Article Text

Abstract
Background: The establishment of a balanced intestinal microflora which may protect against infection is desirable for the preterm infant.
Objective: To investigate the effect of a preterm formula milk supplement consisting of oligosaccharides in similar proportions to human milk on the faecal flora and stool characteristics of preterm infants.
Study design: To resemble the effect of human milk, an oligosaccharide mixture consisting of 90% galacto-oligosaccharides and 10% fructo-oligosaccharides was used to supplement a standard preterm formula at a concentration of 10 g/l. This supplemented formula was studied in 15 preterm infants, and the results were compared with those found in 15 infants fed a formula supplemented with maltodextrin as placebo. A group fed fortified mother's milk was investigated as a reference group (n = 12). On four days during a 28 day feeding period (1, 7, 14, and 28), the faecal flora was investigated, and stool characteristics, growth, and possible side effects were recorded.
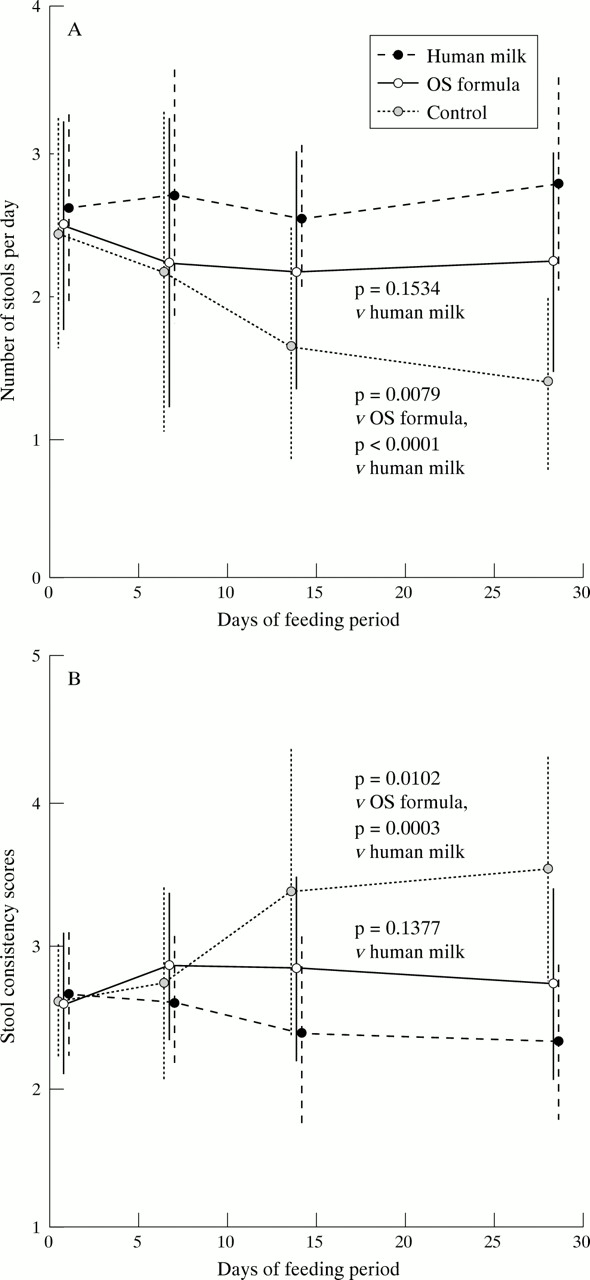
Results: During the study period, the number of bifidobacteria in the group fed the oligosaccharide supplemented formula increased to the upper range of bifidobacteria counts in the reference group. The difference between the supplemented and non-supplemented groups was highly significant (p = 0.0008). The stool characteristics were also influenced by the supplement: the stool frequency after 28 days was significantly lower in the control group than in the oligosaccharide supplemented group (p = 0.0079) and the reference group (p < 0.0001). Over the study period, the stool consistency in the control group became harder, but remained fairly stable in the other two groups. There was no effect of the different diets on the incidence of side effects (crying, regurgitation, vomiting) or on weight gain or length gain.
Conclusion: Supplementing preterm formula with a mixture of galacto- and fructo-oligosaccharides at a concentration of 10 g/l stimulates the growth of bifidobacteria in the intestine and results in stool characteristics similar to those found in preterm infants fed human milk. Therefore prebiotic mixtures such as the one studied may help to improve intestinal tolerance to enteral feeding in preterm infants.
- oligosaccharides
- milk formula
- preterm
- bifidobacteria
Statistics from Altmetric.com
In the neonatal period, the intestine is colonised in a stepwise process that depends on mode of delivery, environmental factors, bacterial interactions, and the host itself, resulting in colonisation with a complex heterogeneous bacterial flora.1
Only a few studies have focused on the early establishment of a balanced intestinal flora in preterm infants,2,3 and they have shown delayed colonisation with bifidobacteria in preterm infants compared with full term infants. The data also indicate that the influence of prematurity of the intestine of preterm infants is not as important as the influence of extrinsic factors such as type of feeding, antibiotic treatment, and the nosocomial environment of these infants during intensive care.
Preterm infants are particularly vulnerable to intestinal infections, therefore the establishment of a balanced microflora that may protect against infection4–,6 is desirable in such infants.
One extrinsic factor that is important for the timing and quality of intestinal colonisation is feeding. Breast milk seems to favour a more diverse microflora with dominance of bifidobacteria and/or lactobacilli, but the mechanism by which this occurs remains to be clarified.7 However, the neutral oligosaccharides of human milk8,9 have been identified as such prebiotic factors. It was recently shown that human milk oligosaccharides are resistant to enzymatic digestion in the upper gastrointestinal tract, which is a prerequisite for a prebiotic effect.10
The composition of neutral oligosaccharides in human milk is very complex,8,9,11–,13 and the functional consequences of these different structures are not fully understood.
In this study, we aimed to reproduce the prebiotic effect of human milk oligosaccharides. Because of the high amount of galactose in human milk oligosaccharides, we used available galacto-oligosaccharides derived from lactose as one component of the mixture.14 The second component was fructo-oligosaccharides extracted from chicory roots with a reduced amount of the low molecular mass fraction (degree of polymerisation (DP) > 10). Fructo-oligosaccharides with DP > 10, as a high molecular mass inulin fraction, have a slower fermentation rate than low molecular mass fructo-oligosaccharides, possibly resulting in fewer side effects such as flatulence.15
The mixture is composed in such a way that the size distribution of the molecules is similar to that of human milk oligosaccharides, therefore containing 90% of the low molecular mass galacto-oligosaccharides and 10% of the high molecular mass fructo-oligosaccharides.12 This combination promotes beneficial intestinal bacteria in a synergistic way so that a maximum number of different species, especially bifidobacteria and lactobacilli, can grow.16
The prebiotic effects of both compounds have been shown in several human studies,9,15,17–,19 but to our knowledge they have never been used in combination.
In this study, the effect on the faecal microflora of supplementing a preterm formula with such an oligosaccharide mixture, with particular respect to bifidobacteria, was investigated in preterm infants.
PATIENTS AND METHODS
Preterm infants with a maximum gestational age of 32 weeks according to Dubowitz and Dubowitz20 admitted to the neonatal intensive care unit of the Hospital Mangiagalli, Milan, were eligible for the study. The study protocol was approved by the ethical committee of the hospital, and informed parental consent was obtained for each infant before enrolment in the study.
For all infants, enteral nutrition was started with pasteurised mother's milk. When a volume of 80 ml/kg/day was tolerated, the milk was supplemented with a commercially available human milk fortifier. When the neonatologist in charge decided to start formula feeding because the mother was no longer able to provide milk, the infants were randomly assigned to one of two formula groups. The compositions of the two formulas were, apart from the supplemented oligosaccharides, identical (table 1⇓). The feeding regimen was performed according to the practice of the hospital and was not influenced by the study protocol. A group fed fortified mother's milk matched for sex and gestational and postnatal age was investigated as the reference group. Table 2⇓ gives the most relevant clinical data of the infants studied.
Composition per 100 ml of the two formulas studied
Clinical characteristics of the study population
In the experimental formula, a mixture of fructo-oligosaccharides and galacto-oligosaccharides was added to an otherwise standard preterm formula. As it was the intention to reproduce the spectrum of molecular masses of human milk, the relation between galacto-oligosaccharides and fructo-oligosaccharides was a matter of some experiment. On the basis of our own analytical data,12 a mixture of 9 parts galacto-oligosaccharides and 1 part fructo-oligosaccharides was found to closely resemble the spectrum of molecular masses of the neutral oligosaccharide fraction of human milk. The concentration of the mixture in the formula was adapted to the concentration of neutral oligosaccharides in human milk—that is, 10 g/l.12 In the control group, a similar quantity of maltodextrins was added as placebo.
The first day of full formula feeding was defined as measurement day 1. Measurements were repeated after seven, 14, and 28 days. On each of these days, faecal flora was investigated, and stool characteristics as well as possible side effects were recorded.
Microbiological analysis of fresh stool sample was performed after suspension, homogenisation, and dilution in physiological saline solution. For analysis of bifidobacteria and lactobacilli, 1 ml of the diluted suspension was inoculated into 10 ml Soybean Casein Digest Agar and incubated at 37°C for five hours. The layer of Soybean Casein Digest Agar was then overlaid with 10 ml Rogosa Agar. After microaerophilic incubation for two days at 37°C, single colonies were counted and identified on the basis of their morphology and biochemical reactions as described previously.21 The faecal samples were also analysed for Bacteroides, Clostridium species, Escherichia coli, Enterobacter, Citrobacter, Proteus, Klebsiella, and Candida.
The oligosaccharides were analysed by matrix assisted laser desorption/ionisation mass spectrometry (MALDI-MS) as described previously.12,13,22 For each spectrum, a sum of 50 single spectra was recorded in linear positive ion mode (Voyager DE-STR; Applied Biosystems, Langen, Germany).
Stool characteristics were evaluated on the basis of a questionnaire about frequency and consistency (score 1–5: 1 = watery; 2 = soft; 3 = seedy; 4 = formed; 5 = hard). The consistency of each stool of the respective day was recorded, and the mean of all scores was used to characterise the stool consistency of the respective day.
In addition, the incidence of crying (score 1–3: 1 = seldom; 2 = normal; 3 = often), regurgitation (score 1–3: 1 = none; 2 = once or twice; 3 = more than twice), and vomiting (score 1–3: 1 = none; 2 = once; 3 = more than once) was recorded on the basis of the nurse's report.
For all infants, body weight was measured on each measurement day using a balance with an accuracy of ± 5 g. The crown-heel length was measured at the start and end of each feeding period using a special board for newborn infants with an accuracy of ± 1 mm.
Statistical analysis
All data are given as means (SD). An overall group effect on a measured variable was evaluated by one way analysis of variance. If significant, this was followed by Scheffé post hoc tests for single group comparisons. All tests were performed at an α level of 5%. p < 0.05 was considered significant. StatView 5.0 (SAS Institute Inc) was used for the analyses.
RESULTS
The molecular mass distribution of the mixture containing 90% galacto-oligosaccharides and 10% fructo-oligosaccharides as measured by MALDI-MS is similar to that found in the neutral oligosaccharide fraction of human milk (data not shown).
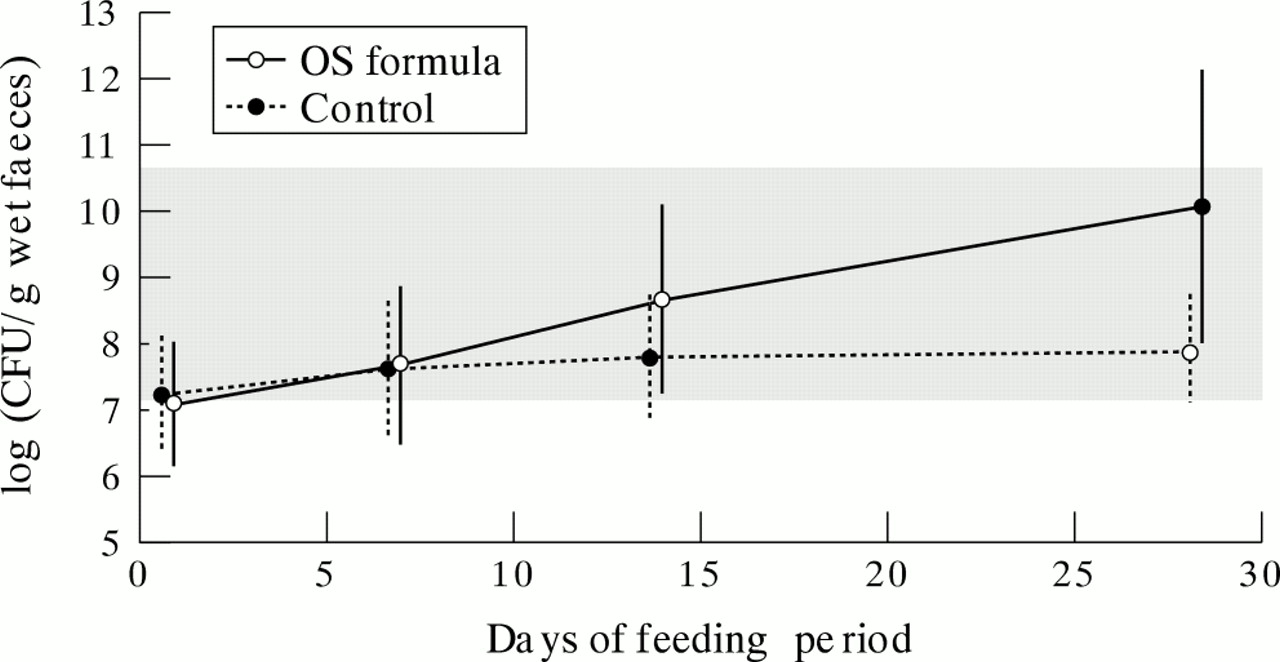
Bifidobacteria were detectable on the first measurement day in all faecal samples. There was no difference between the two formula groups, and both were in the range of the reference group. During the study period, the number of faecal bifidobacteria increased significantly with time in both groups receiving formula (p < 0.05), but this increase was only marginal in the group fed the control formula (fig 1⇓). After the 28 day feeding period, the number of bifidobacteria in the group fed the oligosaccharide supplemented formula was in the upper range of the reference group whereas the number in the control group fed the formula supplemented with the placebo was in the lower range. This difference between the two groups receiving formula was highly significant (p = 0.0008) (fig 1⇓).

Number of bifidobacteria (mean (SD) log of colony forming units (CFU)/g wet faeces) in the group fed the experimental formula with oligosaccharides (OS formula) and the group fed the unsupplemented control formula (Control). The shaded area indicates the reference range for infants fed human milk (mean (SD) 8.9 (1.8)). The difference between the groups at 28 days was highly significant (p = 0.0008; t test).
Lactobacilli were also detectable in all infants at the study entry. There was a significant increase in all groups during the course of the study period but there was no significant effect of the diet (data not shown). Neither was there a significant effect of the oligosaccharide supplement on the counts of Bacteroides, Clostridium species, E coli, Enterobacter, Citrobacter, Proteus, Klebsiella, and Candida.
Mean stool frequency increased slightly in the reference group fed mother's milk, remained fairly constant in the group fed the oligosaccharide supplemented formula, and gradually decreased in the placebo group (fig 2⇓). At day 28, the highest frequency was observed in the group fed mother's milk (2.75 (0.8)), which was significantly higher than in the group fed the unsupplemented formula (1.33 (0.6); p < 0.0001) and tended to be higher, but not significantly so, than in the group fed the oligosaccharide supplemented formula (2.20 (0.8); p = 0.1543).
{kind=link}
{kind=link}
Effect of the formula supplemented with oligosaccharides (OS formula) and the unsupplemented formula (Control) on (A) stool frequency (mean (SD)) and (B) consistency scores (mean (SD); 1 = fluid; 2 = soft; 3 = seedy; 4 = formed; 5 = hard) during the 28 day study period in comparison with the reference group fed human milk. Group differences shown at 28 days were evaluated by analysis of variance followed by Scheffé post hoc tests.
The stool consistency was also influenced by the diet (fig 2⇑). In the group fed the unsupplemented formula, the score increased during the study period and reached the highest level at the end of the study period. On day 28, the hardest stools were observed in the group fed the unsupplemented formula (score 3.55 (0.8)); they were significantly harder than in the group fed the oligosaccharide supplemented formula (score 2.74 (0.7); p = 0.0102) and in the reference group (score 2.33 (0.6); p = 0.0003).
There was no effect of the different diets on the incidence of crying, regurgitation, or vomiting (data not shown). Weight gain and length gain was similar in all the groups (table 2⇑).
DISCUSSION
The prebiotic oligosaccharide mixture used in the study was designed to stimulate growth of bifidobacteria. The data show that supplementation of a standard preterm milk formula with this mixture can significantly stimulate bifidobacterial growth, indicating a bifidogenic effect of the oligosaccharide supplement. In many studies on preterm infants, a delay in the establishment of a bifidogenic flora has been observed. In this study, the first effect of the supplementation on the number of faecal bifidobacteria was already observed after 14 days, which underlines the bifidogenic potency of the supplement. However, the effect of the supplement on the number of bifidobacteria was more pronounced after 28 days.
A prerequisite for a bifidogenic effect of a dietary ingredient is its resistance to digestion during passage through the small intestine. Even though the digestibility of the supplemented oligosaccharides was not measured in this study, the clear bifidogenic effect indicates that their absorption was as low as found for those in human milk.10
The increase in the number of faecal bifidobacteria was accompanied by increased stool frequency and a significant change towards softer stools. Increased frequency and softer stool consistency is an effect of the supplementation that is of practical importance because hard stools and obstipation are common problems that limit the tolerance of preterm infants to enteral feeding.23 Only 10 g/l of the studied mixture or placebo was added to the formula, which increases the osmolarity (about 5 mOsmol/l) only slightly. Thus, the effect of the supplementation on osmolarity cannot explain the different effects on the stool characteristics, which are probably influenced by the changes in intestinal flora; this is in line with many studies.
A bifidogenic effect of galacto-oligosaccharides16,19 and fructo-oligosaccharides15,17,18 has previously been shown. In this study, the strong bifidogenic effect may be explained by a synergistic effect of galacto- and fructo-oligosaccharides—for example, by promoting different strains of bifidobacteria16—or, as indicated by in vitro studies, by providing prebiotic substrate to more distal regions of the colon because of the slower rate of fermentation of the high molecular mass inulin fractions.15 However, as the galacto- and fructo-oligosaccharides were not studied independently, we cannot comment on the individual contributions of the two oligosaccharides to the observed effects.
The study was conducted in healthy preterm infants who tolerated complete enteral nutrition and were not receiving antibiotic treatment—that is, a very selected population. In addition, enteral nutrition in all infants started with mother's milk for several days, which may have influenced the intestinal colonisation at study entry. In fact, bifidobacteria were detected in all infants on the first day of measurement. Therefore the study cannot answer whether such a bifidogenic effect would be observed if intestinal colonisation were severely compromised—for example, after intensive antibiotic treatment.
Studies in adults indicate that dietary fructo-oligosaccharides may lead to side effects, in particular flatulence. In a study using fructo-oligosaccharides during infancy with an intake of up to 3 g/day, however, no such effects were observed.24 In the present study also, in which only 0.3 g fructo-oligosaccharides were ingested a day, no side effects occurred.
The quantity of oligosaccharide supplement used was 10 g/l, to resemble the amount of neutral oligosaccharides found in human milk.12 The strong and rapid effect on the bifidus flora and stool characteristics suggests that a lower dose may have been sufficient to achieve positive effects on the intestine. This requires further investigation.
In summary, supplementation of a preterm formula with a mixture of galacto- and fructo-oligosaccharides stimulates growth of bifidobacteria and results in stool frequency and consistency similar to those found in preterm infants fed human milk. Thus prebiotic mixtures such as that studied here may help to improve intestinal tolerance to enteral feeding. Further studies on the optimal relation between the different compounds and the dose of the mixture are necessary.
Acknowledgments
The study was supported by a grant from Numico Research Germany. We thank Mrs D Krämer and Mrs A Knosmann for performing a literature search, and Mr M Mank for performing the MALDI-MS analyses.