Article Text

Abstract
Background: Bronchopulmonary dysplasia is an inflammatory fibrotic condition produced as a consequence of injurious influences in the neonatal lung. Exposing the premature lung to high concentrations of oxygen is thought to play an important part in lung injury pathogenesis.
Objective: To see if the amount of oxygen used during resuscitation at birth triggers events that lead to the subsequent lung injury and if a reduction in oxygen used leads to a reduction in lung injury.
Method: The outcomes of newborn babies less than 31 weeks gestation who were resuscitated using either 50% or 100% oxygen were examined. Eight of the babies receiving 50% oxygen required an increase in their oxygen concentration. Evidence of pulmonary inflammation was determined by quantifying interleukin 6, 1β, and 10 and tumour necrosis factor α in bronchoalveolar lavage fluid by enzyme linked immunosorbent assay.
Results: There were no significant differences in any of the cytokines studied in either of the groups. Death occurred in 5/26 (19%) babies who received 100% oxygen and 4/26 (15%) babies who received 50% oxygen. Survival without bronchopulmonary dysplasia at 36 weeks postmenstrual age occurred in 14/26 (54%) and 13/26 (50%).
Conclusion: Reducing the oxygen to 50% at resuscitation did not influence either short or long term outcomes, but a small benefit could not be excluded. There was no increase in adverse clinical outcomes in babies who received 100% oxygen.
- BAL, bronchoalveolar lavage
- BPD, bronchopulmonary dysplasia
- IL, interleukin
- PIP, peak inspiratory pressure
- ROS, reactive oxygen species
- TNFα, tumour necrosis factor α
- bronchoalveolar lavage fluid
- bronchopulmonary dysplasia
- cytokines
- oxygen
Statistics from Altmetric.com
- BAL, bronchoalveolar lavage
- BPD, bronchopulmonary dysplasia
- IL, interleukin
- PIP, peak inspiratory pressure
- ROS, reactive oxygen species
- TNFα, tumour necrosis factor α
Bronchopulmonary dysplasia (BPD) is an inflammatory fibrotic condition produced as a consequence of injurious influences in the neonatal lung. The process of inflammation within the premature lung is a host response to several injurious insults such as volutrauma, infection, and oxygen toxicity. Exposure to high concentrations of oxygen is thought to play a significant part in the pathogenesis of lung injury, through damage caused by toxic reactive oxygen species (ROS) or oxygen free radicals.1,2 ROS are derived from sequential incomplete reduction of oxygen within the cell and can damage lipids, carbohydrate, and proteins causing enzyme dysfunction and loss of integrity of cellular and organelle membranes, with resulting cellular dysfunction.3,4
ROS have also been shown to damage genetic material and are known to activate nuclear factor κB, which enhances the expression of many cytokine genes involved in inflammation.5,6
Pulmonary inflammation is a complex cascade of events in which cytokines are responsible for both the promotion and modulation of the inflammatory process. Several cytokines have been found to be prominent in the early stages of this inflammatory process in the ventilated premature baby.7,8,9,10,11,12,13,14
It is possible that the use of 100% oxygen during resuscitation at birth is responsible for initiating the process that ultimately leads to lung damage, and using less oxygen at resuscitation may ameliorate the problem in preterm babies.
There is evidence from research conducted with term, asphyxiated babies that they can be as effectively resuscitated in air as with 100% oxygen, with no apparent difference in long term outcomes.15–18 There are, however, no studies in preterm infants that have looked at the outcome of this intervention on lung injury.
The aim of this study was to investigate whether lung injury could be reduced in very premature babies by using 50% as opposed to 100% oxygen during resuscitation at birth.
METHODS
This was a randomised controlled trial with factorial design. The interventions compared were the use of either 50% or 100% oxygen as a resuscitation gas at birth and the use of sustained lung inflation for five seconds before the onset of tidal ventilation compared with the currently used two to three seconds of inflation. Comparison of the two oxygen concentrations is presented here.
Block randomisation using sealed envelopes was used. Although consent was obtained earlier, randomisation did not take place until delivery of the baby was imminent.
The primary outcome measure of evidence of pulmonary inflammation was concentration of the cytokines interleukin (IL)6, IL10, IL1β, and tumour necrosis factor α (TNFα) in bronchoalveolar lavage (BAL) fluid obtained at 12 hours of age. Secondary outcome measures included: the severity of initial lung disease determined by blood gas analyses, oxygen and ventilator requirements over the first 24 hours of postnatal life; death; BPD (oxygen requirement at 36 weeks postmenstrual age); major cranial ultrasound abnormality (post-haemorrhagic ventricular dilatation requiring treatment, parenchymal haemorrhage, or cystic periventricular leucomalacia); necrotising enterocolitis (pneumoperitoneum or pneumatosis on abdominal radiograph or confirmed at laparotomy or postmortem examination); retinopathy of prematurity leading to treatment in accordance with national guidelines19 or blindness; a patent ductus arteriosus requiring treatment; systemic infection proven by positive blood culture; pneumothorax requiring chest drain insertion.
Subjects
Babies born at less than 31 completed weeks gestation were eligible for recruitment into the study, but only those who required some degree of resuscitation at birth and had no life threatening malformations were included.
Resuscitation
The resuscitation was conducted on a Vickers Resuscitaire Radiant Warmer (Air-Shields; Hill-Rom, Leicester, UK). This provided the facility to deliver fractions of inspired oxygen and tidal ventilation. The oxygen was preset to be delivered at either 100% or 50% for the duration of the resuscitation until cardiorespiratory stability was achieved and surfactant had been given. It could then be altered at the discretion of the person conducting the resuscitation. Pulse oximetry was not used until the baby arrived on the neonatal unit. The peak inspiratory pressure (PIP) was set at 25–30 cm H2O, and the positive end expiratory pressure at 3–4 cm H2O.
The babies received tidal ventilation during transportation to the neonatal unit on the resuscitaire. At the neonatal unit, they were ventilated using conventional intermittent positive pressure on a time cycled pressure limited SLE 2000 baby ventilator (Specialist Laboratories Equipment, Croydon, Surrey, UK).
BAL fluid
BAL fluid was taken immediately after intubation and stabilisation of the baby at birth before the first dose of exogenous surfactant (0 hours), and the second at 12 hours of age before the second dose of surfactant (12 hours). One person (AEH) performed BAL fluid collection using a standard technique.8,12,20

Median partial pressure of carbon dioxide over first 24 hours in babies receiving 50% oxygen or 100% oxygen.
Cytokine quantification
Cytokines in BAL fluid supernatant were determined with a commercial enzyme linked immunosorbent assay (R&D Systems Europe Ltd, Abingdon, Oxon, UK). The limits of detection for the individual assays were 6.2 pg/ml for IL6, 3.9 pg/ml for IL1β, 62.4 pg/ml for IL10, and 15.6 pg/ml for TNFα. Standards and samples were run in duplicate, and the log of the mean absorbance was plotted. Regression analysis was used to determine the line of best fit from which the cytokine concentrations were read; an r2 of 0.95 and above was considered acceptable. If a sample exceeded the upper limit of the assay, a second sample was diluted and assayed; the results were then multiplied by the dilution factor. The cytokine concentrations are expressed as pg/ml BAL fluid in line with the current recommendations of the ERS task force.21
Statistical analysis
No previously published data were available from which to generate a sample size calculation. We planned a pilot study with a view to using any differences observed between the groups to calculate a sample size for a later definitive study. To show a difference of one standard deviation in any of the continuous variables, we planned to randomise 20 ventilated babies into each group. The Mann-Whitney U test was used for the continuous data, and the χ2 test for categorical data. Two tailed tests were used for all statistical comparisons, and p<0.05 was considered significant. Statistical analyses were performed using SPSS for Windows 10.0.7. (SPSS, Chicago, Illinois, USA).

Median pH over first 24 hours in babies receiving 50% oxygen or 100% oxygen.
Ethical considerations
Informed parental consent was obtained in the antenatal period, and the study had the approval of the local paediatric research ethics committee.
RESULTS
A total of 63 babies were randomised into the study. Fifty two required resuscitation and received the intervention. However, eight of the babies randomised to receive 50% oxygen required a brief increase beyond 50%. Ten babies responded to resuscitation by face mask, and 42 proceeded to intubation. A further four babies were intubated on the neonatal unit. We studied the outcomes of all 52 babies who had received the intervention, although the primary outcome of BAL cytokine concentrations was not available for babies not intubated.
The antenatal history was similar in the two groups: all mothers had received antenatal steroids and all intubated babies received exogenous surfactant (table 1).
Basic and clinical details of babies receiving 50% or 100% oxygen, and cytokine concentrations at 0 hours in both oxygen groups
The median time to intubation was four minutes in the 50% oxygen group and five minutes in the 100% oxygen group. Surfactant was administered by a median time of 12 and 15 minutes respectively. The first BAL fluid was collected as soon as cardiorespiratory stability was achieved and immediately preceded the first dose of surfactant. Randomisation continued until there were sufficient babies intubated to measure the primary outcome of BAL inflammatory markers at 12 hours. Thirty four samples were suitable for analysis at 0 hours and 40 at 12 hours, although there was not sufficient volume of BAL fluid for all babies to permit analysis of all four cytokines at both time points. Table 1 shows the 0 hour BAL fluid cytokine concentrations.
Cytokine concentrations
The interassay coefficient of variation and intra-assay coefficient of repeatability for each cytokine were as follows: IL6, 5.98% and 24.11%; IL1β 1.76% and 19.80%; IL10 16.32% and 33.49%; TNFα 5.93% and 42%.22

Median breaths per minute over first 24 hours in babies receiving 50% oxygen or 100% oxygen.
We found all four cytokines studied present from immediately after birth and at 12 hours of age. However, not all the babies had detectable concentrations of all the cytokines at both time points. Table 2 shows the distribution of cytokine concentrations within the oxygen groups. There were no significant differences in any of the cytokine concentrations between the two groups.
Cytokine concentrations at 12 hours in babies resuscitated in either 50% or 100% oxygen
Ventilator requirements
The only difference found was in the initial PIP, which was slightly higher in the 100% oxygen group immediately after birth (p = 0.02). Otherwise oxygen and ventilator requirements and blood gas analyses were similar in the two groups for the first 24 hours of life. Figures 1–6 show the ventilation and blood gas median results; the ranges are omitted for clarity.

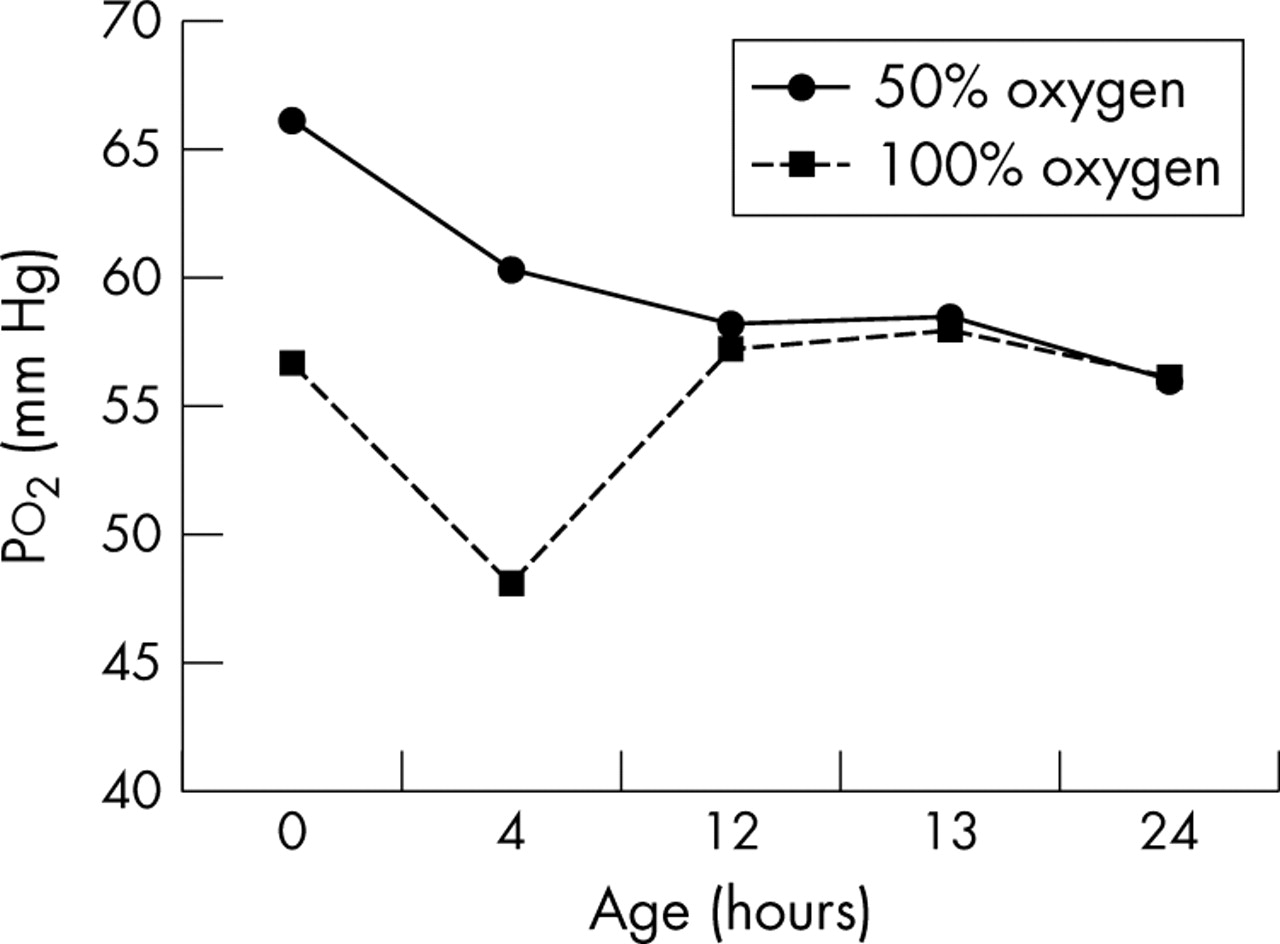
Median partial pressure of oxygen over first 24 hours in babies receiving 50% oxygen or 100% oxygen.

Median peak inspiratory pressure (PIP) over first 24 hours in babies receiving 50% oxygen or 100% oxygen.

{kind=link}
{kind=link}
{kind=link}
Median fraction of inspired oxygen (Fio2) over first 24 hours in babies receiving 50% oxygen or 100% oxygen.
Clinical outcomes
Table 3 shows long term clinical outcomes. There were no significant differences between the groups.
Long term clinical outcomes in babies resuscitated in either 50% or 100% oxygen
DISCUSSION
To our knowledge this is the first study to specifically address the question of whether the amount of oxygen used during the resuscitation of preterm babies affects lung injury. There was no evidence of any difference in lung injury between the two oxygen groups when they were assessed by the BAL fluid cytokine concentrations (table 2), neither did we show a difference in long term clinical outcomes (table 3). However, eight (31%) of the babies from the 50% oxygen group who were difficult to intubate did experience an increase in oxygen concentration at some point during resuscitation, which may have weakened the power of this pilot study to detect a difference. This is a higher number than in a previous study in which babies were randomised to either air or 80% oxygen. Here 26% of the babies in the air group required more oxygen, but concentration did not exceed 50%.23
It may also be that the period of time over which we collected BAL fluid was too short. Had we collected daily sequential BAL fluid samples and for a longer time period, a difference in cytokine concentrations between the two groups may have been evident.
However, given the similarities in the initial course of the respiratory illness and eventual outcome in the two groups (table 3), we think it is unlikely that a reduction of inspired oxygen from 100% to 50% during resuscitation is of any benefit.
The only significant difference in blood gas measurements or oxygen or ventilator requirement between the two groups was in the initial PIP on admission to the neonatal unit: 20 v 18 cm H2O in the 100% and 50% oxygen groups respectively (p = 0.02; fig 4). Clinical practice on our neonatal unit is to set the initial PIP between 18 and 20 cm H2O for babies requiring ventilation because of prematurity until ventilator requirements are confirmed by blood gas analysis. The difference we observed between the two groups is probably a type 1 error.
The question as to whether preterm infants can be effectively resuscitated in less than 100% oxygen and whether using less oxygen would reduce the number of infants who develop BPD has yet to be answered. Current recommendations are still that 100% oxygen be used for resuscitation in this vulnerable group of infants.24 From our study we can only say that the use of 50% oxygen for resuscitation of premature babies appears to be safe, but there is no evidence of benefit, although we cannot exclude a small effect. A study of this size in which the prevalence of death or BPD in the control group was 46% would have only been able to detect a difference of 34% with a sensitivity of 5% and power of 80%.
What is already known on this topic
-
It is well documented that air is as effective as 100% oxygen when used to resuscitate term asphyxiated babies
-
Preterm babies resuscitated with 80% oxygen or air have similar short term outcomes, including a persistent oxygen requirement at 28 days of life
What this study adds
-
No short term benefit was shown from the use of 50% oxygen as apposed to 100% oxygen for resuscitation of the preterm baby at birth
-
The use of 50% oxygen did not adversely affect outcome
CONCLUSIONS
Reducing the amount of oxygen from 100% to 50% for initial resuscitation in preterm babies appears to be safe, although we were unable to detect any difference in either short or long term outcomes, and there was no evidence of increased lung injury in the babies who received 100% oxygen.
RECOMMENDATIONS
Further studies comparing the effectiveness and safety of using lower oxygen concentrations during resuscitation are needed before a change in clinical practice can be recommended.
REFERENCES
Footnotes
-
Published Online First 29 April 2005
-
This research was supported by grants from The Smith & Nephew Foundation, The North West R&D Research Fellowship, and The Newborn Appeal.
-
Competing interests: none declared