Article Text

Abstract
Aims: To assess what proportion of all cardiac abnormality can be suspected at birth when all clinical examination before discharge is undertaken by a small stable team of clinicians.
Methods: A prospective audit of all the 14 572 births in a maternity unit only staffed by nurse practitioners between 1996 and 2003.
Results: 1.2% of all babies born in the unit were found to have a structural defect (as confirmed by echocardiography) within a year of birth. The number not suspected before discharge declined over time, and only 6% were first suspected after discharge in the last four years of this eight year study. Four potentially life threatening conditions initially went unsuspected in 1996–8, but none after that. A policy of referring every term baby with a murmur at 1 day of age that was still present at 7–10 days resulted in 4.2% requiring cardiac referral; 54% of these babies still had a murmur when assessed one to two weeks later, and 33% had a structural defect. Parents said in independent, retrospectively conducted, interviews that they found it confidence building to have any possible heart defect identified early and the cause of any murmur clearly and authoritatively explained.
Conclusions: Effective screening requires experience and a clear, structured, referral pathway, but can work much better than most previous reports suggest. Whether staff bring a medical or nursing background to the task may well be of less importance.
- cardiac murmur
- congenital heart disease
- examination
- screening
Statistics from Altmetric.com
It has long been assumed that a doctor ought to examine every baby at birth, but it is now being suggested that this can be done, just as effectively, by an appropriately trained neonatal nurse1 or midwife.2,3 Although this could well be true for most aspects of the standard predischarge examination, it is not yet clear how effective such staff are at detecting signs of congenital heart disease. Medical examination typically picks up slightly more than half the defects of any structural significance.4 Only a few of these abnormalities are life threatening, but the early recognition of those that are can be life saving.5,6 When nurse practitioners became responsible for all aspects of the care of the babies born at Ashington Hospital, Northumberland therefore they initiated a formal review of this aspect of predischarge care.7 This paper reports the outcome of the first eight years of that prospective audit.
METHODS
Setting
A team of eight nurse practitioners became responsible for all the predischarge care of the 1800 babies born each year in the maternity unit in Ashington when on-site paediatric cover ceased to be available in 1996. The nature of the change that this involved, and the quality of the service now on offer, have been discussed elsewhere.8 Despite these changes there has been no change in the unit’s obstetric booking criteria, which remain the same as in the other 14 obstetric units in the north of England that do not undertake long term neonatal ventilation. Less than 3% of the babies booked for delivery each year are eventually transferred elsewhere for care before or after birth, and even these babies spend, on average, three quarters of their time before discharge in Ashington because of early back-transfer.7
Predischarge assessment
Unless the mother was among the 1–2% who had arranged to return home immediately after delivery, those term babies who were well were only examined for the first time when they were a day old. If a murmur was identified during full cardiovascular examination, saturation was assessed by pulse oximetry, and a further check was undertaken to see if the murmur had disappeared by the time the mother was ready to go home. If a murmur was still heard, the parents were told (both verbally and in writing) what to do should the baby start to become unwell or to feed poorly. They were also asked to bring the child back for review after another three to six days so that a decision could be taken about referral to the regional cardiothoracic centre in Newcastle. Until early 2001, a paediatrician made that decision, but, since then, the nurse practitioners have referred babies to that centre’s weekly assessment clinic themselves. Preterm babies were assessed at regular intervals in much the same way, and a decision taken about the need for referral when they were nearly ready for discharge home. Babies with breathlessness, poor pulses, or other signs suggestive of left ventricular outflow tract obstruction, or an otherwise unexplained functional leg saturation below 90%, were referred for cardiac assessment before discharge. Babies going home within 24 hours of birth were examined before discharge, but only after the importance of getting the family doctor to undertake a second examination had been stressed. This paper summarises the outcome of an audit of that assessment process from the time it was first set up in 1996.
Audit criteria
A record has been kept, with help from the regional congenital abnormality register,9 of the outcome of every pregnancy where the mother delivered (or booked for delivery) in Ashington, but the present audit has been limited to a review of those babies whose predischarge examination was undertaken in Ashington and in whom a structural heart defect was eventually confirmed either by a consultant paediatric cardiologist by echocardiography, or at autopsy. Babies in whom the only abnormality was cardiomyopathy, dextrocardia, dextroposition, an arrhythmia, or a cardiac tumour have been excluded. So too have babies in whom the only abnormality was a bicuspid aortic valve (unless there was stenosis). Babies in whom interatrial flow was detected were only included if this persisted for more than a year. Ductal patency in the term baby was included if it persisted for more than six weeks, but cases occurring after preterm birth were excluded. The severity of every defect was classified using the approach adopted by the recent UK Health Technology Assessment (HTA) report,4 and a record kept of those defects that required surgery, and those that resolved spontaneously, within a year of birth. All babies first suspected of a heart defect after discharge in the area served by the maternity unit are soon referred to the regional cardiothoracic centre for assessment, making it possible to assess both the sensitivity and specificity of the unit’s current screening policy.
Parental views
In 2002–3 the Community Health Council asked mothers who had recently delivered a healthy baby at term in any of the five maternity units used by mothers in Northumberland what they thought about their baby’s predischarge care.10 Seven hundred were sent a postal questionnaire, and 20 of these families were later asked a small number of supplementary questions over the phone. Another 100 families were interviewed face to face. The views expressed by 16 mothers whose babies were found to have a heart murmur at birth are reported here.
Ethics approval
Ethics approval for this study was obtained as part of the wider review of the quality of the neonatal care provided by the Ashington unit after all on-site paediatric support was withdrawn in 1996, as described in the audit report published in 2004.7 Separate ethics approval was obtained for the study conducted by the Community Health Council in 2002–3.10
RESULTS
Defects identified within a year of birth
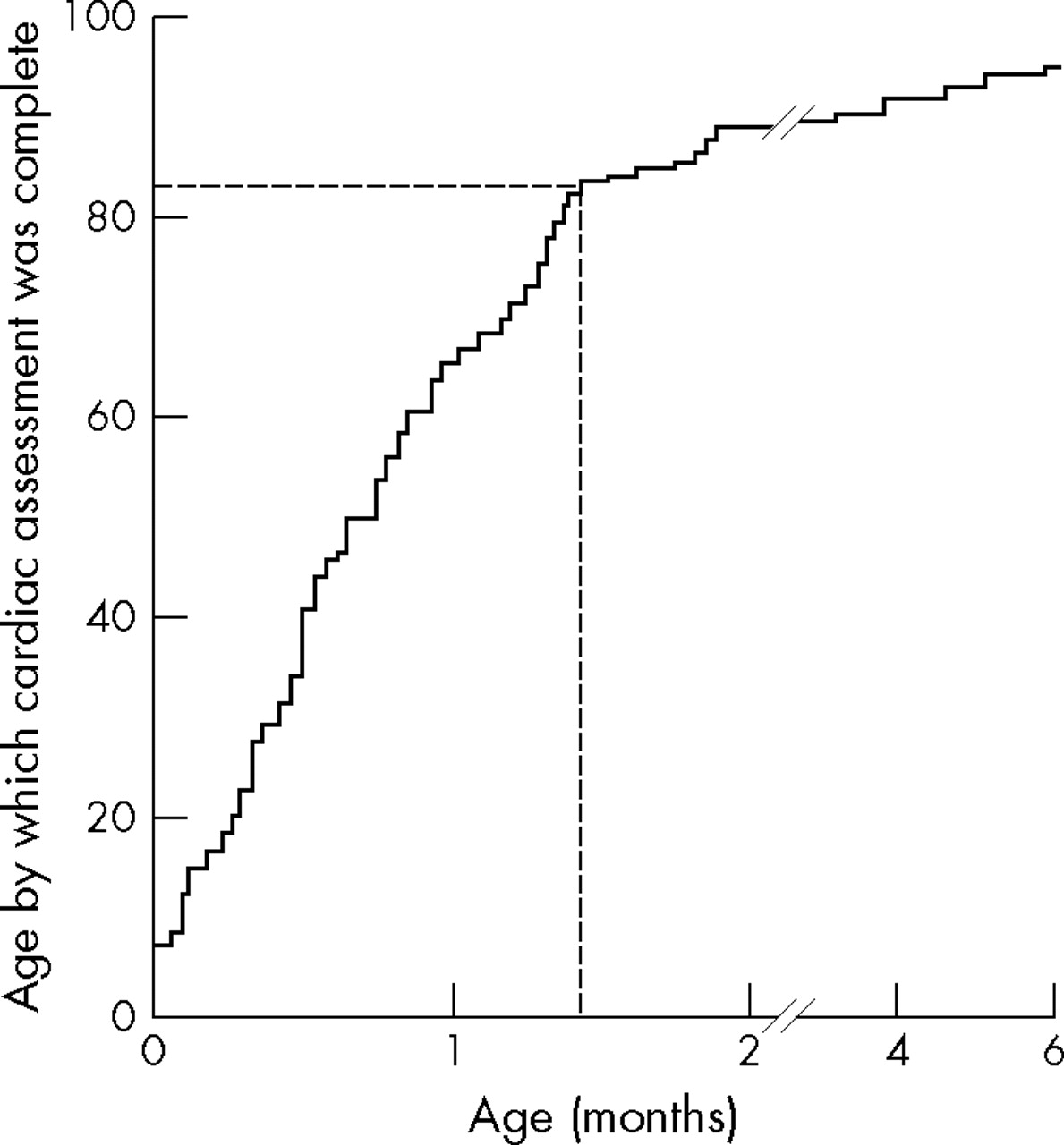
Of the 14 572 babies cared for in the unit between 1996 and 2003, 176 (1.21%) were found to have a structural heart defect before they were a year old (table 1). Congenital heart disease had been suspected in 150 of these babies before discharge. Detection improved from 73% in 1996–7 to 80% in 1998–9, and to 94% in 2000–3. The sensitivity of the referral process during the second four year period, as measured by the number of structural defects identified, was 94.3% (95% confidence interval 89.5% to 99.2%), and the fact that 239 babies were referred for assessment in that time generates a specificity of 97.7% (97.3% to 98.0%). Figure 1 shows the time it took for a firm diagnosis to be made during the second four year period.
Structural heart defects identified within a year of birth

Age at which the 88 babies born in 2000–2003 in whom a cardiac defect was detected within a year of birth were first seen by a cardiologist; 80% of diagnoses had been confirmed within 6 weeks of birth.
Using the recent HTA classification,4 just 20 of the 176 defects could be considered potentially life threatening (table 2). Four babies with a potentially life threatening defect were missed in the first three years of this eight year study, but all were subsequently identified, and cardiac referral effected before they became symptomatic (table 3). Only five defects were missed in the second four year period (table 1). None were of major clinical import. Three were small atrial septal defects, and two were small ventricular septal defects (VSDs); all were picked up by the family practitioner within two months of birth.
Structural heart defects coming to light within a year of birth 1996–2003 inclusive
Potentially life threatening cardiac defects not suspected before discharge
Cardiac defects were also found between 1996 and 2003 in 12 fetuses where pregnancy was terminated because of a chromosome abnormality, and five other pregnancies where a serious structural abnormality was suspected. Defects were also found in one stillbirth, and one unresuscitatable, multiply malformed, live birth. Another two babies who died of severe immaturity within six hours of birth were found, at autopsy, to have a VSD. The defects in five of these 21 babies were potentially life threatening. Inclusion would have increased birth prevalence to 1.36%.
Review of the assessment process 2001–3
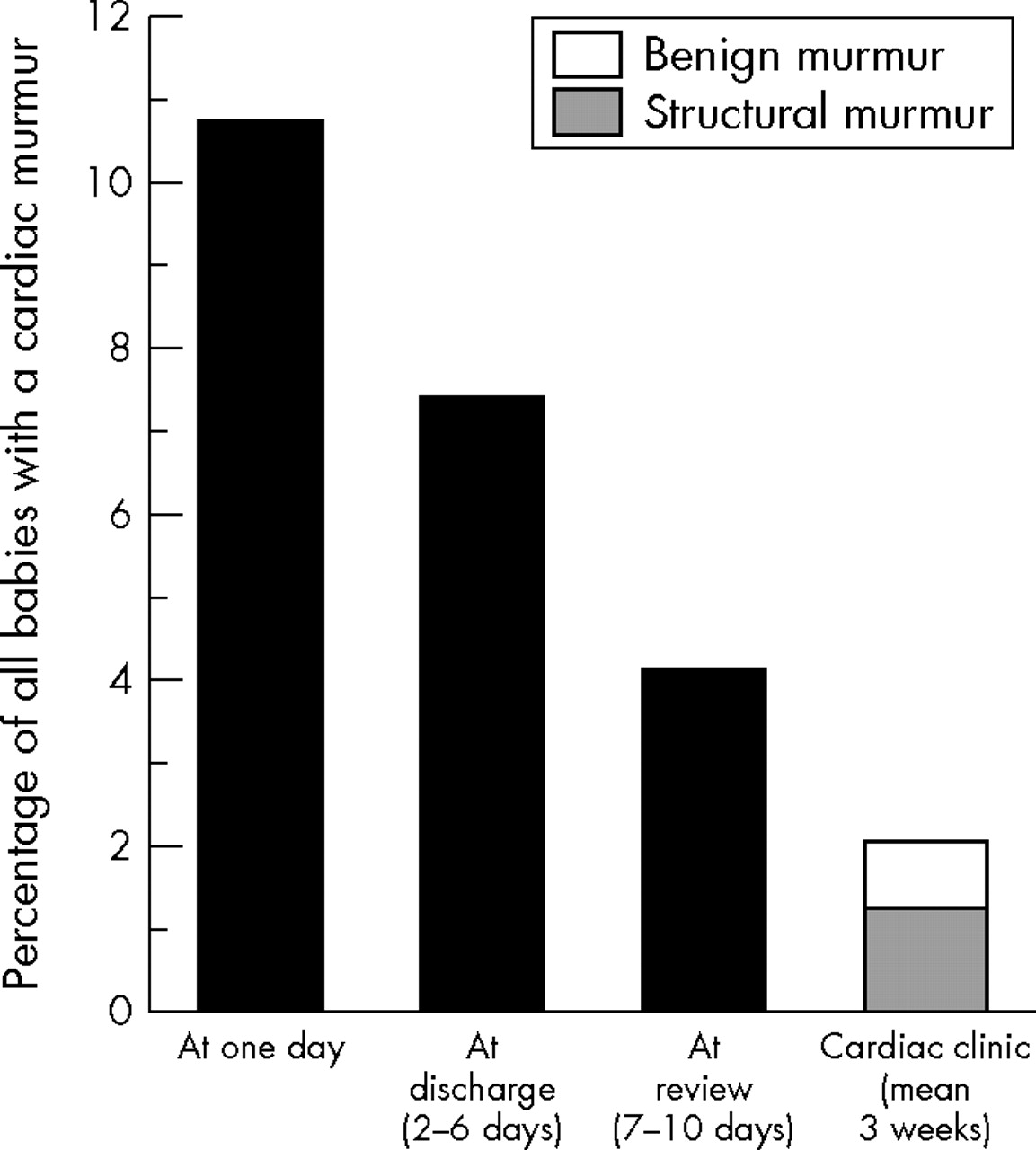
Figure 2 summarises a more detailed audit of the management of the 4779 babies of 36 weeks gestation or more born in 2001–3. Six who were cyanosed or otherwise obviously unwell underwent urgent predischarge referral; 10.7% of the others had a murmur, but were asymptomatic when first examined a day after birth. Nearly 40% of these still had a murmur on review at 7–10 days, and a fifth (2.3%) still had a murmur when seen by a paediatric cardiologist, on average, three weeks after birth. Sixty per cent of those who then had a murmur (1.4%) had a structural defect, and in two thirds of those with a “benign” murmur there was evidence of pulmonary artery branch stenosis,11 a small atrial septal defect that closed within a year of birth, or some minor pulmonary valve stenosis.
{kind=link}
{kind=link}
Of the 4779 babies born at 36 or more weeks gestation in 2001–3, 515 had a murmur when first examined one day after birth; 203 still had a murmur on review at 7–10 days, and 109 still had a murmur at cardiac review. Sixty seven of those with a murmur at cardiac review had a structural defect. None of these defects had been suspected antenatally.
Defects identified in babies more than a year old
Thirteen heart defects have so far come to light among the 14 572 children born between 1996 and 2003 when they were more than 12 months old. VSDs accounted for a third of these late diagnoses. As a review of earlier birth cohorts shows that it is now rare for heart disease to present for the first time when a child is more than 4 years old and as less than 2% of all children migrate out of the study area before then, there is likely to be little residual under-ascertainment.
Parental views of the screening programme
Sixteen mothers interviewed during the Community Health Council study had been told, before discharge, that their baby still had a heart murmur on review 7–10 days after birth. Nine of these babies were later found to have a heart defect, and two others had a benign murmur that persisted for at least six months. Thirteen of these mothers said that they had not found the two to three week delay before they saw a cardiologist particularly stressful once the reason for the referral, and the way it would be managed, was explained to them. Three also said, without prompting, that the early identification of what turned out to be a “normal” murmur, or a VSD that closed spontaneously, had led them, retrospectively, to value the thoroughness with which their child’s initial examination had been conducted. Two volunteered that the clear and authoritative way in which the nature of their child’s heart problem (or non-problem) had been explained had left them more self confident when they had to take their child for subsequent health checks, and another four expressed similar views when specifically asked about this. Three mothers, in contrast, said that that they had been very worried to learn that their child had a “murmur” but told nothing more after that until seen by a cardiologist. None of these three had been delivered in Ashington.
DISCUSSION
Parents and staff alike attach great importance to the careful examination of every baby at birth, and heart defects are known to account for most of the abnormalities of clinical significance that are not visible to the naked eye at delivery. It used to be said that about 0.6% of all babies had a heart defect at birth,12 but several recent studies have suggested that the true figure is probably closer to 1%,13,14 and that earlier studies missed quite a lot of the VSDs that were destined to close spontaneously early in life.12,14–16 More than 1.2% of all the babies in the present study were eventually found to have had a defect at birth but, if isolated septal defects undergoing spontaneous closure within a year are excluded, prevalence at birth is closer to 0.9% (table 2).
Very few reviews of the effectiveness of neonatal screening exist with which to compare the present findings.17–21 Most studies have only reviewed the assessment of term babies who seemed well at birth,19–21 and these reports are not therefore directly comparable. Only three have reported, not only on what was found before discharge, but also on what was only identified later in the first year of life.18,20,21 Many would doubt that the proportion with a “real” murmur at 1 day was as high as reported here, but that is consistent with what others who only examined a moderately small number of babies with some care have also reported.22,23 A combination of prompter recognition, prompter referral, and prompter outpatient assessment has progressively reduced the time taken to establish a firm diagnosis during the course of this eight year study, and a diagnosis had been made within six weeks of birth in 80% of babies in the second four year period (fig 1). That had only been true of 53% of the babies delivered in medically staffed units in the north of England 10 years ago.20
Because no formal baby check was undertaken, as a matter of unit policy, until at least 24 hours after delivery, overt problems, such as poor feeding, poor colour, or early jaundice, had nearly always been noticed by the parents, or by the midwifery staff, by the time the predischarge check was carried out. Parents were also reminded that discharge was simply discharge home and not discharge from midwifery care, that the community midwife would continue to visit, and that they could bring the baby back to the unit at any time should they become worried about anything. How often heart disease would have been suspected had the first check been performed before the babies were a day old is hard to say. Examination is said to be carried out earlier than this in most units in the United Kingdom at present,24 but delay does give more time for symptoms to emerge, and parents rather longer to formulate and express any questions or concerns they may have.
Several factors probably help to explain the effectiveness of the present screening programme. Ascertainment has clearly improved over time (table 1), and the fact that all examinations were undertaken by a small core of increasingly experienced people must have contributed to this. The fact that a prospective audit was being conducted may have had some impact on the diligence with which assessments were carried out. The existence of an audit “feedback” loop almost certainly helped—in most units the staff who refer babies for further assessment seldom get to hear what the outcome of that assessment revealed. The fact that all the babies with a persisting murmur were referred for full evaluation in the second four year period, and that no attempt was made to judge whether some murmurs were “benign”, certainly reduced the number of occasions when a structural defect was missed.
The only defects overlooked in the second period were five isolated septal defects, and it is not unreasonable to suppose that these babies may not have had a murmur when they were only 1 day old because, at that stage, some trans-septal pressure gradients are still probably small. If this is true, it would only be possible to detect these cases before discharge by examining every baby more than once. As the only defects missed were of little immediate import and were picked up by the family practitioner at the six to eight week assessment anyway, repeat predischarge examination is not very likely to be cost effective.
Four of the 20 children born with a condition of potentially life threatening severity in this eight year study had conditions that went unsuspected before discharge (table 1). All were delivered in the first three years of this eight year study. It is likely that two of these would have been picked up had every baby been screened for subclinical cyanosis with a pulse oximeter before discharge (table 3).25,26 However, the cost effectiveness of screening all children,4,27 rather than a selected subgroup, in this way will vary inversely with the effectiveness of the main clinical examination. There is a need to improve the way the primary clinical examination is often conducted before adding to its complexity.
Only a third of the otherwise well term babies referred for full assessment in 2001–2003 turned out to have a structural defect (fig 1), a proportion similar to that recently reported from two medically staffed units.19,21 Having established that the number with an audible murmur decreases over time, staff are now looking to see whether it is possible to reduce the number referred by delaying their own reassessment of these babies until they are 2 weeks old as long as they remain asymptomatic. Parents do not seem to find the delay inherent in the present screening system (fig 2) unduly stressful as long as they are properly informed of what is going on and why. Most also seem to understand that, as with testing for other conditions such as deafness,28 the system only works as well as it does because the initial screen picks up some “false positives” along with all the “true positives”. It is, however, known that the time parents spend waiting for a cardiac diagnosis often generates more stress than the diagnosis itself.29
The audit reported here seems to have vindicated Northumberland Health Authority’s decision to let nurse practitioners take over the work previously carried out by resident paediatric staff. Whether that success can be replicated elsewhere may depend on whether the nurses or midwives called on to do that work get the chance to build up enough experience to start doing it well. It may also depend on whether they get the chance to build up as effective a working relationship with a clinician experienced in echocardiography as the one described here. Given the importance that parents and clinicians alike attach to the clinical examination of every baby at birth, it is, perhaps, surprising that there is almost no published information as to the effectiveness of that examination.
What is already known on this topic
-
Examination at birth only seems to identify about half the babies found to have structural heart disease by the time they are a year old in most hospitals in the UK at present
-
Although much of the heart disease that is missed is trivial, some is potentially life threatening
Any excessive focus on whether that examination detects a murmur can, nevertheless, be dangerously misleading, because some babies with a potentially life threatening condition, such as preductal coarctation, do not have a murmur (and are not cyanosed either).30 Getting parents to understand that they can, and should, return to the unit where their baby was delivered if they have any worries seems to have achieved as much as the initial examination for signs of heart disease to ensure that the few babies who did have a serious defect reached a cardiologist before they became dangerously unwell.
What this study adds
-
Having a small team carry out every predischarge examination, and providing them with a structured referral pathway, resulted in more than 90% of all heart disease being suspected before discharge, and experienced nurses were able to manage that examination without on-site medical support
-
Only a larger case series will show that such a system reliably recognises all potentially serious heart disease promptly
Acknowledgments
This study would not have been possible had there not been a collaborative, region-wide, congenital abnormality survey in existence in the north of England (NorCAS),[9] and we are extremely grateful to Dr Christopher Wren, the consultant responsible for maintaining the cardiac component of that register, for support and advice, and for checking the accuracy of all the data on which this review is based. We are grateful to the secretarial staff, and to the Ashington unit’s part time audit nurse, Kathleen Davidson, for their careful maintenance of the correspondence files without which it would never have been possible to document what happened to many of the children referred for further assessment. We are also grateful to Graham Stacey, for permission to quote from the parental interviews he undertook for Northumberland Community Health Council.
REFERENCES
Footnotes
-
Published Online First 17 March 2006
-
Competing interests: EH started the region’s congenital abnormality register. He was also the first to suggest the development of a nurse led unit to Northumbria Health Authority in 1993, but had retired before the unit opened. CP has been one of the nurse practitioners at the unit since 1996. Neither received funding for this study.