Article Text

Abstract
Objective: To determine if differences in respiratory muscle strength could explain any posture related effects on oxygenation in convalescent neonates.
Methods: Infants were examined in three postures: supine, supine with head up tilt of 45°, and prone. A subsequent study was performed to determine the influence of head position in the supine posture. In each posture/head position, oxygen saturation (Sao2) was determined and respiratory muscle strength assessed by measurement of the maximum inspiratory pressure (Pimax).
Patients: Twenty infants, median gestational age 34.5 weeks (range 25–43), and 10 infants, median gestational age 33 weeks (range 30–36), were entered into the first and second study respectively.
Results: Oxygenation was higher in the prone and supine with 45° head up tilt postures than in the supine posture (p<0.001), whereas Pimax was higher in the supine and supine with head up tilt of 45° postures than in the prone posture (p<0.001). Head position did not influence the effect of posture on Pimax or oxygenation.
Conclusion: Superior oxygenation in the prone posture in convalescent infants was not explained by greater respiratory muscle strength, as this was superior in the supine posture.
- posture
- respiratory muscle strength
- oxygenation
Statistics from Altmetric.com
In the perinatal period, infants with respiratory distress placed prone rather than supine have higher oxygen saturation (Sao2) levels1 and better respiratory mechanics.2 Improved oxygenation and lung compliance has also been noted in premature infants recovering from respiratory disease.3 In term infants with lower respiratory tract infections aged between 2 and 11 months, however, only a modest (1.7%) improvement in oxygenation was noted with prone posture.4 The effect of posture and the mechanism of any posture related benefits have been less well investigated in convalescent preterm infants. The limited data available suggest that prone posture may still in such infants be associated with improved oxygenation.5,6 In addition, healthy preterm infants have a better response to a carbon dioxide challenge7 and reduced frequency of central and mixed apnoeas, bradycardias, and desaturations8 when nursed prone. The diaphragm is the primary respiratory muscle in the neonate and performs most of the work of breathing.9 Changes in posture by alterations in respiratory system mechanics or lung volume could affect diaphragm function by influencing the resting length of the diaphragm or the degree to which it shortened during inspiration.10 We therefore hypothesised that any posture related changes in oxygenation in convalescent infants could be explained by alterations in respiratory muscle strength. The aims of two consecutive studies were to test that hypothesis.
METHODS
Protocols
Infants were eligible for entry into the studies if they had no continuing respiratory problems and were nursed in air. In the first study (study A), infants were examined in three postures: supine, supine with a tilt of 45°, and prone. The supine head up tilt posture was achieved by putting the infant on a firm cot mattress maintained at 45° tilt. When supine, the infant's head was kept in the midline, but when prone it was turned to the right. The second study (study B) was performed to examine whether the position of the infant's head in the supine posture affected the results of the comparison of the supine and prone postures. Infants were examined as follows: supine with head in the midline, supine with head to the right, and prone with head to the right. The order in which the postures/head positions were studied was randomised between babies.
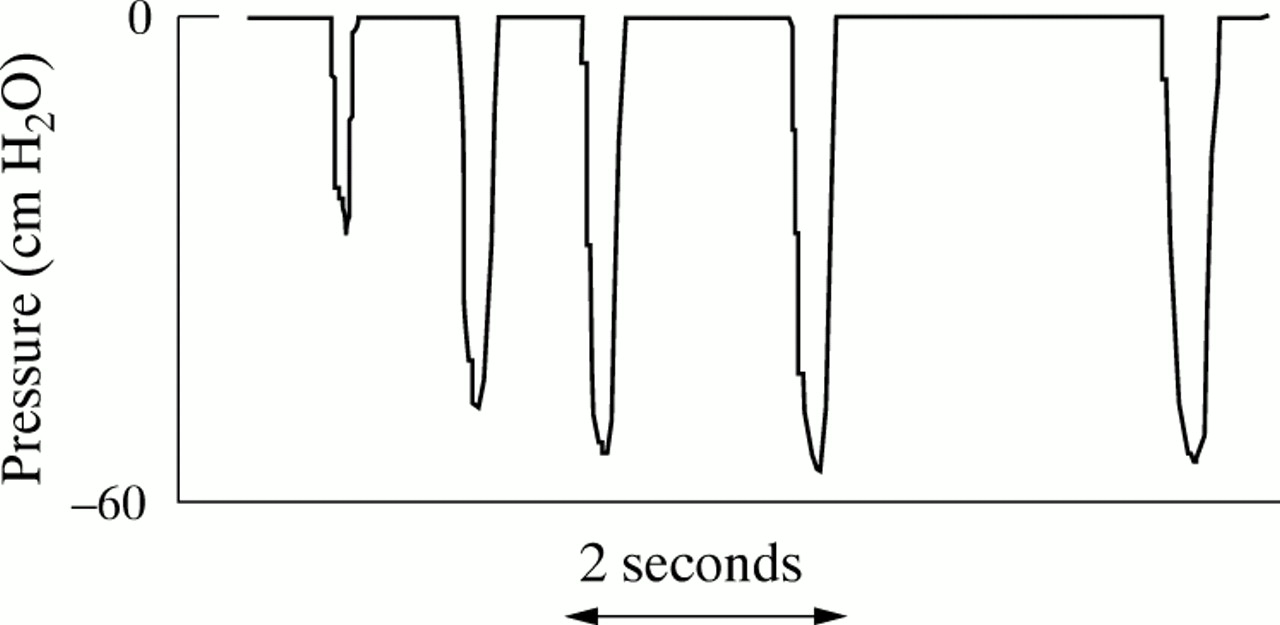
Respiratory muscle strength and oxygen saturation were measured in each posture/head position. Infants were studied when awake and about one hour after a feed. All the infants were on full enteral feeds. To assess respiratory muscle strength, the maximum inspiratory pressure (Pimax) generated during an end expiratory occlusion was measured (fig 1⇓). A face mask was placed over the infant's nose and mouth, with a pneumotachograph (GM Engineering, Kilwinning, Ayrshire, UK) fitted snugly into the distal end of the facemask. Airway pressure changes were measured from a side port on the pneumotachograph using a differential pressure transducer (Validyne MP 45, range ± 100 cm H2O; Validyne Corporation, Northridge, California, USA). The pressure transducer was calibrated before each recording using a Universal Pressure Meter (Co-Mark, Welwyn Garden City, Herts, UK). The signal from the pressure transducer was amplified using a Gould CD 280 carrier amplifier (Gould, Ilford, Essex, UK). The results were displayed in real time on a Toshiba laptop running Labview software version 4.0 (National Instruments, Austin, Texas, USA) with a 100 Hz analogue to digital sampling (DAQ 16XE-50; National Instruments). A two way valve was inserted in the distal end of the pneumotachograph. Occlusion of the valve at end expiration allowed expiration but not inspiration. At least three occlusions were performed at end expiration. The exact timing of the manual occlusion was determined by observation of the infant's respiratory movements. Occlusions were maintained until the infant had made at least five respiratory efforts. From the series of occlusions, Pimax was identified as the largest negative pressure generated. During the measurements the infants were observed for episodes of chest wall distortion. During and immediately after the occlusion, on no occasion did Sao2 fall below 85%. Sao2 was monitored using an Ohmeda Biox 3470-pulse oximeter with an Ohmeda flex II reusable probe. Infants remained in each posture/position for 30 minutes, and then the saturation level was recorded for a five minute period just before the measurement of Pimax. A spot reading was written down once a minute, and the mean Sao2 for the five minute period was reported. From the infant's medical records, gestational age, birth weight, postnatal age, and weight at the time of measurement were obtained.
{kind=link}
Representative trace of airway pressure during measurement of maximum inspiratory pressure (Pimax). Airway occlusions were performed at end expiration on at least three separate occasions. Each occlusion was maintained until the infant had made at least five inspiratory efforts. From the series of occlusions, Pimax was identified as the largest negative pressure generated.
Statistical analysis
Data were tested for normality using the Sharpiro-Wilk W test and found to be distributed normally. Differences in Pimax and Sao2 between positions/head posture were assessed for statistical significance using analysis of variance for repeated measures and the Scheffe test for multiple comparisons.
Patients
In study A, 20 infants (12 boys), 12 born less than or equal to 37 weeks of gestational age, were studied. They had a median gestational age of 34.5 weeks (range 25–43) and birth weight of 2.228 kg (range 0.684–3.740). At the time of study the infants had a median postnatal age of 12.5 days (range 4–91), postconceptional age of 38.5 weeks (range 31–44), and weight of 2.456 kg (range 1.686–4.286).
In study B, 10 infants (seven boys) were examined. They had a median gestational age of 33 weeks (range 30–36) and birth weight of 1.940 kg (range 1.152–2.130). At the time of study their median postnatal age was 19.5 days (range 15–63), postconceptional age was 36 weeks (range 35–39), and weight 2.175 kg (range 1.800–2.360).
The studies were approved by King's College Hospital National Health Service Trust research ethics committee and parents gave informed written consent for their infants to be examined.
RESULTS
Study A
Compared with the prone posture, Pimax was higher in the supine posture and supine with 45° tilt posture (p<0.001) (table 1⇓). There were no significant differences between the supine and supine with 45° tilt postures. Compared with in the supine posture, Sao2 was significantly higher in the prone and supine with 45° tilt postures (p<0.001) (tables 1 and 2⇓⇓). There were no significant differences between the prone and supine with 45° tilt postures (table 1⇓). Analysis of the results of the 12 infants born at or less than 37 weeks of gestational age also showed the median Pimax to be higher in the supine than the prone posture (74.4 (range 46.2–118.2) v 66.5 (range 39.7–89.5) cm H2O, p<0.01), and the median Sao2 to be higher in the prone than the supine posture (median 98% (range 96–100%) v 96.5% (range 94–99%), p<0.001).
Effect of posture on oxygenation and respiratory muscle strength (study A)
Individual Sao2 data related to posture (study A)
Study B
Compared with in the prone posture, Pimax was higher in the supine posture both with the head in the midline (p<0.001) (table 3⇓) and with the head to the right (p<0.01), and Sao2 was lower in the supine posture both with the head in the midline (p<0.001) and with the head to the right (p<0.05) (table 3⇓). In the supine position, there was no significant difference in Pimax measured with the infant's head in the midline or to the right.
Effect of head position (study B)
DISCUSSION
We have shown that respiratory muscle strength, as assessed by measurement of Pimax, is higher in the supine than the prone posture, whereas the reverse was found with regard to oxygenation. Many factors affect muscle strength. After only a few days of mechanical ventilation, disuse atrophy has been noted in healthy adult baboons.11 In addition, respiratory muscle strength is related to maturity at birth, Pimax being higher in term than preterm infants.12 To avoid such biases, in each of the two studies the infants acted as their own controls. To assess respiratory muscle strength, the inspiratory pressure generated against an occlusion was measured. Pimax was measured in the infants during spontaneous crying, and thus we feel was a reflection of respiratory muscle strength rather than respiratory drive. Two occlusion methods can be used: one involves total airway occlusion and the second a unidirectional expiratory valve that permits exhalation but prevents subsequent inspiration.13,14 Marini et al13 showed that, although the timing of the maximum pressure generated was not affected by the choice of methods, the maximum pressure achieved was almost invariably higher when a unidirectional expiratory valve was used. Pimax varies with the lung volume at the time of airway occlusion.15,16 The likely explanation for the findings of Marini et al13 is that use of a unidirectional expiratory valve resulted in lower lung volumes with improved operating characteristics of the inspiratory muscles.17 At low lung volumes, the length of the inspiratory muscles and the geometry of the diaphragm are optimised.13,17 Also, outward recoil of the relaxing chest wall near residual volume assists the inspiratory musculature in achieving inspiratory force.18 In this study, we used an occlusion method, which allowed exhalation but not inspiration, and showed significant differences in Pimax between the prone and supine postures.
In the first study, Pimax was higher in the supine and supine with 45° head up tilt postures than in the prone posture. In the supine posture, the infant's head position was in the midline, whereas, in the prone posture, it was held to the right. Thus we could not exclude the possibility that our results were due to differences in head position, Pimax measurements perhaps being more difficult to make when the infant's head was turned to the right. In addition, head turning results in deformation of the airways.19 A second study was therefore performed in which each infant was assessed in both the supine and prone posture with the head to the right, as well as in the supine posture with the head to the midline. The supine posture, regardless of head position, was associated with a significantly higher Pimax than the prone posture. There was no significant difference in the median Pimax between the two head positions in the supine posture. Pimax was determined as the maximum pressure achieved during an occlusion maintained for five breaths, and the same technique was applied in all postures and head positions. Thus our results indicate that Pimax is influenced by posture.
Changing from the supine to the prone posture in healthy full term infants has been reported to be associated with lessened thoracoabdominal incoordinaton and increased tidal volume.20 In our population we did not observe chest distortion but, as we did not use respiratory inductive plethysmography, we cannot be confident that this did not occur in the prone position. It has been suggested that the advantageous effects of the prone posture in healthy full term neonates could be due to changes in diaphragm function.20 The authors felt that the prone position, by permitting the area of greater excursion of the diaphragm to be unopposed by hydrostatic pressure, would increase diaphragmatic work and allow more efficient ventilation.21 In addition, they emphasised that the prone posture increases intra-abdominal pressure, passively distending the diaphragm and stabilising the compliant chest wall.22 The postulated effect of the prone posture on diaphragmatic function in healthy term neonates20 is not supported by either our findings of a higher Pimax in the supine compared with the prone posture or postural differences in diaphragm configuration recently described in healthy term neonates.10 Using ultrasonographic examination, Relian et al10 showed that the diaphragm was significantly thicker at end expiratory volume in the prone than in the supine posture. In addition, the prone posture was associated with greater diaphragm thickening during inspiration. It was concluded that, in the prone posture, the diaphragm and diaphragm shortening during tidal breathing is greater. There were similar findings in a canine model.23 The degree of diaphragm shortening in the prone compared with the supine posture10 was similar to that resulting from a lung volume increase of 15–20% of vital capacity.24 In adults such an increase in lung volume results in a 40–50% reduction in diaphragm strength and endurance.25 Thus it is not surprising that we found that Pimax was lower in the prone than in the supine posture.
Prone compared with supine posture has been associated with improved oxygenation outside the perinatal period in preterm infants with chronic oxygen dependency.5,6 The infants we examined were convalescent, without continuing respiratory problems, and their average postconceptional age was term. Posture related changes in thoracoabdominal synchrony have been reported in both preterm2 and term20 infants. In the term infants, the reduced thoracoabdominal asynchrony in the prone posture was associated with improved ventilation and increased respiratory drive.20 Such changes may therefore explain the improved oxygenation observed by us in the prone posture.
A possible explanation for the higher oxygenation in the prone posture may be a higher lung volume, resulting from reduced cephalad stress on the diaphragm. Others, however, have suggested that lung volume may be lower in the prone position because of the compressing effect of the infant's body weight on the relatively compliant chest wall.26 The impact of posture on functional residual capacity of preterm infants at a postconceptional age of near term is unexamined but, in healthy full term infants, no posture related significant changes in either functional residual capacity or effective pulmonary blood flow were shown in the first days after birth.26
Prone posture also influences the likelihood of gastro-oesophageal reflux. Nursing infants prone is associated with less severe gastro-oesophageal reflux in both symptomatic27 and asymptomatic28 infants and with less gastric residual. In addition, prone positioning resulted in a decreased number of apnoeic episodes in preterm infants with gastro-oesophageal reflux and theophylline resistant apnoea.29
Oxygenation was significantly higher in the supine with 45° head up tilt posture than in the supine posture. A head tilt of 15° has been associated with a reduction in the frequency of hypoxaemic episodes in prematurely born infants.30 In addition, head elevation by 20–45° has been shown to improve oxygenation.31,32 Possible mechanisms include improved ventilation/perfusion matching.30 It has been suggested that tilting may also improve diaphragm activity.31 Our results, however, do not support this hypothesis,31 because, although Pimax was higher in the supine with 45° head up tilt posture than in the prone posture, there was no significant difference in the Pimax results obtained in the supine with 45° head up tilt posture compared with the supine posture.
We conclude that oxygenation is significantly better in convalescent preterm and term infants when they are nursed prone rather than supine. Differences in respiratory muscle strength seem unlikely to explain these posture related changes in oxygenation.
Acknowledgments
G D was supported by a Children Nationwide Medical Research Fund/Nestle Research Fellowship. We thank Ms Sue Williams for secretarial assistance.
A G and G F R were responsible for the study design. G D and A H were research fellows involved in data collection. L P and M McG, BSc students, assisted the research fellows in data collection. All authors were involved in data analysis and producing the manuscript.
REFERENCES
Linked Articles
- Fantoms