Article Text

Abstract
Objective: To determine the feasibility of continuous glucose monitoring in the very low birthweight baby requiring intensive care, as these infants are known to be at high risk of abnormalities of glucose control.
Method: Sixteen babies were studied from within 24 hours of delivery and for up to seven days.
Results: The subcutaneous glucose sensors were well tolerated and readings were comparable to those on near patient whole blood monitoring devices.
Conclusion: Continuous glucose monitoring is practical in neonates, giving detailed information about glucose control.
- CGMS, continuous glucose monitoring sensor
- CI, confidence interval
- VLBW, very low birth weight
- glucose monitoring
- very low birth weight
- prematurity
Statistics from Altmetric.com
Very low birthweight (VLBW, weight <1500 g) babies are at risk of both hypoglycaemia and hyperglycaemia, usually defined in this population as blood glucose <2.6 mmol/l and >10 mmol/l respectively. However, there is a great deal of controversy over what constitutes normoglycaemia in the neonatal population.1 In a retrospective study of 20 VLBW babies admitted to our neonatal unit, we found that nine babies (45%) had documented episodes of asymptomatic hypoglycaemia during the first week of life. However, we also noted that 11 (55%) of these infants had episodes of hyperglycaemia (blood glucose >10.0 mmol/l). This is in keeping with previously published data supporting a prevalence of hyperglycaemia of 20–86% in infants requiring intensive care. Those at the extremes of immaturity and small for gestational age have the greatest risk.2,3 Both hypoglycaemia and hyperglycaemia may be clinically significant, as the former has been associated with poor neurodevelopmental outcome,4 and the latter with osmotic diuresis, electrolyte imbalance, and an increased risk of intraventricular haemorrhage.5
These retrospective data were obtained with current best practice of intermittent blood sampling, “as clinically indicated”, often resulting in many hours between measurements. However, in adults and children with diabetes, continuous glucose monitoring using a subcutaneous sensor has recently been validated and shown to be useful in the management of glucose control, revealing episodes of asymptomatic hypoglycaemia and hyperglycaemia.6–8 In these patients the sensor (which is described below) is well tolerated.6,7 The use of continuous glucose monitoring has not previously been reported in the neonatal period in VLBW babies. We aimed to assess the practicalities and validity of a continuous glucose monitoring device in the VLBW neonate and to obtain more data on the prevalence of hypoglycaemia and hyperglycaemia in this population.
METHOD
Cohort characteristics
Sixteen babies (nine male) requiring intensive care and born <1500 g were recruited from Addenbrooke’s Hospital NHS Trust, Cambridge and Luton and Dunstable Hospital NHS Trust. The infants had a median (range) gestational age of 26.5 weeks (23.3–29.9), birth weight 706 g (584–1387), and birth weight standard deviation score (SDS) −0.435 (−2.95 to −0.49). All infants were recruited within 24 hours of delivery and monitored for up to seven days. Approval was obtained from both Addenbrooke’s Hospital and Luton and Dunstable Hospital ethics committees, and written informed consent was obtained from all parents before participation.
The continuous glucose monitoring sensor (CGMS)
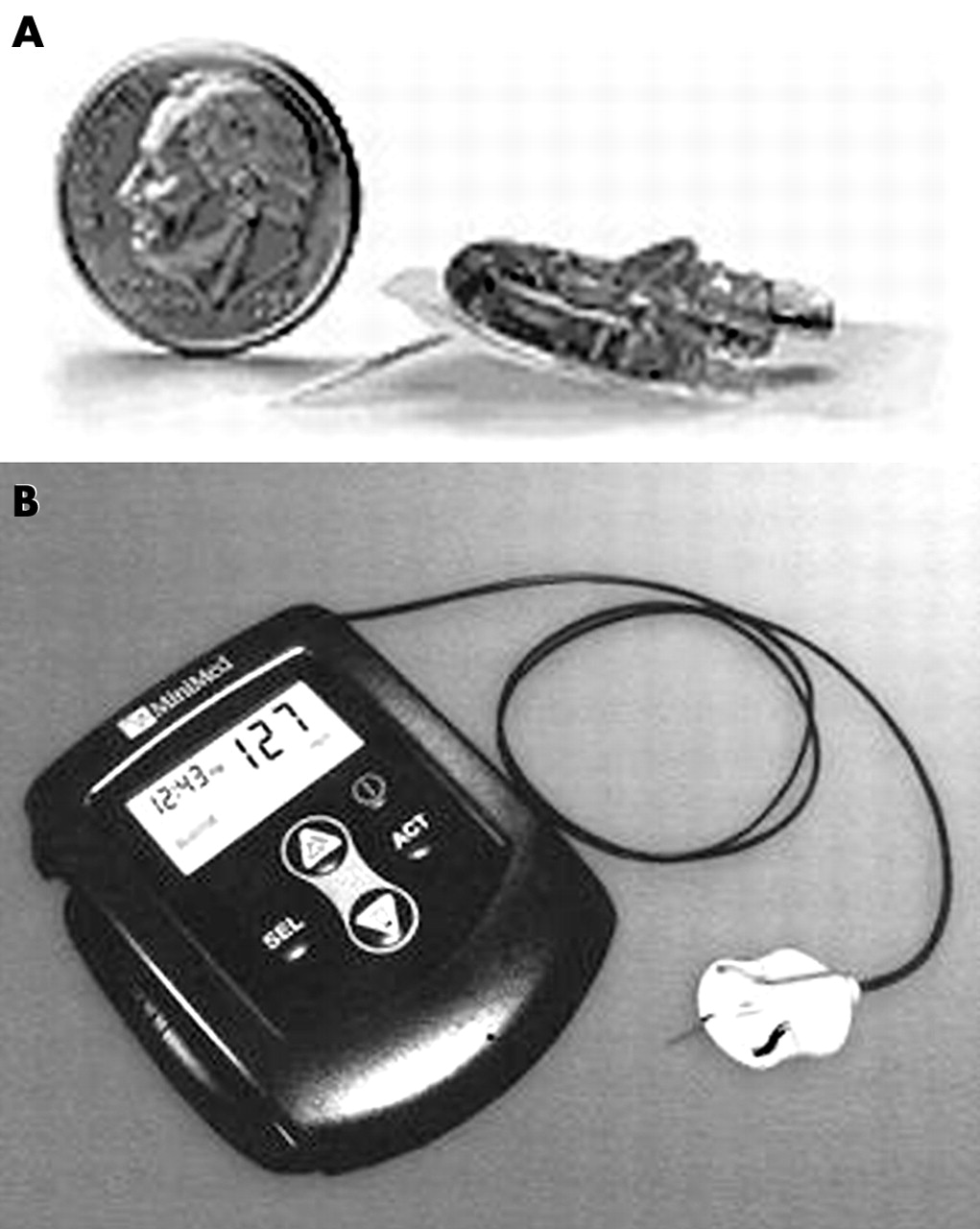
The CGMS (fig 1) comprises a disposable, glucose oxidase based, platinum electrode sensor which catalyses interstitial glucose oxidation generating an electrical current every 10 seconds, which is recorded via a cable by a pager sized monitor (6 × 9 × 2 cm). Although the sensor measures the concentration of interstitial glucose every 10 seconds, the monitor records averaged values every five minutes, giving a total of 288 readings a day, and is considered “continual”. Glucose concentrations outside the range 2.2–24 mmol/l (40–430 mg/dl) were reported as <2.2 mmol/l (<40 mg/dl) or >24 mmol/l (>430 mg/dl) respectively. The data cannot be viewed in real time, and therefore did not impact on clinical care. Nursing and medical staff were instructed in the use of the CGMS and were asked to enter all blood glucose measurements taken for clinical reasons using near patient monitoring devices into the CGMS for calibration. The Elite (Bayer, Munich, Germany) and Medisense (Abbott, Abbott Park, Illinois, USA) near patient glucose monitors were used.
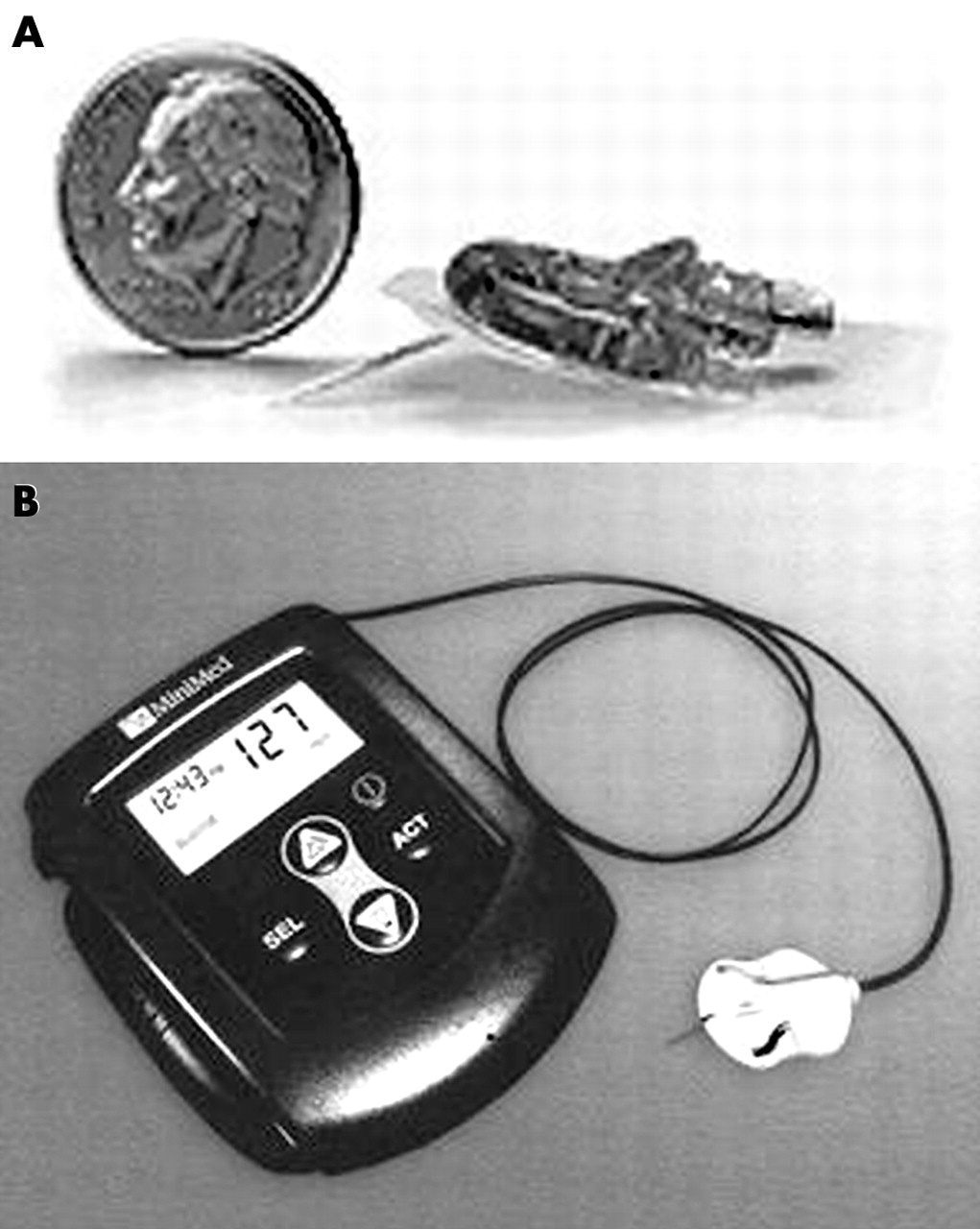
(A) Minimed sensor shown with an American nickel (20 mm diameter) for size comparison. (B) Continuous glucose monitoring sensor (CGMS) monitor with sensor attached (monitor size: 6 × 9 × 2 cm). Reproduced with permission from Medtronic Limited (Sherbourne House, Croxley Business Centre, Watford, UK).
The Minimed sensor (Medtronic, Northridge, California, USA) was sited in both centres by the same investigator (KB). It was inserted by hand (the manufacturer’s insertion device was not used) into the subcutaneous tissue of the lateral aspect of the thigh using an aseptic technique.
Insertion technique
The legs were examined to find an area of unbroken skin, the skin was cleaned with sterile water, and a fine spray of Cavilon (3M Health Care, Borken, Germany) was applied if the skin appeared particularly friable. The sensor is soft and flexible, about 1 mm in width by 10 mm in length, and mounted inside a hollow needle to allow subcutaneous insertion. Although the sensors are manufactured with a white adhesive backing, this was cut in half to minimise the area of infants skin exposed to adhesive. The insertion technique comprised holding the leg firmly, pinching the skin and muscle of the thigh between thumb and forefinger, and angling the introducer parallel to the skin to ensure superficial insertion in the subcutaneous tissues. Once the sensor was inserted, the needle/introducer was withdrawn and the sensor attached to the skin by the white adhesive backing. The sensor was then secured with steristrips and a clear occlusive dressing (again trimmed to ensure minimal contact with the neonate’s skin), so that the insertion site could be inspected daily. There was occasionally a very small amount of serous ooze or a small amount of blood at the insertion site, but this settled quickly and was not clinically significant. A couple of steristrips were also used to anchor the leads from the monitor to the baby’s lower leg to avoid displacement. Infants tolerated the procedure well, with minimal apparent discomfort.
Removal
At the end of the study period, the dressing was gently peeled off the thigh and the sensor withdrawn. There were no problems with bleeding at the site. The site appeared clean and dry in all babies, with a small puncture hole visible at the insertion site which healed quickly. As the sensor lies in the subcutaneous tissue, accidental displacement did not cause any problems.
Some infants required replacement of the sensor either because of dislodgement or because the electrode signal became inadequate. However, the sensor was only replaced on a single occasion in any baby. A single blood sample was taken each day for comparison of sensor value with blood glucose measured using laboratory glucose oxidase methods (Yellow Springs Instruments, Yellow Springs, Ohio, USA; YSI). Standard neonatal care with regard to blood glucose comprised interventions only if blood glucose fell to <2.6 mmol/l on any occasion, or was >10.0 mmol/l on more than two occasions.
Statistical analysis
Hypoglycaemia was defined as a subcutaneous sensor glucose value <2.6 mmol/l, and hyperglycaemia as >10 mmol/l. The prevalence of both hypoglycaemia and hyperglycaemia for each subject was defined as the percentage of studied time spent hypoglycaemic or hyperglycaemic. The Bland-Altman method was used to assess the agreement between blood glucose concentrations obtained with the CGMS and both conventional glucose meters and YSI laboratory samples. Correlation between the different methods was determined by linear regression. Weight standard deviation scores were calculated using the reference data based on the British 1990 growth reference and Cole’s LMS method supplied by the Child Growth Foundation.
RESULTS
Safety
The CGMS was well tolerated. Babies did not make any attempts to pull at either the sensor or the lead, and it did not compromise nursing care. In one baby of 23 weeks gestation, in whom 50/50 paraffin had been used because of very poor skin condition, the sensor fell out on two occasions and was therefore not replaced. In another baby (24 weeks gestation) a small area of superficial skin loss was noted 24 hours after sensor removal, but this healed well. There was no evidence of local oedema, inflammation, or infection at the sensor sites in any baby.
Comparison of data from CGMS and conventional meters
Paired glucose readings from the CGMS and the Elite (n = 516), taken from 16 babies, correlated significantly (r2 = 0.87, p<0.001). For all data, mean glucose difference between the MiniMed sensor and near patient monitoring was −0.06 mmol/l (95% confidence interval (CI) –2.94 to –2.82)—that is, the CGMS reading was a mean of 0.06 mmol/l lower than that of near patient monitoring devices (fig 2A). Although there was good agreement below 10 mmol/l at higher glucose levels (n = 96), the correlation was not as good (r2 = 0.69, p<0.001), and the mean glucose difference rose to −0.106 mmol/l (95% CI –4.3 to −4.25). There were insufficient paired values <2.6 mmol/l to allow comparison. We also compared paired sensor readings (n = 56) and paired near patient measurements (Elite monitor n = 72) with the YSI laboratory measurements (fig 2B,C). We found the sensor to show a mean difference of 0.29 mmol/l (95% CI –5.55 to −6.13), and the Elite a mean difference of 0.36 mmol/l (95% CI –4.38 to –5.1), when compared with the YSI laboratory measurements. Ten infants contributed data on sensor versus plasma glucose comparisons. Although the numbers of subjects are relatively small, in covariate analysis we did not see any evidence at all for interindividual variation in the sensor versus plasma glucose regression line, for the constant (p>0.9) or the slope (p>0.9).

{kind=link}
{kind=link}
Bland-Altman plots. (A) Comparison of sensor data with near patient monitoring device, showing 95% confidence interval (CI) limits (± 2SD). Mean glucose difference = −0.06 (95% CI –2.94 to –2.82). Difference (mmol/l) refers to continuous glucose monitoring sensor (CGMS) minus near patient monitoring device. (B) Comparison of sensor with Yellow Springs Instrument (YSI) laboratory glucose measurements. Mean glucose difference = 0.29 mmol/l (95% CI ± 2 D –5.55 to −6.13). (C) Comparison of near patient monitoring with YSI laboratory glucose measurements. Mean glucose difference = 0.36 mmol/l (95% CI ± 2SD –4.38 to −5.1). (D) Comparison of sensor data with near patient monitoring device at glucose concentrations of <10 mmol/l.
Characteristics of glucose control
A total of 1302 hours of data were reviewed from eight babies receiving standard care. This represents a median of 163 hours per patient (range 126–180 hours). Over this period, median (range) percentage time hypoglycaemic was 0.4% (0–11%). All episodes were asymptomatic, and three babies had episodes that were undetected clinically. In one baby, hypoglycaemia was recorded on the sensor 2 hours 45 minutes before a blood glucose being taken, which then confirmed hypoglycaemia. The median (range) of time hyperglycaemic during the study period was 36% (0–53%), peaking on day 3 (43%). This was in the context of a mean (SD) daily dextrose infusion rate of 9.18 (2.48) mg/kg/min. With small numbers, we were unable to comment on relative risk because of prematurity or size.
DISCUSSION
We have evaluated the use of the MiniMed continuous glucose monitor in the VLBW neonate requiring intensive care. It appears to be safe to use in this population, and it remains effective if left in situ for up to seven days, which is twice the length of time that the sensors tend to last in older paediatric patients. It is well tolerated after insertion in the thigh, with infants settling quickly and appearing to be unconcerned by its continued presence throughout the study period. It does not interfere with nursing care. Although we had concerns about attachment to babies with very delicate skin there was no evidence of significant tissue damage after placement for seven days or after the sensor was accidentally dislodged. Some of the babies had suspected sepsis during the study period, as would be expected in this high risk group, who also all had central lines in situ. However, as the sensor site did not show any signs of inflammation, and the sensor lies subcutaneous not intravenous, we do not feel that it was likely to be responsible for these episodes. However, a much larger study would be needed to be sure that there is no increased risk of infection.
The device measures interstitial rather than blood glucose, and, in two babies who had particular problems with oedema, the sensor was noted to have periods when no measurement was recorded. As there is considered to be a standard difference of 1.11 between plasma and blood glucose, one might expect the interstitial sensor to under-read. However, the device is calibrated to any blood glucose concentrations entered into the monitor during the study period, and therefore results can be interpreted as equivalent to blood glucose concentrations.
The sensor readings have wide confidence intervals, particularly at higher blood glucose concentrations. This is not of great importance at high concentrations—the difference between a blood glucose of 10 and 12 mmol/l is not clinically significant—but there would be difficulties in relying on sensor values at low concentrations of blood glucose. We had only a limited number of blood glucose values at the lower end of the monitor’s range, and therefore it is difficult to comment on the accuracy of the monitor in detecting hypoglycaemia. We hope to address this clinically significant issue by targeting patients at risk of hypoglycaemia, such as those with metabolic or endocrine disorders undergoing controlled fasts.
However, current near patient monitoring devices also have wide confidence intervals especially at low readings, as shown by our comparisons of the Elite reading with YSI laboratory values. The sensor, however, has the advantage of continuous data acquisition, and, although the device used for this study did not give a real time read out, new monitors in development do have real time read outs and will have variable alarm settings. These monitors are due to be available in 2005.
From a research perspective, monitors without real time read outs have the advantage of providing blinded data on glucose control in populations at risk of both hypoglycaemia and hyperglycaemia. However helpful this blinded information may be in terms of long term management of individuals, there are ethical issues in obtaining such blinded information if intervention could be beneficial to a patient.
The development of monitors with real time read outs has the potential to significantly improve the clinical management of glucose control in intensive care patients. However, from these data, the wide confidence intervals mean clinicians should not rely solely on these monitors for making decisions about clinical care. With an averaged value every five minutes and alarm settings, clinicians may be alerted to the need for a sample to be taken to check the blood glucose concentration. This would provide clinicians with the ability to optimise the management of glucose control without the need for frequent blood sampling, allowing minimal handling and disturbance of babies and less frequent access to central lines. Pre-emptive management with alteration in delivery of dextrose, total parenteral nutrition, or insulin may avoid the problems of both hyperglycaemia and hypoglycaemia.
It is well known that VLBW infants are at risk of both hypoglycaemia and hyperglycaemia during the first week of life. The data from the CGMS during this study were not available to the clinicians in real time and therefore could not affect management. However, during this study we found there were often prolonged periods (sometimes up to 12 hours) between near patient blood glucose measurements. The CGMS data were important in that they revealed periods of clinically undetected hypoglycaemia and highlighted delays of up to 2 hours 45 minutes between hypoglycaemia being registered on the sensor and being detected clinically and appropriate management being undertaken. This may be clinically important, as asymptomatic hypoglycaemia is associated with both acute neurophysiological abnormalities9 and later neurodevelopmental impairment.4
We have shown that the CGMS is practical for glucose monitoring in the VLBW infant and that both hypoglycaemia and hyperglycaemia are prevalent in this population. Although there is no universally agreed management, it is now increasingly considered that both hypoglycaemia and hyperglycaemia are potentially harmful to these vulnerable patients. New CGMSs with alarm settings could help in guiding management of glucose control in this population, and in the future tighter glucose control may prove beneficial in the sick VLBW infant.
Acknowledgments
We thank the families and staff from both neonatal units, Medtronic MiniMed (Croxley Business Park, Watford) for supplying the sensors, and SPARKS for funding a fellowship for KB.
Footnotes
-
Competing interests: Medtronic supplied the CGMS monitors
Linked Articles
- Fantoms