Article Text

Abstract
Aim: To evaluate the changes in the osmolality of expressed breast milk (EBM) after the addition of seven additives and four proprietary fortifiers commonly used during neonatal intensive care.
Methods: The osmolality of 5 ml EBM was measured with increasing doses of 6% NaCl, caffeine, sodium ironedetate, folic acid, and multivitamin drops. Sodium acid phosphate and chloral hydrate were added to 8 ml EBM, and the fortifiers were added to standard volumes of EBM. Dose-effect curves were plotted, and the volume of milk that must be added to the above additives to maintain osmolality below 400 mOsm/kg was calculated.
Results: The osmolality of the pure additives ranged from 242 to 951 mOsm/kg. There was a significant increase in the osmolality of EBM with increasing doses of all additives except caffeine. The osmolality of EBM with many additives in clinically used dosages potentially exceeded 400 mOsm/kg. The greatest increase occurred with sodium ironedetate syrup, where the osmolality of EBM increased to 951.57 (25.36) mOsm/kg. Proprietary fortifiers increased the osmolality of EBM to a maximum of 395 mOsm/kg.
Conclusion: Routine additives can significantly increase the osmolality of EBM to levels that exceed current guidelines for premature infant feeding. A simple guide for clinical use is presented, which indicates the amount of milk required as diluent if hyperosmolality is to be avoided.
- expressed breast milk
- osmolality
- fortifiers
- necrotising enterocolitis
Statistics from Altmetric.com
Breast milk is the first choice for feeding preterm infants. The nutritional and immunological superiority of breast milk gives short term benefits1,2 and possible improved long term outcomes such as neurodevelopment3 and lower blood pressure.4 However, in neonatal practice, various additives are routinely combined with expressed breast milk (EBM) for therapeutic or nutritional benefit. These additives have the potential to increase the osmolality of EBM. The administration of hyperosmolar feeds is thought to be associated with necrotising enterocolitis.5–7 This concern led to recommendations that enteral feeds for neonates should not have osmolality above 400 mOsm/kg,8 and so any intervention that increases the osmolality of EBM may be counterproductive.
White and Harkavy9 first recognised that the addition of medication to formula milk increased the osmolality by up to 300%. Ernst et al10 measured the osmolality of both oral and intravenous preparations of 63 drugs and infant formulas. They confirmed that additions to formula milk significantly increased the osmolality of enteral feeds and showed that many of the drugs intended for oral administration induced increase in the osmolality of feeds that was 3 to 4 times higher than their corresponding intravenous preparations.
However, the available data do not give guidance on the osmolar effect of therapeutic and nutritional additions to EBM. The aim of this study was therefore to determine the effects of commonly used additives, drugs, and fortifiers, on the osmolality of EBM. We suggest a simple format that indicates the volume of milk needed as solvent to prevent the osmolality of EBM exceeding 400 mOsm/kg in clinically relevant doses of additives.
METHODS
This study was approved by The Hammersmith Hospital Trust research ethics committee. Seven samples of EBM, from seven different mothers, which were otherwise to be discarded were collected from Queen Charlottes and Chelsea Hospital Milk Bank, where they had been kept frozen at −20°C. The osmolality of each of these milk samples alone and with increasing doses of a series of additives were evaluated: 6% NaCl (Sterile Fluids Unit (SFU), Edgware General Hospital, London, UK) containing 1 mmol sodium in 1 ml; sodium acid phosphate (SFU, Edgware General Hospital) containing 0.9 mmol phosphate and 1.5 mmol sodium in 1 ml solution; caffeine (SFU, Edgware General Hospital) containing 10 mg in 1 ml; Dalavit (Eastern Pharmaceuticals, Coomb House, Isleworth, Middlesex, UK), a multivitamin preparation, 0.6 ml containing vitamin A (palmitate 5000 units), vitamin B (thiamine hydrochloride 1 mg, sodium phosphate riboflavin BP 0.4 mg, pyridoxine hydrochloride BP 0.5 mg, nicotinamide B.P 5 mg), vitamin C (ascorbic acid BP 50 mg) and vitamin D (ergocalciferal BP 400 units); sodium ironedetate syrup (Link Pharmaceutical Ltd, Horsham, Sussex, UK), containing 5.5 mg elemental iron in 1 ml, and folic acid syrup (Pharmacy Department, Hammersmith Hospitals NHS Trust) containing 2.5 mg in 5 ml; chloral hydrate (Pharmacy Department, Hammersmith Hospitals NHS Trust) containing 200 mg per 5 ml.
The osmolality of EBM containing appropriate doses of four proprietary human milk fortifiers was also measured: Nutriprem breast milk fortifier (one sachet in 50 ml); SMA breast milk fortifier (one sachet in 50 ml); Enfamil human milk fortifier (one sachet in 25 ml); Eoprotin (3 g in 100 ml).
Osmolality was determined from freezing point depression (Advanced TM microosmometer model 3300). The instrument was calibrated with aqueous NaCl. When the osmolality exceeded 3000 mOsm/kg, the substance was diluted 1:10 with distilled water. All measurements were performed in duplicate and averaged. If the difference was more than 2 mOsm/kg, a third measurement was taken and the two closest readings were used.
All the additives were added to 5 ml aliquots of EBM in increasing doses within the normal therapeutic range. The sodium acid phosphate solution was added to 8 ml aliquots of EBM, and chloral hydrate was also added to 8 ml EBM because of its viscosity; the osmolalities were then extrapolated to 5 ml EBM. Dose-effect curves with 95% confidence interval were constructed by least squares linear regression analysis (Sigma Plot version 8.0: Jandel Scientific, San Rafael, California, USA). The volume of the EBM required to avoid an osmolality greater than 400 mOsm/kg when typical clinical doses were added was calculated for each additive.
RESULTS
Table 1 gives the osmolality of the additives alone and in combination with a standardised volume of EBM (5 ml). Figure 1 shows dose-effect curves for each additive on the osmolality of EBM (8 ml in the case of sodium acid phosphate and chloral hydrate and 5 ml in the case of all other additives). Table 2 gives the osmolality of proprietary milk fortifiers added to standard volumes of EBM.
Osmolality of each additive alone and in combination with a standardised volume (5 ml) of expressed breast milk (EBM)
Osmolality of expressed breast milk (EBM) with addition of proprietary fortifiers

Osmolality of expressed breast milk with increasing doses of nutritional additives showing least squares linear regression and 95% confidence intervals.
Osmolality increased with increasing doses of all additives except for caffeine, where the osmolality decreased with higher doses. The maximum increase in osmolality of EBM with the addition of a therapeutic dose occurred with chloral hydrate, where the osmolality increased to 1382.6 mOsm/kg. The addition of proprietary fortifiers to EBM did not increase the osmolality above 400 mOsm/kg.
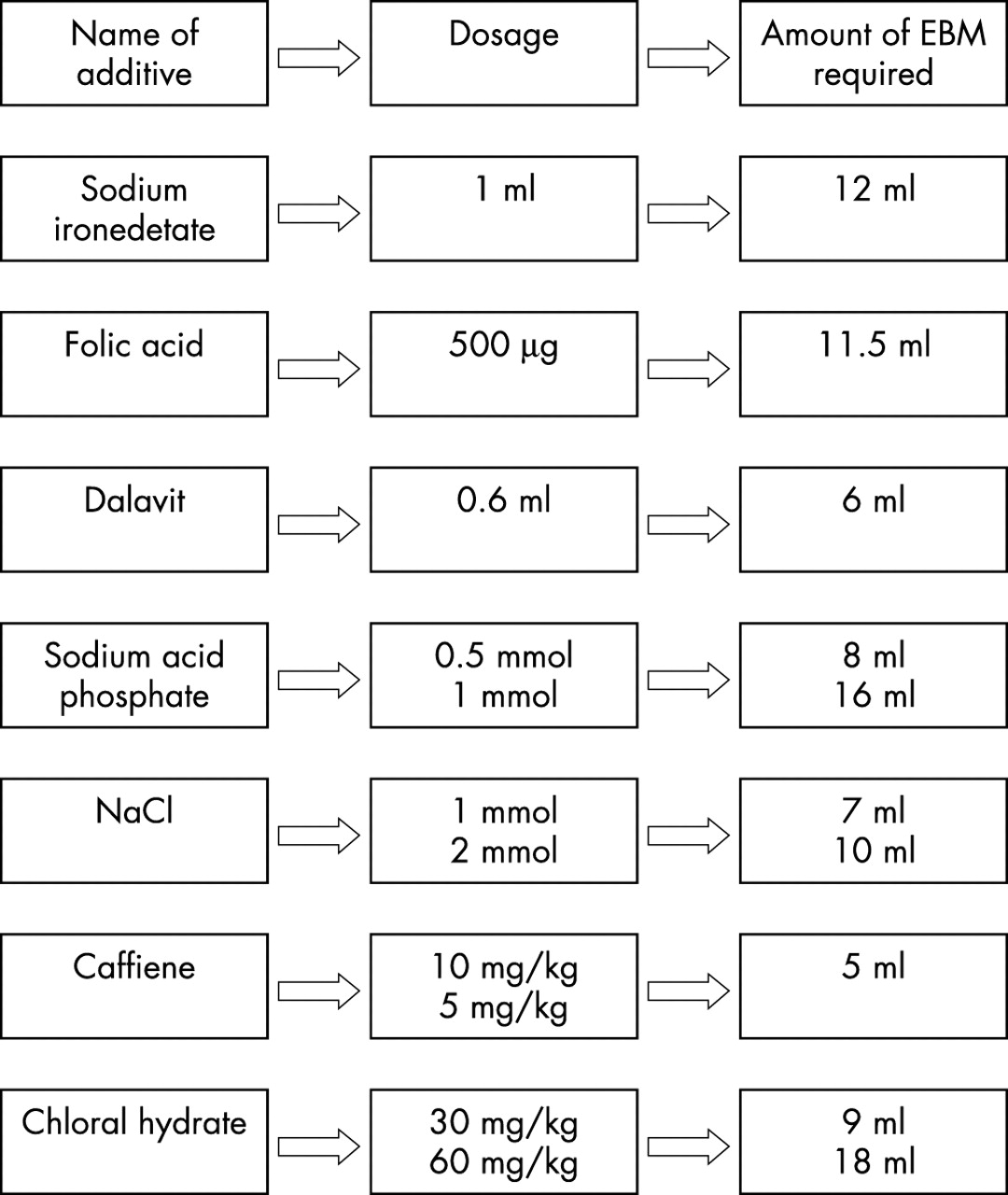
Figure 2 gives a simple chart depicting the minimum amount of milk required for the dilution of commonly administered doses of additives if the osmolality is to remain below 400 mOsm/kg.

{kind=link}
{kind=link}
Amount of expressed breast milk required as solvent to maintain osmolality below 400 mOsm/kg.
DISCUSSION
This study shows that modification of EBM with therapeutic doses of commonly used additives can result in a significant increase in its osmolality. It is important to note that this study also suggests that the osmolality of EBM could be further worsened by the use of drugs and nutritional supplements in combination with fortified EBM.
White and Harkavy9 and Ernst et al10 noted high osmolality when certain drugs were added to formula feeds, largely due to the vehicle used in oral preparations, and previous studies have also evaluated the osmotic changes of breast milk with added fortifiers.11,12 However, this study indicates that hyperosmolality can be avoided by the simple measure of dilution in sufficient volumes of EBM.
The osmolality of a solution can be described by the equation

where as is the effective concentration, fs is the activity coefficient, and Cs is the analytical concentration. The effective concentration of the solute is due to the interactions of its molecules and ions with each other and water molecules, which in turn affects the colligative properties, such as freezing point depression. Hence ionic compounds such as NaCl, which dissociates into two ions for each molecule, exert more osmotic pressure.
As expected, for most substances the osmolality rose with increasing concentration of the additive, but with caffeine the opposite happened. This may be explained by certain physical properties of caffeine, such as increasing association equilibrium with increasing concentration and, being an organic compound, it does not dissociate into two or more ions. The decrease may also be related to the dilution effect.
Dose-response curves for different concentrations of fortifiers are not available in this study. The carbohydrate concentrations of fortifiers have recently been increased, leading to further concerns about the risk of necrotising enterocolitis. It is important to note that this study was performed with previously used fortifiers. There have also been concerns about the refrigeration of EBM with fortifiers and the resultant increase in osmolality.11,12 In this study, the measurements were performed immediately after the addition of the fortifiers to EBM, as recommended.
The risks of hyperosmolar solutions to neonatal intestine have been documented in both animal and human studies.5–8,13 As the fetal gut is exposed to the amniotic fluid which has an osmolality of about 275 mOsm/kg and the osmolality of human milk is similar, there is concern about the administration of enteral feeds with significantly higher osmolalities because of the risk of necrotising enterocolitis. In the light of these concerns, recommendations have been made that enteral feeds for neonates have osmolalities no greater than 400 mOsm/kg.8
The use of EBM lowers the incidence of necrotising enterocolitis,14,15 and may improve neurodevelopment2 and lower blood pressure.3 It is postulated that the effects of the growth factors, trophic factors, and immunological factors of EBM on the intestine are responsible. It therefore seems appropriate to use breast milk, but maintain a low osmolality to avoid any risk of reducing these beneficial factors. Rational policies for the use of additives will allow this, and the chart provided in fig 2 suggests an approach that neonatal units could use to simplify safe additive administration.
Acknowledgments
Our thanks go to the nurses of the Neonatal Unit, Queen Charlottes and Chelsea Hospital for suggestions on the chart and to Dr M Ajayi-Obe and Ms Oonagh Prendiville, Principle Biochemist BSc SRCS, for technical assistance.