Article Text

Abstract
Hypotension occurs in up to 20% of very low birthweight infants, usually in the first 48 hours after birth. Its importance lies in its possible causal link with brain injury. Its management is controversial.
- hypotension
- inotropes
- tissue perfusion
- very low birthweight
- VLBW, very low birth weight
- NIRS, near infrared spectroscopy
Statistics from Altmetric.com
Every paediatrician working on a neonatal unit will have treated the very low birthweight (VLBW; < 1500 g) infant with hypotension. Hypotension, however defined, occurs in up to 20% of VLBW infants, most commonly in the first 48 hours after birth. Its importance lies in its possible causal link with brain injury in these infants.1–4 The common dilemma is when to treat, and how.
There are numerous controversies surrounding the management of hypotension in the VLBW infant. Firstly, the definition of hypotension varies, particularly at the extremes of prematurity. Secondly, the method of monitoring blood pressure is also variable; in particular, the value of non-invasive assessment remains open to debate. Thirdly, the causes of hypotension and its effect on prognosis in these babies is not proven. Lastly, treatment remains prone to personal preference, as it has not been as extensively studied as one might expect.
This article reviews the definition of hypotension, its clinical relevance, and the available treatments, including volume support, inotropes, and steroids.
DEFINITION
Normal blood pressure has proved difficult to define in preterm babies, partly because it varies with gestational and postnatal age,5,6 but also because the range of blood pressure that will ensure adequate organ perfusion is not known. A few studies have attempted to define the normal range of blood pressure in the neonate.1,5–8 These have resulted in two widely accepted definitions of hypotension:
-
Mean arterial blood pressure less than the 10th centile for gestation/birth weight and postnatal age1
-
Mean arterial blood pressure less than gestational age in weeks. This is derived from the first definition, after the observation that the 10th centile for mean blood pressure is roughly equal to the gestational age. It is worth remembering, however, that this is only valid in the first 48 hours of life.5
MEASUREMENT
Monitoring of intra-arterial blood pressure through an umbilical or peripheral arterial catheter is widely accepted as the optimum method. Several studies have compared oscillometric with invasive measurement. Provided that cuff size is standardised, oscillometric measurement seems to be accurate within the normal range.9,10 However, concern has been expressed that, at the lower levels, it consistently overestimates the blood pressure, providing false reassurance.11 We refer the reader to articles that have explored this issue in more detail.9–12
CLINICAL RELEVANCE
Tissue perfusion
In neonatology, blood pressure is regularly used as a marker of systemic organ perfusion. Unfortunately, there are few data to support this. Kluckow and Evans13 showed that there is only a weak correlation between blood pressure and cardiac output in preterm infants. Furthermore, as blood pressure is the function of blood flow and systemic vascular resistance, blood pressure may not reflect the blood flow in end organs, as the vascular resistance will vary. Several methods that may be useful for assessing systemic blood flow and tissue perfusion in neonates are being evaluated.
Left ventricular output is often used in adults to assess systemic blood flow. Measurements of ventricular outputs in neonates may be confounded by shunts through a patent ductus or foramen ovale. Kluckow and Evans14 successfully measured systemic blood flow in the superior vena cava of newborn infants, using Doppler echocardiography. Flow in the superior vena cava was chosen to represent blood flow in the upper body, particularly the brain, and correlated well with left ventricular output in babies with a closed duct.
Wardle et al15 used near infrared spectroscopy (NIRS) to measure haemoglobin flow and venous saturation in the forearm of hypotensive preterm babies. From this they were able to calculate oxygen delivery and consumption and fractional oxygen extraction. They found that peripheral oxygen delivery and consumption were lower in hypotensive babies, but that oxygen extraction was similar to normotensive controls. There was also no rise in lactate concentration. The results suggest that in hypotensive babies, peripheral oxygen delivery is still adequate for tissue demands, challenging the need to routinely correct hypotension. Tsuji et al16 used NIRS to monitor cerebral circulation in sick premature infants. They showed a direct relation between mean arterial blood pressure and cerebral intravascular oxygenation. However, in a further study by Wardle et al,17 there was no relation between hypotension and cerebral fractional oxygen extraction, suggesting that sufficient oxygen is delivered to meet demand even in the presence of hypotension.
As NIRS and cardiac output measurements are not continuous, their role in the decision to treat a blood pressure level remains unclear. They do, however, question our present practice of using a single value below which treatment should be started.
Gastric intramucosal pH (tonometry) has been measured as a reflection of gut perfusion, which may be of value in assessing overall tissue perfusion. Campbell et al18 showed a relation between gastric intramucosal pH and blood flow in the superior mesenteric artery of newborn piglets. In a study in VLBW infants, the same team also found that intramucosal pH was independently predictive of major gastrointestinal complications in VLBW infants.19 These results suggest that gastric tonometry may be a useful, relatively non-invasive method of evaluating tissue perfusion in preterm infants.
Further research in this area is obviously needed before techniques such as this have direct relevance to the management of hypotension. Until this is available, it would seem important that a blood pressure level should not be the only criterion in determining when to treat, and that other markers of systemic perfusion, such as metabolic acidosis, capillary refill time, urine output, and peripheral temperature should also be considered. These additional clinical parameters of cardiovascular status are not proven to be of value in determining end organ perfusion in newborn infants.20,21 However, at present they are the only easily repeatable additional assessments, and are used by many clinicians in deciding an individual patient’s “hypotensive level”.
Cerebral injury
It is well documented that sick VLBW infants have reduced cerebral vascular autoregulation compared with term infants,22,23 with the postulated effect that severe hypotension may lead to cerebral hypoperfusion. Hypotension has been linked to cerebral haemorrhage and ischaemia in many studies. Watkins et al1 found that hypotension was strongly associated with intraventricular haemorrhage, but not with periventricular ischaemic lesions. Hypotension is thought to lead to intraventricular haemorrhage by causing ischaemic damage to the germinal matrix, which bleeds on reperfusion. It is unlikely that overenthusiastic correction of hypotension is involved, as episodes of hypertension in this study were not associated with the occurrence of intraventricular haemorrhage. A review of recent studies by Dammann et al3 supports the finding of Watkins et al that systemic hypotension does not, in itself, lead to periventricular leucomalacia. There is also evidence to link episodes of hypotension in the neonatal period to long term neurological sequelae. In a study of 98 premature babies, Low et al4 found that sustained hypotension and hypoxaemia, in the first four days after delivery, increased the probability of a major adverse neurodevelopmental outcome from 8% to 53%. Interestingly, there is little evidence to support the view that treating hypotension prevents these sequelae.
MANAGEMENT
The aim of treating hypotension is to preserve adequate organ perfusion and thus to prevent complications such as cerebral injury. However, a cause for hypotension should always be sought before treatment is instituted. Important conditions to exclude include:
-
Blood loss
-
Pneumothorax
-
Sepsis
-
Patent ductus arteriosus
-
High positive intrathoracic pressure (secondary to mechanical ventilation)
-
Heart failure
If one of the above causes is identified, the primary treatment of the hypotension is to institute the specific treatment for the underlying condition. In most instances, a cause for hypotension in the neonatal period will not be determined, although myocardial dysfunction has been identified as a common factor in,24 and treatment will be initiated on the basis of unit protocols. These normally follow a stepwise approach beginning with volume support followed by inotropes and, in some, the use of steroids.
Volume support
It is generally accepted that hypovolaemia is an uncommon cause of hypotension in the sick preterm infant.25 It is also difficult to diagnose in the immediate postnatal period, as indicators such as urine output and capillary refill time are unreliable. However, because it does occasionally occur, and is relatively easy to treat, most units adopt a policy of moderate volume replacement before the institution of inotropes.
Fluids available for volume replacement may be either crystalloid or colloid. The main difference between the two is the oncotic pressure effect, according to Starling’s law, and the theoretical difference in the length of time they stay in the intravascular space.
Emery et al26 looked at the protein content of solutions used to treat hypotension, and found that volume appeared to be more important than protein content in producing a sustained increase in blood pressure. More recently, King et al27 showed that isotonic saline is as effective as 5% albumin for treating hypotension in preterm infants. Furthermore, they found an additional advantage, in that saline caused less fluid retention, in the first 48 hours of life, than albumin. This was thought to be due to the high capillary leak of plasma proteins into the interstitial space, resulting in interstitial oedema.
There are, of course, other advantages of crystalloid over colloid, which should be considered.
-
Colloids are blood products and therefore carry an infection risk
-
The cost of isotonic saline is about one-fiftieth of that of 4.5% human albumin solution
In summary, it seems that colloid and crystalloid are equally effective in treating hypotension in the neonatal period. Considering the other advantages of using isotonic saline, it would seem that the safest approach to volume replacement would be to use 10–20 ml/kg 0.9% saline given over 30 minutes in the first instance. The use of 4.5% albumin should be reserved for babies who are likely to be hypovolaemic secondary to protein-losing conditions, such as those who have had gastrointestinal surgery.
Dopamine and dobutamine
Most neonatal intensive care units support the use of dopamine and dobutamine as inotropic agents in the treatment of hypotension. Their use, however, is historically based rather than evidence based, and there are few data relating to associated mortality and morbidity.
There is evidence that myocardial dysfunction plays an important role in the development of hypotension in preterm infants in the first few hours of life.24 It is therefore clear that inotropic agents should be of some benefit in the management of hypotension in these babies.
In a study comparing early use of dopamine infusion to volume expansion with plasma protein fraction, Gill and Weindling28 showed that dopamine was more effective in restoring normal blood pressure. In fact, this study supported the initiation of treatment with dopamine without waiting for a response to volume expansion.
Dopamine is a sympathomimetic amine which exerts its cardiovascular effects through dopaminergic and α and β adrenergic receptors. It is thought to exert up to 50% of its inotropic effect through an indirect action on β2 adrenoceptors, stimulating the release of endogenous noradrenaline.29
There have been several studies into the pharmacokinetics and mechanism of action of dopamine in the preterm infant. Roze et al30 showed a dose dependent increase in mean arterial blood pressure with dopamine infusions of 5–20 μg/kg/min. The increase in blood pressure in this study was attributed to an increase in systemic vascular resistance, but not in left ventricular output. Padbury et al31 showed a dose dependent increase in myocardial contractility and resulting cardiac output at dopamine doses of 1–8 μg/kg/min, without significant changes in systemic vascular resistance or heart rate. Seri et al32 have shown that, at doses of 2.5–7.5 μg/kg/min, dopamine causes selective renal, but not mesenteric vasodilatation in preterm babies with an overall increase in total peripheral vascular resistance. There was no effect on cerebral blood flow at this dose. It is worth noting, however, that this study was carried out on normotensive neonates. Studies in adults suggest that, in sick hypotensive patients, there is a downregulation of adrenergic receptors, requiring much higher doses of dopamine to maintain blood pressure.33 However, there have been no such studies in neonates. There is also some suggestion that preterm infants have relative adrenal insufficiency.34 Further research is clearly required to define a maximum dose for dopamine, as the use of high doses (> 25 μg/kg/min) has not been studied.
Dobutamine is a relatively cardioselective sympathomimetic amine which exerts its positive inotropic action by direct stimulation of cardiac α and β adrenoceptors. It has several theoretical advantages over dopamine: (a) it has limited chronotropic effect; (b) its use is not associated with an increase in systemic vascular resistance30; (c) it does not rely on release of endogenous catecholamines for any part of its action.
The dose of dobutamine that should be used is again unclear. Klarr et al35 and Roze et al30 used doses of 5–20 μg/kg/min, whereas Greenough36 used a maximum dose of 15 μg/kg/min. Hentschel et al37 and Miall-Allen and Whitelaw38 both used a constant infusion rate of 10 μg/kg/min. Stopfkuchen et al39 showed a positive effect on left ventricular performance at doses of 7.5–10 μg/kg/min. The use of high doses (> 25 μg/kg/min) has again not been studied.
There has been relatively little research into the use of dobutamine in preterm neonates, and it is generally used as a second line drug, in patients unresponsive to dopamine. However, several studies have compared dopamine with dobutamine in hypotensive preterm infants. A recent meta-analysis confirmed that dopamine is significantly more effective than dobutamine in the short term treatment of systemic hypotension in preterm infants.40 It also showed that there are fewer treatment failures with dopamine, but that there is no difference in the incidence of tachycardia between the two treatments. There were no differences in short term complications such as intraventricular haemorrhage and necrotising enterocolitis. No data are available on long term outcome for either drug.
Other agents
Most neonatal units advocate the use of adrenaline or noradrenaline in cases in which dopamine and dobutamine have failed to maintain “normal” blood pressure. However, very few studies have looked at the use of these agents in preterm infants. Seri and Evans41 have shown that the addition of adrenaline to dopamine increases both blood pressure and urine output in hypotensive neonates. Derleth42 has suggested that noradrenaline infusions are safe in neonates, and do not cause significant cerebral or myocardial vasoconstriction. Further research is clearly needed in this area before its routine use can be recommended.
Dopexamine, a relatively new synthetic catecholamine, has been shown to be effective in raising blood pressure and improving arterial pH and urine output.43 In neonates who are hypotensive secondary to septic shock, methylene blue, an inhibitor of soluble guanylate cyclase, has been shown to be effective in increasing blood pressure.44
Steroids
Antenatal steroids are now commonly given to mothers in preterm labour. They have been shown to have an independent effect (from the effect on respiratory distress syndrome) on reducing the incidence of hypotension in the preterm infant.45
In neonates with hypotension who are unresponsive to volume or pressor administration, there is growing evidence that steroids may be of some value. The theory is that infants with refractory hypotension may have relative adrenal insufficiency.34,46–48 Because glucocorticoids have a role in regulating the expression of cardiovascular adrenergic receptors,33 this may render these infants incapable of responding to sympathomimetic agents.
Ng et al48 describe five VLBW infants with severe hypotension refractory to both volume expansion and inotropes. All the infants had a normal adrenocorticotrophic hormone response to human corticotrophin releasing hormone, but a low cortisol response, indicating adrenal insufficiency. Treatment with either single dose dexamethasone or a five day course of hydrocortisone was successful in all cases, with discontinuation of inotropes within 54 hours. None of the infants experienced further hypotensive episodes during the following week.
Bourchier and Weston49 found intravenous hydrocortisone, given as a reducing dose over a six day period, starting at 2.5 mg/kg/dose, to be as effective as dopamine in the treatment of hypotension in VLBW infants. Seri et al50 showed that hydrocortisone at 2–6 mg/kg/day resulted in a stable increase in mean blood pressure within six hours. Gaissmaier and Pohlandt51 carried out a double blind, placebo controlled study of the effects of single dose dexamethasone on preterm infants with refractory hypotension. They showed that a single dose of 250 μg/kg of dexamethasone is effective within 12 hours in improving severe arterial hypotension.
Some groups have advocated the use of hydrocortisone in smaller doses as prophylaxis against hypotension in at risk VLBW infants.52 Side effects from postnatal steroids are well documented and probably prohibit prophylactic use.53
Based on the available evidence, we would advocate the use of a single dose of 250 μg/kg dexamethasone in babies with severe, intractable hypotension resistant to inotropes, with a further dose at 12 hours as rescue treatment in unresponsive cases. Although we recognise that there are significant concerns over the use of dexamethasone, it is not clear whether these concerns may in fact be related to any steroid. As the only randomised, blinded, placebo controlled trial of steroids for hypotension uses dexamethasone, this would be our first choice over hydrocortisone. Obviously there is a balance of risks against benefits, but the short term benefit of preventing death must outweigh the long term risks, which are anyway unproven. Further research is obviously needed to decide the optimum dose and course. In our experience most babies do respond to one or occasionally two doses of dexamethasone.
SUMMARY
The management of hypotension in preterm infants remains controversial. Research in this area is relatively limited, which in part is probably due to the difficulty of obtaining continuous measures of tissue perfusion. There is no consensus on either the definition of hypotension or the level at which treatment should be initiated. The effects of aggressive correction are relatively underresearched, and there are few data on morbidity and mortality in relation to the use of volume support and inotropes. The aim of management must be to attain adequate tissue perfusion and oxygenation, but there may be little or no relation between blood pressure and organ perfusion. Further research is required into methods of assessing tissue perfusion, which can be used alongside monitoring of blood pressure to guide the neonatologist in deciding when to intervene.
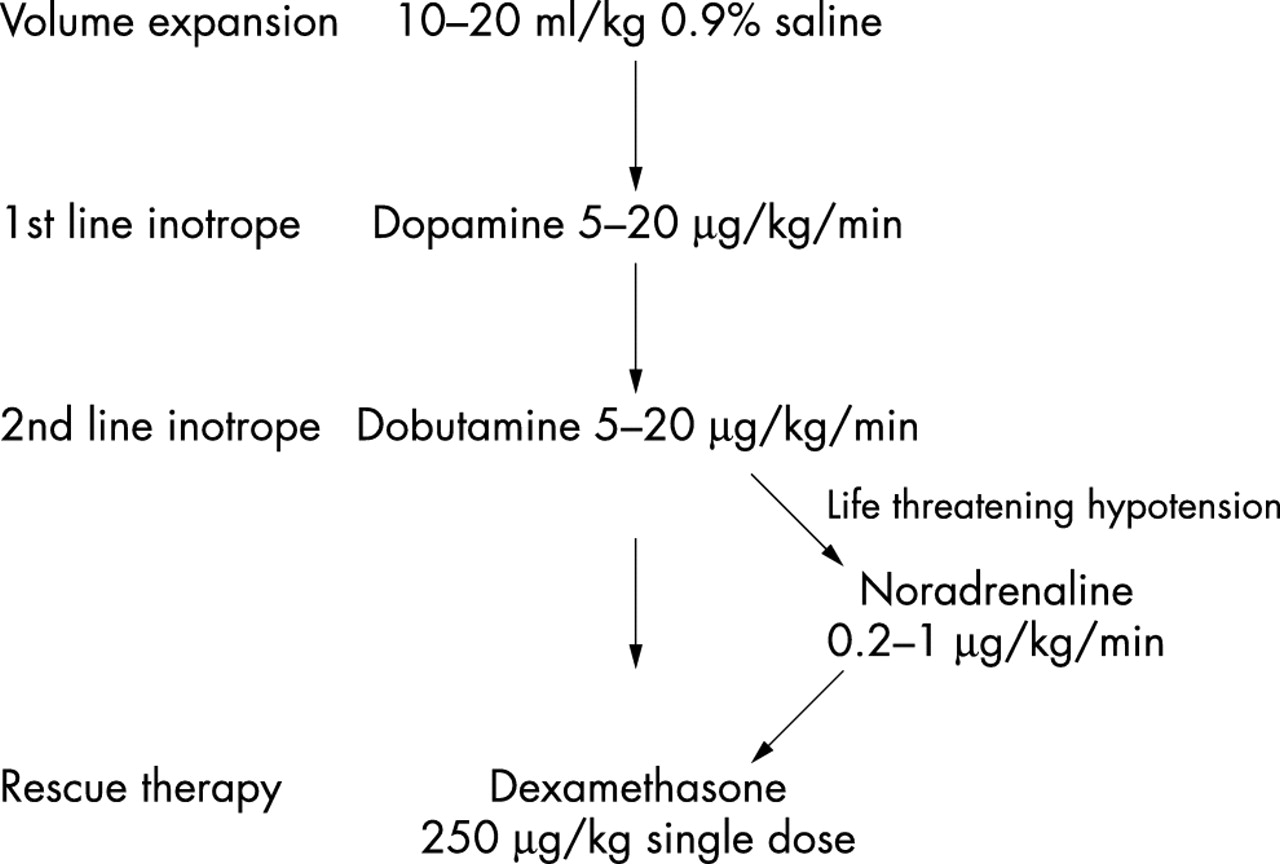
Continuous invasive arterial blood monitoring remains the preferred method of recording blood pressure. Decisions to treat hypotension should be based on the general condition of the infant, not on the mean arterial blood pressure alone. On the basis of the available evidence, fig 1 outlines our view on the management of hypotension in the VLBW infant.

{kind=link}
Flow chart for management of hypotension in the very low birthweight infant.