Article Text

Abstract
A census of activity and staff levels in 1996 was conducted in UK neonatal units and achieved a 100% response from 246 units. Among the 186 neonatal intensive care units, the median (interquartile range) number of total cots was 18(14−22); level 1 intensive care cots 4(2−6); total admissions 318(262−405); very low birthweight admissions 40(28−68); and the number ventilated or given CPAP by endotracheal tube 52(32−83). Forty six (25%) intensive care units lacked the recommended minimum of one consultant with prime responsibility for neonatal medicine. As a conservative estimate 79% of intensive care units had a lower nursing provision than that recommended in previously published guidelines. There was substantial variation in activity and staffing levels among units.
- staff numbers
- intensive care units
- risk adjusted outcomes
Statistics from Altmetric.com
On behalf of the British Association of Perinatal Medicine (BAPM), Milligan1 surveyed neonatal intensive care provision in the UK for 1992–93; the response rate reached 84%. He reported increased numbers of intensive care level 1 cots and increased intensive care activity compared with 1989. However, contrary to contemporary policy initiatives, most of the neonatal intensive care activity was delivered in small or medium sized units.
In 1996 the BAPM2 offered guidance on organisation and standards, and recommended that units offering neonatal intensive care should have total level 1 and level 2 activity of over 500 intensive care days per year. However, BAPM also emphasised the need to obtain evidence that implementation of the standards, including the still contentious issue of size and throughput of units, would improve outcomes. The UK Neonatal Staffing Study aims to address this issue and we report here the results of the first census phase.
We achieved responses from every UK neonatal unit, describing patient volume, activity levels and throughput, nurse and medical staff numbers. These results gave a complete sampling frame for a stratified random sample of UK neonatal intensive care units for the second prospective phase. That second phase will consider the relation between the directly alterable characteristics of size, staffing levels and workload and risk adjusted mortality and morbidity.
Methods and results
Of the 250 UK hospitals surveyed in 1997, three had closed and two had merged. All remaining 246 units returned questionnaires using their most recent annual data available (98% for 1996, 2% for 1995). One hundred and eighty six (76%) were categorised as neonatal intensive care units because they reported providing sustained neonatal intensive care as well as special care. The remaining 60 (24%) were special care baby units which provided only temporary intensive care before transfer to a neonatal intensive care unit.
ACTIVITY
The reported cot establishment and descriptions of unit activity for 186 neonatal intensive care units are summarised in table 1. Definitions used to measure ventilation activity varied between units, both for the total number of infants ventilated or given continuous positive airway pressure (CPAP) and for the total counts of ventilated days. A few units counted ventilation activity only as that delivered by endotracheal tube, whereas most included other respiratory support, such as that delivered by nasal prongs or face mask. Thus the most complete, comparable, and robust proxy measure available of neonatal intensive care activity was total annual admissions of very low birthweight (VLBW) babies. With the development and adoption of the BAPM neonatal dataset, for annual reporting of data for neonatal intensive care units,3 more reliable data will be routinely available for future comparisons of unit based activity and staffing.
Reported cot establishment and activity levels in UK neonatal intensive care units
STAFFING
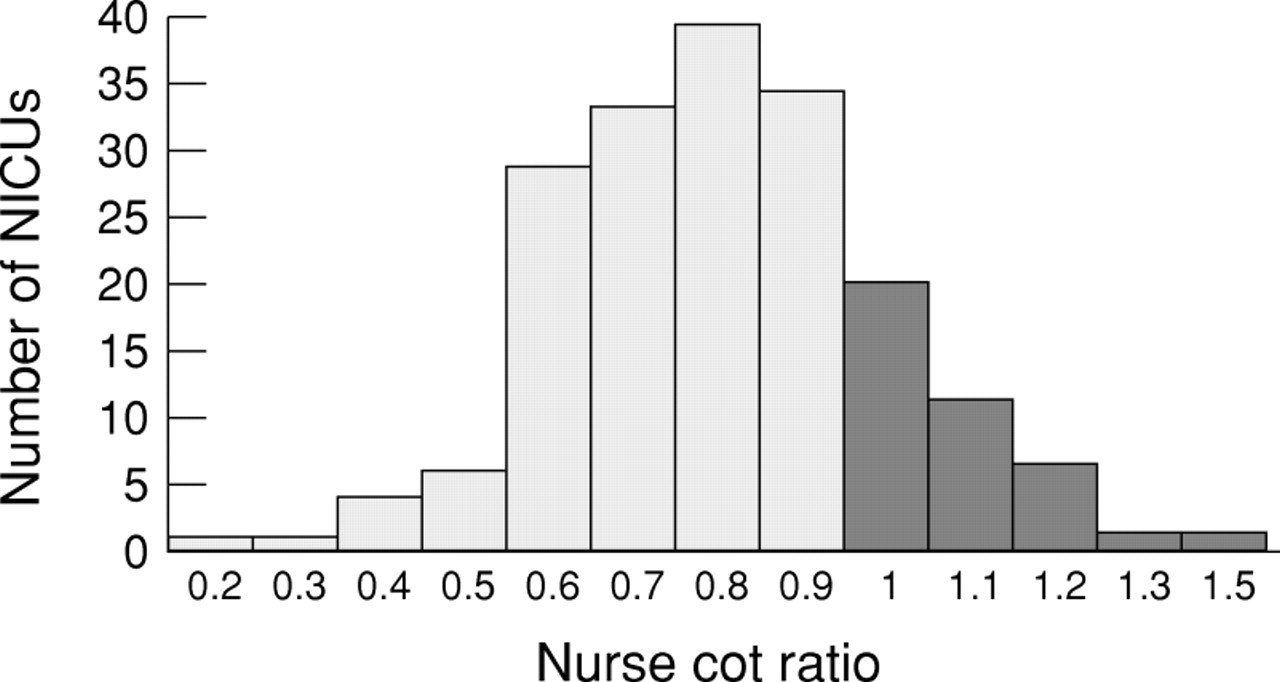
Forty six (25%) neonatal intensive care units lacked the recommended minimum of one consultant1 with prime responsibility for neonatal medicine (measured as >50% of clinical sessions dedicated to neonatal care). The trained and qualified nurse staffing establishment proposals of 19924 were 5.5 whole time equivalent (WTE) nurses per level 1 intensive care cot, 3.5 per level 2 intensive care cot, and one per special care cot. We used more conservative assumptions (fig 1) for two reasons. Firstly, this census did not distinguish between level 2 intensive care cots and special care cots, and secondly it did not distinguish between trained nurses, those with additional qualifications in neonatal specialty, nursery nurses and auxiliaries. A ratio of 1.0 indicates reported nursing establishment provision equivalent to the calculated requirement: 79% (147/186) of neonatal intensive care units had ratios <1.0, varying from 0.3–1.5 (median 0.84, IQR 0.73–0.98) (fig 1).

{kind=link}
Nurse:cot ratios in all UK neonatal intensive care units (actual/recommended numbers of WTE nurses).
Nurse:cot ratios (fig 1) were calculated using the following formula: WTE/(5.5 × ICL1+SC), where WTE is observed total whole time equivalent nurses in the establishment, including trained, qualified nurses and auxiliary or nursery nurses; ICL1 = total level 1 intensive care cots; and SC = total number of other cots, such as level 2 intensive care cots and special care cots. Seventy nine per cent of neonatal intensive care units had a nurse:cot ratio < 1, indicating lower provision than that required by our conservative interpretation of the 1992 guidelines. The calculation underestimates the deficit between actual and recommended numbers of nurses, as it equates trained, qualified, and untrained nurses, and level 2 intensive care with special care cots.
Comment
These results show continuing and substantial variation in neonatal intensive care unit activity and staff numbers.1Despite conservative assumptions in our calculation, we noted divergence between actual and calculated nurse requirement. Similar wide variation has been described by Redshaw and colleagues.5 The reasons for the variation in levels of activity probably include different admission criteria and inherent differences in case mix. The reasons for divergence in staffing provision could include varying definitions of cot types and categories of care,6 resource constraints, problems in recruitment or retention of staff, and doubts about the validity of the staffing guidelines.4
Whether these observed variations in organisational characteristics are important determinants of outcome remains unknown. It has been suggested that staff may get more experience if activity and specialisation are high,1 but outcomes may deteriorate if staff are overworked. In the second phase of this study risk adjusted outcomes will be assessed prospectively for over 6000 infants from a random sample of 54 neonatal intensive care units, stratified by these census measures of activity (volume of VLBW babies), and medical and nurse staffing numbers. Consistent measures of workload and staffing6 will also be observed and recorded twice daily. The UK Neonatal Staffing Study may provide more reliable evidence to inform policy than has been available before.
Acknowledgments
The UK Neonatal Staffing study is funded by the NHS R&D Executive Mother and Child Health Programme and endorsed by the British Association of Perinatal Medicine, the Neonatal Nurses Association (UK) and Scottish Neonatal Nurses Group. We thank all UK neonatal units for their support. The views expressed in this paper, however, are those of the authors on behalf of the UK Neonatal Staffing Study Group.