting the length criteria, even those without associated oxygen desaturation or an arousal. Apnoeas <5 s were included if associated with a ⩾2% oxygen desaturation. Apnoea indexes were calculated as the number of events per hour of sleep.
We defined bradycardia as a decrease in heart rate to 70% of immediately preceding baseline levels. Gastro-oesophageal reflux was defined as a pH <4 for ⩾5 s. Total periods of reflux for the each sleep period were counted as completed minutes. A reflux index was calculated as the percentage of total sleep time with a pH <4,21 and an index >10% was considered significant. The Compumedics analysis software determined the number of events in each sleep stage and position. Parents gave informed written consent and the Wellington Ethics Committee approved the study.
Criteria for termination of the study
Criteria for termination of the car seat trial by nursing observations were:
recurrent oxygen desaturation to <90% associated with respiratory distress;
apnoea >20 s in length;
observation of respiratory distress or airway compromise even in the absence of desaturation.
The presence of any one factor was considered a study failure. Failure of the car seat trial by PSG criteria was retrospective and was indicated by:
recurrent oxygen desaturation below 90% over a 5-min period associated with obstruction;
apnoea >20 s of any type or desaturation below 80%.
Statistical analysis
Descriptive statistics are presented as mean (SD) or median and interquartile range, depending on the normality of the data. Data were compared using paired t tests. Data were log-transformed when the distribution was not normal. For analysis of reflux index data +1 was added to the data figure prior to log-transformation as some values were 0. For assessing risk for failure of the PSG study in the cot or car seat the Wilcoxon rank sum test and unpaired t tests were used. p Values <0.05 were considered statistically significant. The sensitivity, specificity, positive predictive value and negative predictive value and 95% CI were calculated for the utility of the nurse-observed test to predict failure of the PSG test and the finding of increased obstruction on PSG.
RESULTS
Group data
In all, 20 infants (10 boys; median gestation at birth 33 weeks (range 28–35 weeks); median birth weight 1877.5 g (range 1300–2490 g); median PMA at time of study 36.5 weeks (range 35–38 weeks)) were consecutively enrolled in the study. Two infants were ventilated (1 day only) and nine had received oxygen (median 0 days, range 1–8). Two infants were excluded because of insufficient data on sleep in the car seat for comparative analysis with hunger as the reason for not settling. Of the remaining 18 infants, one did not settle in the car seat until after the angle of the seat was changed from 60° to 45°. As the infant slept only a little before seat adjustment, the PSG recording after adjustment was used for analysis. Another infant slept for only 17 min in the car seat but as the study was stopped by the nurse for failure of the car seat trial this infant was included.
Comparison between cot and car seat sleep periods
As we could not obtain data on quiet sleep in the car seat for three infants comparisons were made in active sleep only. Table 1 gives the main respiratory variables and oesophageal reflux data that were assessed. We found differences between the groups only with regard to total sleep time, central apnoea and the arousal index, all of which significantly decreased in the car seat (see table 1 for p values).
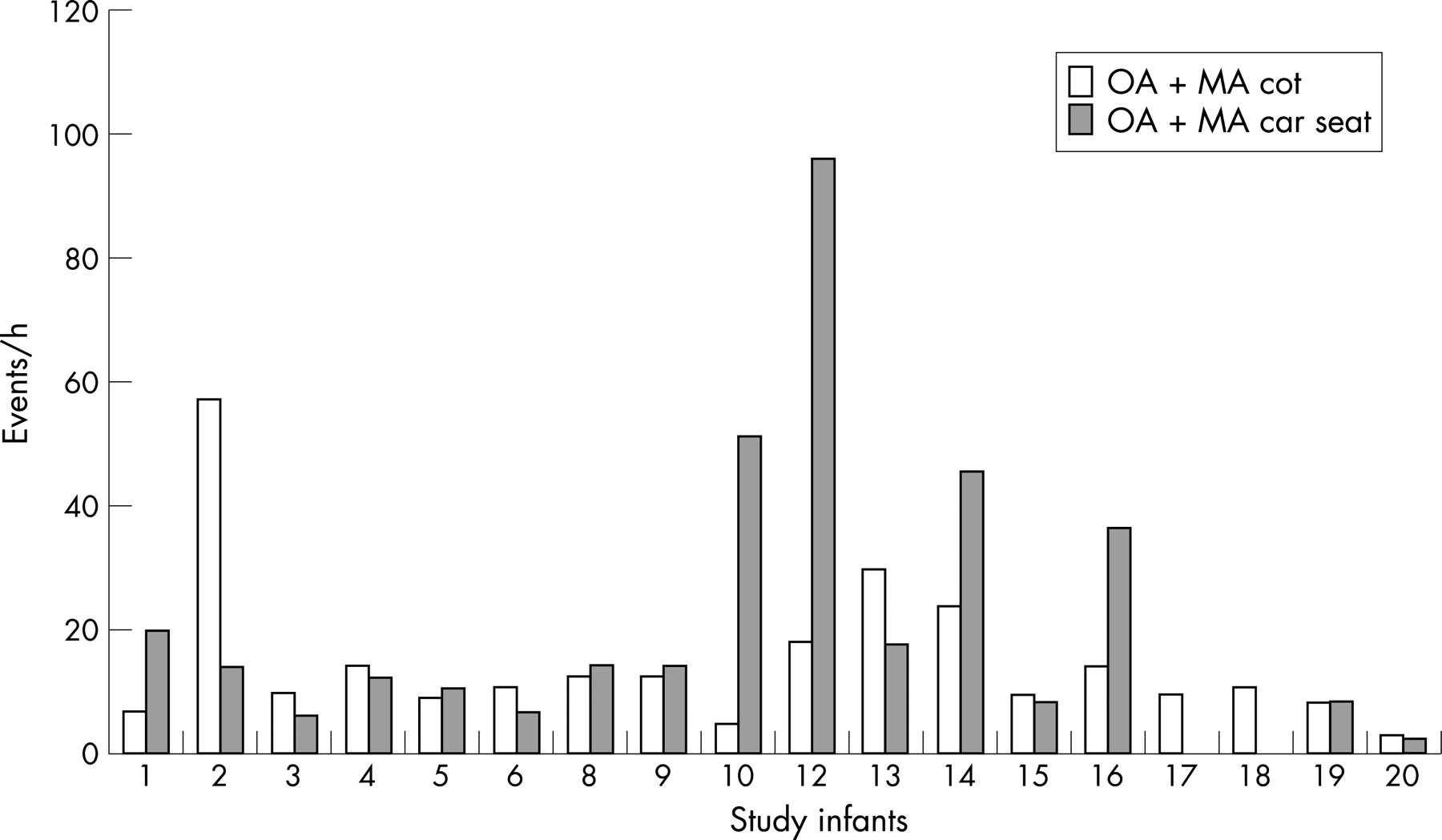
Measures of obstruction
We calculated total obstruction adding the obstructive and mixed apnoea indices. We considered the increase in obstruction to be appreciable if the combined index of obstructive and mixed apnoea in the car seat was above the cot index by an amount that was at least 20% of the baseline value. Eight infants had increases in total obstruction after transfer to the car seat and for five the increase was considered appreciable. Figure 1 shows the findings for individual infants.

{kind=link}
Oesophageal pH
Oesophageal pH recordings were available for 16 infants. The reflux index was greater than 10% for eight infants during the cot period and six infants during the car seat period. Only three infants had an increase in reflux index in the car seat, and this was marked for only two infants.
Oxygen desaturation recorded by PSG
Oxygen desaturation was assessed in completed minutes of time. When a cut-off for desaturation to <90% was considered, eight recordings showed prolonged desaturation—five in the cot period and three in the car seat period. Oxygen desaturation to <85% was documented for 1–2 min of the study period in three infants only, two while in the cot and one while in the car seat.
Predefined PSG failure criteria
Five infants met PSG criteria for failure of the control period in the cot. Four also met PSG criteria for failure while in the car seat. Five infants failed the car seat study on PSG criteria. Lower PMA at time of study predicted failure in both cot and car seat (p = 0.022 for both variables) but there was no relationship between weight at time of study and failure in the cot (p = 0.57) or car seat (p = 1.0). There was no effect of total obstruction on failure in the cot (p = 0.27) or car seat (p = 0.88), and the reflux index also did not predict failure in the cot (p = 0.97) or car seat (p = 0.91).
Comparison between nursing observations and PSG
The nurse failed seven infants, two because of persistent low oxygen saturation, one because of respiratory distress and four because of respiratory distress with low oxygen saturation. Three of the seven infants also failed on PSG criteria. Five infants had a marked increase in obstructive apnoea in the car seat, four were failed by the nurse and three failed on PSG criteria.
Accuracy of the clinically observed test
We assessed the accuracy of the clinical car seat test to predict PSG failure and an increase in obstruction on PSG separately. Clinical observation was more sensitive at predicting infants with increased obstruction in the car seat than failure of the PSG test (sensitivity 80% and 60%, respectively) but the positive predictive value of the test was low for both adverse outcomes (57% and 43%, respectively) indicating poor reliability. The high negative predictive value for both outcomes (91% and 82%, respectively) suggests that a pass of the clinical test should be reassuring.
DISCUSSION
What is already known on this topic
Both preterm and term infants can show respiratory compromise when placed to sleep in a car seat.
Car seat trials have been recommended for preterm infants to assess individual risk of respiratory compromise in a car seat before discharge from the neonatal unit without good evidence of their efficacy or accuracy.
Our study shows that a clinical car seat test by a nurse can detect infants with increased obstruction in a car seat but will not detect all infants at risk. In addition, it may assess infants as being at risk when they are no less stable in a car seat than in a cot. This can cause anxiety to parents and result in delay of discharge with no evidence of benefit to the infant. Preterm infants ready for discharge from the neonatal unit in this study had variable and individual cardiorespiratory responses, as measured by PSG, to being placed in a car seat during sleep. Although there were no group differences in the amount of obstruction apnoea experienced by infants after transfer to the car seat some infants did seem to have increases in obstructive apnoea in the car seat at a level that may be clinically important. Immaturity was the most consistent risk factor for cardiorespiratory instability, which occurred in both the cot and car seat. Infants at 35 weeks’ PMA are now often being discharged and these infants continue to have respiratory events not recognised by event monitors or staff.22 23
The strength of our study is that both obstructive and central apnoea were considered as well as the effect of respiratory events on oxygenation. Apnoeas ⩾5 s in length or shorter if associated with a greater than 2% desaturation were included for analysis although it is not clear if all these apnoeas are clinically notable. For this group of infants the range of values for the lowest saturation after apnoea recorded in active sleep was 71–93% for the time in the cot and 76–94% for the period in the car seat. Despite this, prolonged (⩾1 min) desaturation to <85% was seen in only three infants, two while in the cot and one while in the car seat.
Preterm infants are prone to obstruction particularly with neck flexion.24 Four of the five infants with an increase in obstruction were not yet term corrected age. Vulnerability to obstruction has been postulated as a reason for respiratory compromise in preterm infants in car seats but despite this few studies have measured obstructive apnoea. Willett et al studying preterm infants ready for discharge found obstructive apnoea was uncommon and not apparently exacerbated by the car seat.3 However many events were associated with what were described as short (5–20 s) mixed apnoeas. Others have shown that keeping the head in the neutral position while the infant is in the car seat can improve the size of the airway.25
In this study the nurse-observed predischarge test did not detect apnoea in any infant by apnoea monitor. Apnoea monitors that depend on abdominal movement will not pick up obstructive apnoea and impedance monitoring can also miss apnoea in preterm infants.26 We used PSG as the gold standard for detection of apnoeic episodes, allowing us to differentiate obstructive from non-obstructive events. Most infants with obstruction in the car seat were observed to be in respiratory distress. This assessment can be taught to parents without the need for a car seat test.
What this study adds
Preterm infants can show as much or even more compromise in a cot after a feed than is seen when they are sleeping in a car seat.
Some, but not all, preterm infants have an increase in obstructive apnoea after being moved from a cot to a car seat to sleep.
An observed car seat trial does not reliably pick up all adverse respiratory events experienced by preterm infants while sleeping in a car seat and may produce false positive results, which could potentially delay infant discharge.
Gastro-oesophageal reflux seemed to be uncommon and more likely during the period in the cot after a feed. This suggests that gastro-oesophageal reflux is not a major reason for the obstruction experienced by preterm infants in car seats although we may have missed some non-acid reflux. Not studying the infants in the car seat after a feed may have affected the results by increasing the level of obstruction seen in the car seat, but local clinical practice guidelines recommend that infants should not be placed in a car seat immediately after a feed.
We used the car seat provided by parents even though this meant a variety of car seats were studied. As none of these seats are specifically designed for such small infants it seemed reasonable to use whichever car seat the parents provided as this reflected the current clinical approach in the unit. This meant that for four infants the car seat design was such that the back of the seat was originally set at a 60° angle rather than at 45° as most car seats were. Car seats angled at 60° seemed to be not as well tolerated as those angled at 45° although our numbers were too small to confirm that the angulation of the car seat was a risk factor for obstruction.
A small decrease in central apnoea was seen after transfer to the car seat. This was only just significant and may not be clinically important. All central apnoeas ⩾5 s in length were scored whether or not they were associated with oxygen desaturation or arousal. Periodic breathing was not scored separately. Central apnoea is common in preterm infants of this corrected gestation, and currently there are no clear guidelines about which patterns of central apnoea should be considered clinically noteworthy.
This study deemed a nurse-led car seat trial not to be accurate enough to warrant use in our neonatal unit. We are still concerned about the vulnerability of infants in car seats and have chosen to use the equivalent amount of nursing time to educate caregivers more specifically about use of the car seat and how to recognise signs of respiratory distress. We advise parents to use car seats that do not have a steeply angled back. Caregivers are also instructed that immature infants being discharged from the neonatal nursery should be watched carefully while in the car seat and transferred back to their cot as soon as possible after the car journey ends.
REFERENCES
Footnotes
Funding: This study was funded by the New Zealand Cot Death Association. The PSG equipment was funded by the New Zealand Lotteries Board.
Competing interests: None.
- Abbreviations:
- PMA
- postmenstrual age
- PSG
- polysomnography