Article Text

Abstract
AIMS To determine if nitric oxide (NO) products (nitrate and nitrite) are increased in bronchoalveolar lavage (BAL) fluid obtained from infants who develop chronic lung disease of prematurity (CLD).
METHODS One hundred and thirty six serial bronchoalveolar lavages were performed on 37 ventilated infants (12 with CLD, 18 with respiratory distress syndrome (RDS), and seven control infants) who did not receive inhaled NO.
RESULTS During the first week of life nitrate concentration was between 25–31 μmol/l in all three groups. Thereafter, the concentration of BAL fluid nitrate decreased to 14 μmol/l and 5.5 μmol/l, respectively in the RDS and control groups by 14 days of age. In contrast, nitrate in the CLD infants remained constant until 28 days of age (31.3 μmol/l at day 14; p<0.05). In all BAL fluid samples the mean concentration of nitrite was <1.2 μmol/l throughout the first 28 days with no significant differences noted among the three groups.
CONCLUSION The similar concentration of BAL fluid nitrate in all groups during the first week of life suggest that NO may be important in the adaptation of the pulmonary circulation after birth. However, persistence of nitrate in the BAL fluid of infants with CLD during the second week may reflect pulmonary maladaptation, or, more likely, persisting pulmonary inflammation.
- chronic lung disease of prematurity
- nitric oxide
- nitrate
- bronchopulmonary dysplasia
Statistics from Altmetric.com
Chronic lung disease of prematurity (CLD) is a common sequelae of respiratory distress syndrome (RDS) in preterm infants.1 2 Although the risk factors for CLD, which include oxygen toxicity, barotrauma, immaturity, infection, and patent ductus arteriosus,1-3 have been identified, the exact pathophysiology of CLD remains unknown. However, persisting pulmonary inflammation has been increasingly reported in association with the development of CLD.4-9 Many of these pro-inflammatory cytokines, including tumour necrosis factor α, interleukin-1, and interleukin-6, can increase the expression of inducible nitric oxide synthase (iNOS) in a variety of cell types.10 11
In 1987, Palmer et al 12 and Ignarro et al 13 reported that endothelial derived relaxing factor was nitric oxide (NO). It has since been shown that NO is a ubiquitous molecule with many diverse physiological functions, including relaxation of smooth muscle in blood vessels,14 neurotransmission,15 effects on immune function16-18 and platelet function.19 NO production may be increased in diseases, such as asthma,20 21 pneumonia,22 and sepsis.23 NO may therefore have an important role in the pathophysiology of respiratory disease. The role of NO in the pathogenesis of CLD is currently unknown.
NO is formed by the enzyme nitric oxide synthase from L-arginine and it has a short half life of < 1 second in blood.24 The oxidation reactions of NO are complex and involve nitrogen in many different oxidation states. NO combines extremely rapidly with superoxide radicals to produce peroxynitrite. This reaction occurs preferentially to that of superoxide inactivation by superoxide dismutase.25 Peroxynitrite is unstable at physiological pH and readily decomposes to form nitrite and nitrate.26 27 Both these products may also be formed from nitrogen dioxide, low concentrations of which may be present if endogenous NO is produced in the inflammatory environment of infants who subsequently develop CLD.
As pulmonary inflammation is associated with the development of CLD, and because pro-inflammatory cytokines increase the expression of iNOS, we thought that infants who developed CLD would have increased production of endogenous NO. To assess the production of endogenous NO, we determined the concentration of nitrate and nitrite in bronchoalveolar lavage (BAL) fluid obtained from infants who did and did not develop CLD, but who had not received inhaled NO.
Methods
Newborn infants requiring mechanical ventilation were recruited to the study. Three groups of infants were studied: (a) those with CLD, comprising infants who were initially ventilated for RDS and who were oxygen dependent and had chest radiographic changes at 28 days of age28; those with RDS, comprising infants who were ventilated for RDS, but who were nursed in air, and had a normal chestx-ray picture by 28 days of age; and controls who required ventilation for non-respiratory reasons and required an FIO2 of less than 0.28.
Infants who were diagnosed as having persistent pulmonary hypertension of the newborn by echocardiography or who had received inhaled nitric oxide treatment were excluded from the study. Infants of mothers who had infection or prolonged rupture of the membranes (of greater than 48 hours) were also excluded as were infants with infection at any time verified by positive blood or endotracheal secretion culture.
Informed consent was obtained from the parents and the study was approved by the local research ethics committee.
Bronchoalveolar lavage was performed twice weekly at the time of routine endotracheal tube suction until extubation or 28 days of age, as described before.29 The infant was placed supine with the head to the left. A 5 FG suction catheter was passed until resistance was felt. One ml/kg of physiological saline was then instilled and aspirated immediately. This process was repeated and the 2 aliquots were pooled. The fluid was centrifuged within 10 minutes of collection at 500 × g for 10 minutes and the supernatant fluid stored at −70°C for subsequent analysis of nitrite and nitrate.
ASSAY METHODS
Nitrite assay
The samples were thawed on ice to prevent degradation of nitrite and were centrifuged in 12 kDa molecular weight cutoff ultrafiltration microcentrifuge tubes (Whatman, Maidstone) at 12000 rpm for 35 minutes to remove proteins which may interfere with the assay. Nitrite concentration was determined using a commercial kit (Nitrate/Nitrite Fluorometric Assay Kit, Cayman Chemicals, Ann Arbor, USA) based on a fluorometric method described by Misko.30 Nitrite reacted with 2,3-diaminonaphthalene (DAN) to produce a fluorescent compound (excitation 365 nm and emission 450 nm). The limit of detection for this assay was 0.2 μM nitrite.
Nitrate assay
Nitrate was measured according to the manufacturer’s instructions (Nitrate/Nitrite Fluorometric Assay Kit, Cayman Chemicals, Ann Arbor, USA). Briefly, nitrate was reduced to nitrite by anAspergillus species nitrate reductase (E.C.1.6.6.2) in the presence of essential cofactors NADPH and flavine adenine dinucleotide (FAD).31 Nitrite was subsequently assayed as described above. The limit of detection was also 0.2 μM.
The median (range) is shown for gestation and birthweight of the infants studied. Because of skewed data, the means (SEM) of the log transformed data for nitrite and nitrate concentrations were calculated for which the anti-logs are illustrated. Multiple groups were compared using the non-parametric Kruskal-Wallis test and comparisons between groups were made using the Mann-Whitney U test. A p value of <0.05 was considered significant.
Results
Patient characteristics are shown in table 1. One hundred and thirty six lavages were performed on 37 infants receiving mechanical respiratory support. Twelve infants (5 girls, 7 boys) developed CLD, 18 had acute RDS (8 girls, 10 boys) and seven infants (1 girl, 6 boys) were ventilated for non-respiratory reasons (4 for abdominal surgery, 1 for tracheo-oesophageal fistula with oesophageal atresia, 1 for mild asphyxia at birth and 1 for apnoea). Antenatal dexamethasone had been given to 11 of 12 mothers in the CLD group, 11 out of 18 in the RDS group, and one of seven in the control group. The birthweight and gestational age of the CLD group was significantly lower than that of the RDS or control groups (birthweight: CLDvs RDS p<0.05, CLDvs controls p<0.05; gestational age: CLDvs RDS p<0.05, CLDvs controls p<0.05).
Patient characteristics
Surfactant (Survanta, Abbott Laboratories) was given to all the infants in both the CLD and RDS groups but none was given to infants in the control group. The first bronchoalveolar lavage was performed before the first dose of surfactant was administered. There were no differences between the CLD and RDS groups for maximum peak inspiratory pressure, maximum FIO2, mean airway pressure or oxygenation index on day 1 (table 1). As expected, the control group had a significantly lower maximum FIO2 and mean airway pressure (p<0.05) than the other two groups.
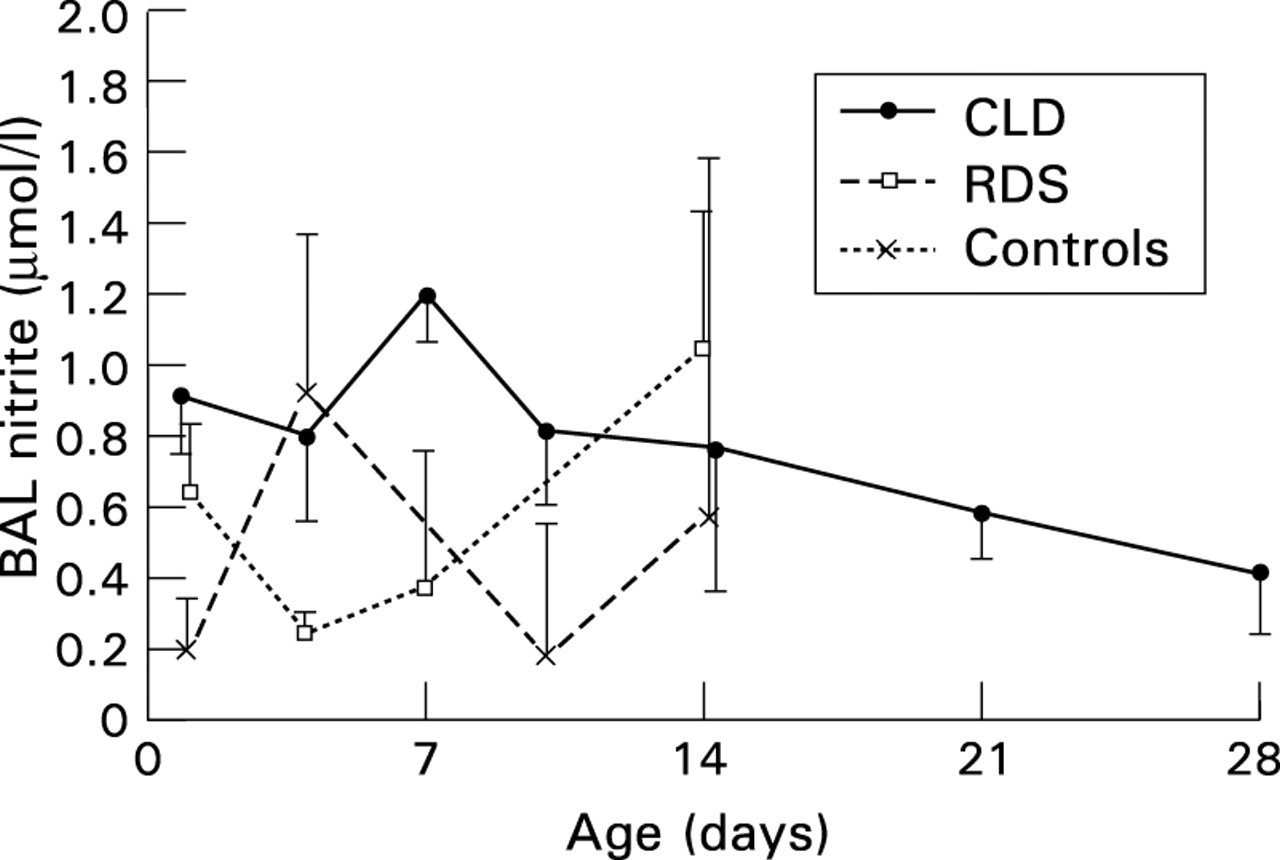
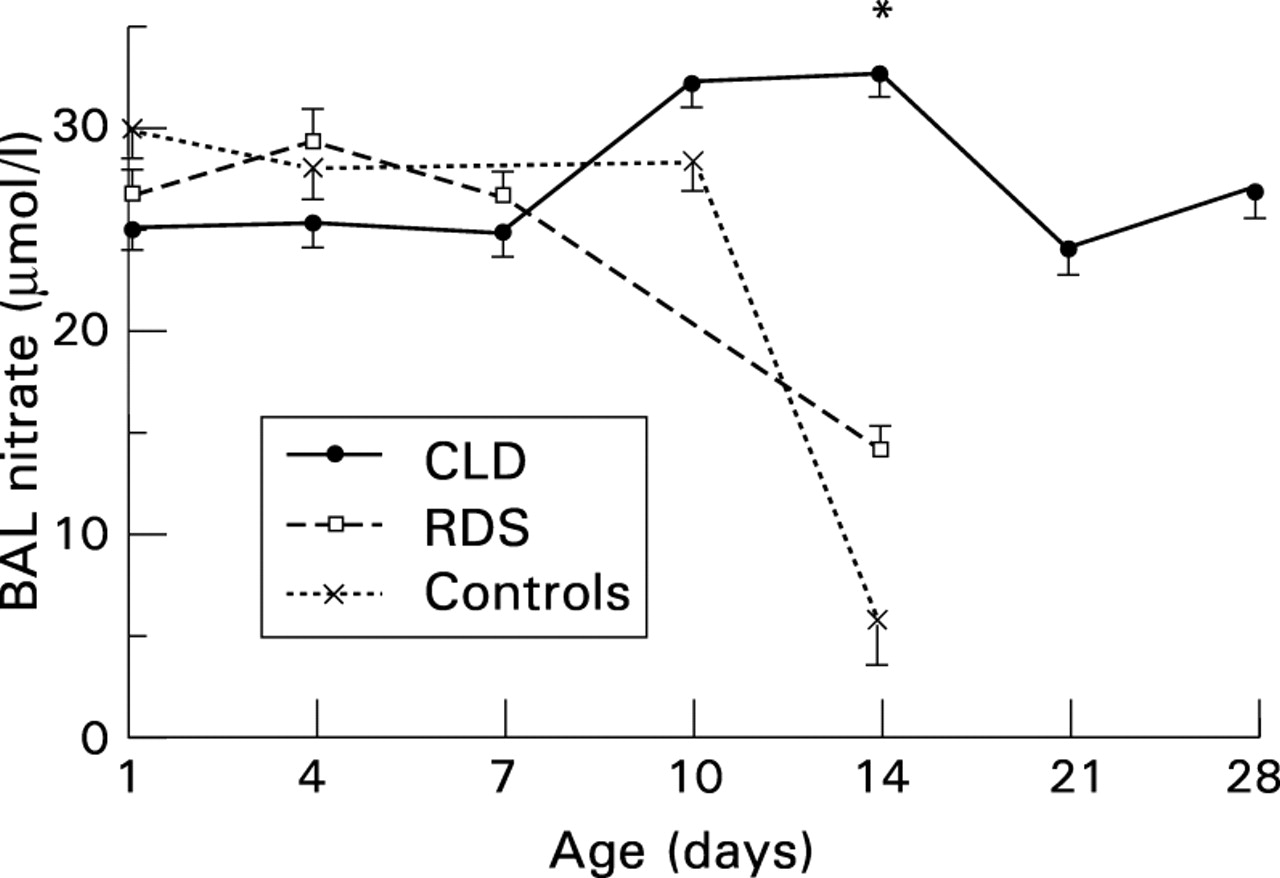
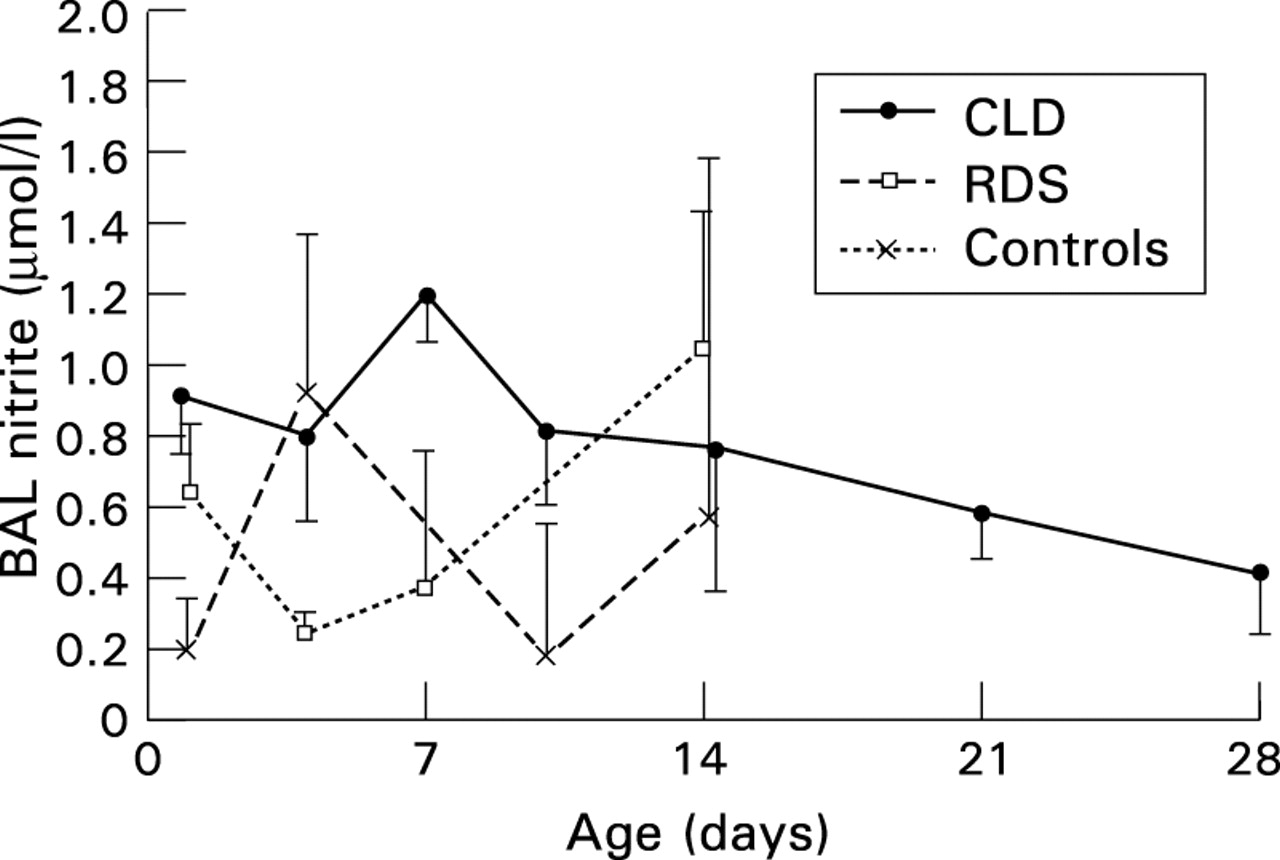
Nitrate concentration in BAL fluid for all three groups during the first week of life was between 25 and 30 μmol/l with little differences seen between the groups (fig 1). By 14 days of age, the concentration of nitrate in lavage fluid had decreased in the RDS and control groups to 14.2 μmol/l and 5.5 μmol/l, respectively. In contrast, it remained at around the same level in the CLD group until 28 days of age (31.3 μmol/l at day 14, p<0.05 compared with the RDS and control groups. The mean concentration of nitrite in BAL fluid obtained from all three groups throughout the study period was less than 1.2 μmol/l with no differences noted between the groups (fig2).

Mean (SEM) nitrate concentration in BAL fluid of infants who developed CLD, infants with RDS nursed in air by day 28, and infants ventilated for non-respiratory reasons (controls); *p <0.05 CLD vs RDS vs controls.
{kind=link}
{kind=link}
Mean (SEM) nitrite concentration in BAL fluid of infants who developed CLD, infants with RDS nursed in air by day 28, and controls.
Discussion
The results have shown that nitrate concentration in BAL fluid from all three groups was very similar during the first week of life. During the second week of life, nitrate concentration remained high in the infants who progressed to CLD. In contrast, it decreased in the RDS and control groups. Nitrite concentration in BAL fluid was less discriminatory between the three groups, being less than 1.2 μmol/l throughout the study period.
The similar concentration of nitrate in all three groups during the first week of life suggests that there is a common cause for its production, independent of gestational age. In animal models NO is thought to have a role in transition of the fetal circulation to the adult circulation.32 33 Abman et al have shown that inhibition of NO synthase by the L-arginine analogue nitro-L-arginine in newborn lambs prevents the normal physiological decrease in pulmonary arterial resistance, suggesting that NO may have a role in the transition from fetal to adult circulation.32 It is tempting to speculate that the nitrate we detected reflects such a circulatory adaptation after birth in all groups. Further studies will be needed to determine if this is indeed the case.
There is evidence that the sensitivity of newborn piglet pulmonary arterial smooth muscle cells to NO increases after day 3 of life; therefore a lower concentration of NO is required for equivalent vasodilatory effect in the pulmonary circulation.33 This observation may explain the decrease in BAL fluid nitrate that we have seen during the second week of life in the RDS and control infants. The persistence of BAL fluid nitrate in the CLD group after the first week may be due to the change in sensitivity of the smooth muscle cells to NO not occurring. This may result in maladaptation of the fetal circulation in this group of babies.
Alternatively, the increase in BAL fluid nitrate in the CLD infants during the second week of life may be due to increased pulmonary inflammation.34 Pulmonary inflammation is increased in the lungs of babies who progress to CLD compared with those babies who recover from RDS.4-9 Certain pro-inflammatory cytokines found in BAL fluid in CLD, and which promote lung inflammation, will probably induce the expression of the inducible form NO synthase (iNOS), as has been shown in asthma35 and sepsis.36 The increase in nitrate in the CLD group during the second week of life may be due to inflammation in the lungs of babies who develop CLD. Further evidence for lung inflammation contributing to the production of NO is provided by animal models. Hyperoxia, which newborn preterm infants who progress to CLD are exposed to, can increase the production of nitrate and nitrite in the lungs of animals.37 In Arkovitz’s model, inhibition of NO synthase (NOS) by L-NG-nitro-L-arginine methyl ester (L-NAME) worsened hyperoxic acute pulmonary injury, suggesting that NO may protect the lungs from such injury. However, the mechanism of increased nitrate and nitrite production in BAL fluid with hyperoxia is unclear as iNOS expression was not increased. It may be that there is a balance of beneficial against adverse effects of NO depending on other prevailing factors.
In the inflammatory environment of the lung of infants who develop CLD, endogenously produced NO, as shown by our study, is likely to react with reactive oxygen species to form pro-oxidant products such as peroxynitrite. Peroxynitrite is an unstable product which rapidly nitrates tyrosine residues to form nitrotyrosine.38Nitrotyrosine has been used as a marker of the presence of peroxynitrite in many inflammatory disorders, including rheumatoid arthritis.39 adult RDS,40 and atherosclerosis.41 Further preliminary studies by our group have shown that infants who develop CLD (and who are not treated with inhaled NO) have increased nitrotyrosine in proteins obtained from BAL fluid (data not shown). This finding has been confirmed by others.42 More importantly, the formation of nitrotyrosine may interfere with phosphorylation of tyrosine residues in critical cell signalling pathways which result in cell proliferation and differentiation.43
We were unable to show any differences between the groups for BAL fluid nitrite. This is likely to have been due to either the instability of nitrite which is readily converted to nitrate in the oxygen enriched environment of the infant receiving oxygen treatment or due to oxidation to nitrate in storage even at −70OC. Other commonly encountered problems with studies such as ours include regular extubation of study infants as their clinical condition improves, the lack of a satisfactory marker for dilution of epithelial lining fluid,44 and difficulty of obtaining “normal” data for preterm infants.
In conclusion, our data show that, during the first week of life, nitrate in BAL fluid from ventilated infants was similar in all three groups studied. This suggests that NO may have a role in the transition of the fetal circulation to the postnatal circulation. Pulmonary NO production seems to persist in infants who develop CLD, possibly reflecting maladaptation of the pulmonary circulation in these infants, or ongoing pulmonary inflammation.
Acknowledgments
Dr Vyas was supported by the British Lung Foundation and Dr Andrew Currie by Action Research.
We thank the parents and nursing staff on the neonatal unit at the Leicester Royal Infirmary.
Data from this work formed part of an oral presentation at the 1998 American Thoracic Society, annual meeting, Chicago, USA.