Article Text

Abstract
Background: Children born very preterm (VP; <32 weeks’ gestation) or with very low birth weight (VLBW, <1500 g; hereafter called VP/VLBW) are at risk for behavioural and emotional problems during school age and adolescence. At school entrance these problems may hamper academic functioning, but evidence on their occurrence at this age in VP/VLBW children is lacking.
Aim: To provide information on academic functioning of VP/VLBW children and to examine the association of behavioural and emotional problems with other developmental problems assessed by paediatricians.
Design, setting and participants: A cohort of 431 VP/VLBW children aged 5 years (response rate 76.1%) was compared with two large national samples of children of the same age (n = 6007, response rate 86.9%).
Outcome measures: Behavioural and emotional problems measured by the Child Behavior Checklist (CBCL), and paediatrician assessment of other developmental domains among VP/VLBW children.
Results: The prevalence rate of a CBCL total problems score in the clinical range was higher among VP/VLBW children than among children of the same age from the general population (13.2% v 8.7%, odds ratio 1.60 (95% confidence interval 1.18 to 2.17)). Mean differences were largest for social and attention problems. Moreover, they were larger in children with paediatrician-diagnosed developmental problems at 5 years, and somewhat larger in children with severe perinatal problems.
Conclusion: At school entrance, VP/VLBW children are more likely to have behavioural and emotional problems that are detrimental for academic functioning. Targeted and timely help is needed to support them and their parents in overcoming these problems and in enabling them to be socially successful.
- CBCL, Child Behavior Checklist
- VLBW, very low birth weight
- VP/VLBW, very preterm or very low birth weight
Statistics from Altmetric.com
- CBCL, Child Behavior Checklist
- VLBW, very low birth weight
- VP/VLBW, very preterm or very low birth weight
Survival of very preterm (VP) or very low birthweight (VLBW; hereafter called VP/VLBW) infants has increased considerably during the past decades.1–4 Developmental outcome varies with the age of the child, the population studied and the definition of handicap. Follow-up studies during the first 2 years of life indicate that very preterm and VLBW infants are at increased risk of chronic illnesses, especially chronic lung disease, cerebral palsy and severe developmental delay in 10–20% of survivors.3,5,6
Follow-up studies across longer intervals show that VP/VLBW infants are at even greater risk of developmental impairments and disabilities that may affect their academic functioning during school age and adolescence.4 These problems include poor motor performance, visual and auditory impairments, and poor cognitive and behavioural development.3–5,7,8,9,10,11,12,13 Problems at early school age seem to increase during the school career. In a nationwide follow-up study of VLBW infants in The Netherlands, attendance for special education increased from 19% at age 9 years to 28% at 14 years.14 Similar figures have been reported for children from Florida and Cleveland, USA.3,15
One explanation for the worsening school career of VP/VLBW children is that they are more likely to have behavioural and emotional problems that hamper academic functioning. School is usually the first group setting that requires complex social skills from children, implying that potential mental health problems in these children will become more pronounced at this age. However, there is very little evidence on the occurrence of these problems among VP/VLBW children at school entrance. A study on children born before 30 weeks’ gestation showed that 23% of the children had behavioural problems at age 5½ years according to their parents and 26% had problems according to their teachers.16 Further evidence is needed to help target interventions to the groups most in need and to behavioural problems most frequently found. The aim of this study is to compare the prevalence rate of behavioural and emotional problems at the age of 5 years among VP/VLBW children with those in children of the same age in the general population, and to assess the association of these behavioural and emotional problems with more general developmental problems among VP/VLBW children.
METHODS
We compared behavioural and emotional problems measured by the Child Behavior Checklist (CBCL) for VP/VLBW children and for two national samples of 5-year-old Dutch children.
Population
We obtained data on 431 children, delivered before 32 weeks’ gestation or with a birth weight <1500 g (called VP/VLBW children), born in three regions of The Netherlands between 1992 and 1995. They represented 76.1% of all VP/VLBW children born in these regions. Complete data were available on 402 of these children. The mean gestational age of the participating children was 30.2 (standard deviation (SD) 1.9) weeks and their mean birth weight was 1268 (SD 329) g. Of these 402 children, 258 (64.2%) were both very preterm and VLBW, 97 (24.1%) were only very preterm and 47 (11.7%) were only VLBW. Details on this sample have been reported by de Kleine et al.17
We further obtained data on 12 217 children from two representative general population samples (response rate 86.9%). Both sets of data were obtained within the framework of the routine preventive health assessments that are provided regularly to all Dutch children. The first sample related to a cross-sectional national study on children aged 4–15 years (response rate 90.1%; n = 4480), representative of the Dutch population.18,19 The second sample was related to the baseline measurements of 7737 children aged 4–6 years (response rate 85.2%) participating in a national randomised controlled trial on improvement of the early detection of psychosocial problems by child health physicians and nurses (child health professionals).20,21 We restricted our analyses to children from these samples in the same age group as the VP/VLBW children (n = 6007)—that is, 5 years, the age of obligatory school entrance in The Netherlands (most children enter school at age 4 years). The local institutional review boards concerned had approved all three studies. Written informed consent by parents was obtained for the first study and verbal informed consent for the other two studies.
Data and data collection
In all three samples, parents completed the CBCL before assessment by a paediatrician or a child health physician. The CBCL is a well-validated questionnaire on behavioural and emotional problems over the preceding 6 months.22,23 It contains 120 problem items on the basis of which a total problems score can be computed. We computed eight syndrome scales, two broad groups of syndromes designated internalising and externalising, and a total problems score. Internalising consists of withdrawn behaviour, somatic complaints and anxious/depressed syndrome scales, and externalising consists of delinquent and aggressive behaviour syndrome scales. Children were allocated to a normal or a clinical range of the scoring distribution based on the Dutch normative sample.23 Cut-offs were set at the 97th centile for the eight syndrome scales and at the 90th centile for the total problems, and internalising and externalising scales.
Subsequently, paediatricians assessed all VP/VLBW children regarding neurological and cognitive functioning, language and general health in a structured way. On the basis of the assessment, the children were categorised into three groups: optimal (all assessment domains normal), at risk (more detailed examination or treatment necessary) and abnormal (abnormal in at least one domain). If for any domain further assessment or treatment was deemed necessary, the child was classified as having developmental problems. Data were also obtained on severe problems in the perinatal period among the VP/VLBW children, which had been registered prospectively. Details have been provided by de Kleine et al.17
Analysis
We first compared background characteristics across the samples (ie, age, sex, family composition and size, and maternal educational level) using the χ2 test. Next, we compared the mean scores for all CBCL scales using the t test. We repeated these analyses with adjustment for differences in background characteristics between the samples, using analysis of variance and F tests. Moreover, because of the non-normal distribution of the CBCL scores, we confirmed the statistical tests for the crude analyses by the non-parametric (Mann–Whitney U) test. Next, we carried out the same analysis on dichotomised scores (ie, clinical v normal), using logistic regression. We then computed standardised differences (mean difference/standard deviation (SD)) between the two groups to adjust for differences in means and variability across the various CBCL scales. We also used the t test to examine differences in the frequency of behavioural and emotional problems between children with and without paediatrician-assessed developmental problems; between children who were only very preterm, only VLBW, or both; and between children with and without severe problems in the perinatal period (Apgar score of <7 at 5 min, grade 3 or 4 intraventricular haemorrhage, artificial respiration for ⩾1 week and use of steroids for bronchopulmonary dysplasia).17 Finally, we examined differences by sex, also using the t test.
RESULTS
The VP/VLBW cohort and the reference samples had similar background characteristics except for maternal educational level, which was lower for VP/VLBW children (p<0.05; table 1).
Background characteristics of the very preterm or very low birthweight children and children from the Dutch general population*
VP/VLBW children had higher mean scores on CBCL total problems, on internalising and externalising problems, and on all syndrome scales (p<0.05), except for sex problems and anxious/depressed behaviour (table 2). Repetition of the analyses with adjustment for background characteristics did not affect differences in any important way (data not shown). The Mann–Whitney U test mostly confirmed the results of the t test (table 2).
Mean Child Behavior Checklist scores of very preterm or very low birth weight children and children from the Dutch general population (aged 5 years)
Table 3 shows that the proportion of children scoring in the clinical range of CBCL total problems was 13.2% among VP/VLBW children versus 8.7% among those from the general population (odds ratio (OR) 1.60, 95% confidence interval (CI) 1.18 to 2.17); for the somewhat lower borderline cut-off criterion, these figures were 22.1% v 15.0% (OR 1.61, 95% CI 1.26 to 2.05), respectively. The proportion of VP/VLBW children scoring in the clinical range was higher also for externalising problems but not for internalising problems. Differences in proportions regarding separate syndrome scales reflected those for mean scores, although some differences did not reach statistical significance, considering the relatively small proportions of children with a clinical score.
Prevalence rates of scores in the clinical range on Child Behavior Checklist problems scales for very preterm or very low birthweight children and children from the Dutch general population (aged 5 years)
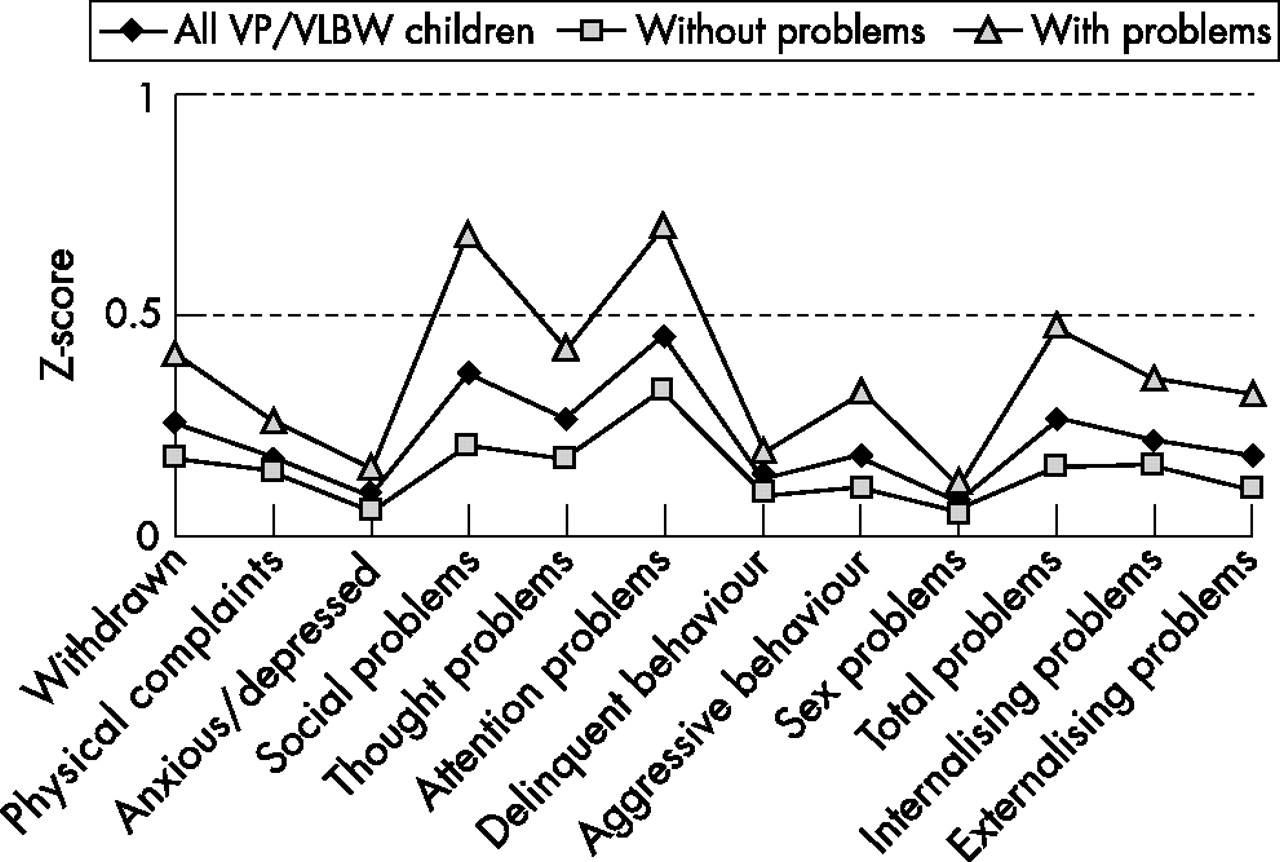
Standardised differences (effect sizes) ranged from 0.08 to 0.44 (fig 1). Values for four CBCL syndromes and for externalising and total problems were >0.2, which Cohen24 designates as small effects, which were largest for attention and social problems. Differences were much larger for VP/VLBW children in whom the paediatrician assessed developmental problems than for the other children. Again, excesses in problems were largest for attention and social problems, 0.70 and 0.67, respectively, which Cohen24 designates as medium (ie >0.50) effects. Regarding the group with paediatrician-assessed problems, the excess of problems was larger if the paediatricians were certain of the existence of developmental problems than if they were uncertain and first needed additional investigation, for all CBCL syndromes (data not shown).

{kind=link}
Standardised differences in mean Child Behavior Checklist scores of very preterm or very low birthweight (VP/VLBW) children and those of children in the general population (that form the zero x axis level of the figure), overall and separately for children with and without paediatrician-assessed developmental problems (age 5 years).
Whether the children were only very preterm, only VLBW or both had no statistically significant effect on differences in behavioural and emotional problems, and neither had the 5-min Apgar score. However, children who had needed artificial ventilation for at least 1 week in the neonatal period (n = 66) had significantly higher scores on social (p<0.001) and attention problems (p = 0.020). Children with grade 3 or 4 intraventricular haemorrhage (n = 19) had higher scores on somatic complaints (p = 0.027), and children who received corticosteroids (n = 14) had higher mean scores for total problems (p = 0.028), and social (p<0.001), thought (p = 0.011) and attention problems (p = 0.014). In all cases, differences between the VP/VLBW children without additional perinatal problems and children from the general population sample remained statistically significant. Moreover, differences regarding receipt of artificial ventilation, presence of intraventricular haemorrhage and receipt of corticosteroids were much smaller than those regarding paediatrician-assessed problems at 5 years (fig 1).
Finally, the excess of problems among VP/VLBW children differed somewhat by sex (table 4). Among VP/VLBW boys, this excess was slightly larger for behavioural (externalising) type problems, but sex-related differences were statistically significant regarding only social and attention problems. Among girls, the excess of problems was somewhat larger for emotional (internalising) type problems, but this sex-related difference was statistically significant regarding only the withdrawn behaviour on the CBCL syndrome scale.
Mean Child Behavior Checklist scores of very preterm or very low birthweight children and of children from the general Dutch population, by sex (age 5 years)
DISCUSSION AND CONCLUSION
The results of our study using large national samples showed that behavioural and emotional problems occur more frequently among 5-year-old VP/VLBW children. Differences are found in most types of problems, but are largest for social and attention problems. Increases in the prevalence of clinical scores are larger for behavioural than for emotional problems. Moreover, they are much larger in children with paediatrician-assessed developmental problems and somewhat larger in children with severe neonatal problems, especially those needing corticosteroids. For 5-year-old children, our results confirm the findings from previous studies on other age groups that indicated that behavioural and emotional problems were more likely among very preterm, VLBW or VP/VLBW children.3,4,9,11–13,25–27
The difference in mean scores of VP/VLBW children and those of children from the general population was similar for internalising and externalising problems, whereas most previous studies found an excess of externalising and attention problems.12 However, when examining clinical scores, we also found an excess of externalising and attention problems, but not of internalising problems. This indicates that mean levels of internalising problems are somewhat increased among VP/VLBW children, but that these increases are mostly moderate (whereas they are more pronounced for the other types of problems). At the level of specific CBCL syndrome scales, standardised mean differences between the two groups (fig 1) were largest for the scales designated as attention problems, social problems, thought problems and withdrawn (by decreasing size of standardised differences). An explanation for the larger mean excess of internalising problems among VP/VLBW children in our study, especially withdrawn behaviour, may be that this behaviour becomes especially visible when children enter school. At that particular moment, owing to the higher prevalence of intellectual and physical problems, a VP/VLBW child may be shyer than average. This situation-oriented character of emotional problems could also explain the moderate nature of this excess that seldom reached a clinical level.
Regarding withdrawn behaviour, we found larger mean differences between VP/VLBW children and children from the general population for girls than for boys. Sykes et al28 and Botting et al26 found similar sex-related differences among older school-aged (7–8-year-old and 12-year-old) VLBW children. However, most studies aiming at VLBW children in these age groups found no sex-related differences.11 On the other hand, Hack et al12 found an excess of this type of withdrawn behaviour also among 20-year-old VLBW women according to both parent reports and self-report, but not among men in this age group. This can be interpreted as an increased vulnerability for this type of problem among VLBW women.
Regarding externalising and attention problems, most studies have shown VLBW boys to be more susceptible to problems than boys from the general population,12,25–27 and our study is no exception. We found especially large differences between VP/VLBW boys and boys from the general population regarding social and attention problems. The process of school entrance may reinforce this well-known effect of VP/VLBW on children, and the rather general response of children to this process, that they become either too active or too shy, may simply be more pronounced among this group. School is the first setting in which children really have to concentrate on specific tasks for long periods, and have continuous social interaction in a large group. Nadeau et al29 showed that a relatively isolated problem in working memory may explain attention problems among 7-year-old VP/VLBW children. Targeted educational assistance for VP/VLBW children and their parents during at school entrance might help them in overcoming such attention problems.
Regarding other types of externalising problems, such as aggression and delinquent behaviour, we found a somewhat higher prevalence, but not a large excess, among VP/VLBW children for each sex. This may imply that a (very) low birth weight is associated with problems in normal social interaction with others, without leading to more general antisocial behaviour. A second domain showing relatively numerous problems among VP/VLBW children relates to attention and thinking, which seem to be specifically vulnerable to the consequences of being born with very low weight.
Overall, our results show rather general difficulties in the domain of socioemotional development. This may indicate that an underlying developmental problem affects several domains, as our study also shows more behavioural and emotional problems among VP/VLBW children with paediatrician-confirmed problems than among others. Another study on extremely preterm children also found that many children show disabilities in more than one developmental domain.16 These problems at 5 years of age were related to developmental outcome measures at 2 years. A study that longitudinally followed up a group of preterm children until 10 years of age and distinguished between subgroups according to academic problems present at 10 years showed differences in the developmental course of these subgroups that gradually diverged during the first 2 years.30 Interventions regarding behavioural problems may therefore be already appropriate in toddlers.
We found smaller differences between VP/VLBW children and those from the general population than those found by Hille et al31 regarding extremely low birthweight (<1000 g) Dutch children aged 8–10 years. Extremely low birthweight children can be expected to have more developmental damage in general. Thus, there is a dose–response relationship between this general developmental damage and the occurrence of behavioural and emotional problems, similar to that in other developmental domains.32
Potential limitations
Our study used large samples with high response rates, in which data were obtained using a standardised method. Moreover, we used the CBCL questionnaire, which has been shown to be a valid measure for behavioural and emotional problems.22,23 Although response rates were somewhat higher in the population samples than in the VP/VLBW sample, even if all non-responding VP/VLBW children had CBCL scores in the normal range, most differences would remain statistically significant. The reverse, a higher prevalence of problems among non-responding VP/VLBW children, seems, however, to be more likely.33,34 If so, differences between VP/VLBW and normal children will be even larger than we found. Moreover, our study may still have somewhat underestimated differences, because some VP/VLBW children may also have been included in the population sample. Finally, our study lacked an in-depth psychiatric interview and additional behavioural observations that would have enabled a more specific description of mental health problems.
What is already known on this topic
-
Survival of very preterm or very low birthweight (VP/VLBW) infants has increased considerably during the past decades.
-
Surviving VP/VLBW infants are at increased risk of developmental impairments and disabilities that may impair their academic functioning.
What this study adds
-
By using large national samples, it was shown that both behavioural and emotional problems occur more often among 5-year-old children who were born very preterm or with very low birth weight.
-
Differences are largest for social and attention problems.
Implications
The relative proportion of surviving VP/VLBW children among all births has increased during the past decades,1,3–5,11 and our results show that these children are 50% more likely than children from the general population (13% v 9%) to have CBCL problems scores in the clinical range. The increased prevalence of problems among this group can therefore be expected to increase the burden of mental health morbidity among children in the community. Paediatricians and other child health professionals working with VP/VLBW children should thus be prepared to meet relatively many behavioural and attention problems, and should also prepare parents concerning this.35 Routine screenings for these problems36,37 should be intensified among the VP/VLBW children. Moreover, routine follow-up examinations regarding different developmental domains of VP/VLBW children should be carried out to identify potential problems as soon as possible.
Our results further show that this higher rate of problems continues at school age, which may imply an increased need for additional support at school or even specialised school services. VP/VLBW children could also be offered supportive treatments from birth onwards to improve developmental outcomes.35 However, results of studies conducted on the effectiveness of the treatments so far vary,38 with decreasing effects in the longer teem, indicating a continued need for specific and age-appropriate assistance.39,40 The results of our study show that better health gain may be achieved in VP/VLBW children. This urgently requires effective programmes that continue at least into school age, to maintain positive long-term effects,4,29,35 paying special attention to VP/VLBW children who have had severe difficulties in the perinatal period.
Acknowledgments
We thank Roy E Stewart, statistician, for his advice.
REFERENCES
Footnotes
-
Published Online First 28 July 2006
-
Funding: The fieldwork for this study was supported by grants from the Dutch Health Organisations Praeventiefonds, project number 28–2756, and from The Netherlands Organisation for Health Research and Development (ZonMw), project number 1010004–20.
-
Competing interests: None.
Linked Articles
- Fantoms