Article Text

Abstract
AIMS To evaluate the commonly used markers—namely IL-6, TNFα, IL-1β, C-reactive protein and E-selectin for identification of late onset neonatal sepsis; to define the optimal cutoff value for each marker in preterm neonates; to assess whether these markers could assist in early discontinuation of antibiotics in non-infected cases; and to delineate the profile of these markers during systemic infection and in relation to successful treatment.
METHODS Very low birthweight infants in whom clinical sepsis was suspected when they were >72 hours of age were eligible for study. A full sepsis screen was performed in each episode. Cytokines, C-reactive protein, and E-selectin were serially measured on days 0 (at the time of sepsis evaluation), 1, 2, 4 and 7. The optimal cutoff value for each marker was calculated after minimising the number of misclassified episodes over all possible cutoff values for days 0 and 1. The sensitivity, specificity, positive and negative predictive values for each test and combination of tests for predicting systemic infection were also determined.
RESULTS One hundred and one episodes of suspected clinical sepsis were investigated in 68 infants. Forty five episodes were proved to be infections. The optimal cutoff values were IL-6 31 pg/ml, TNFα 17 pg/ml, IL-1β 1 pg/ml, C reactive protein 12 mg/l and E-selectin 174 ng/ml. IL-6 had the highest sensitivity (89%) and negative predictive value (91%) for detecting late onset infection on day 0. However, between 24 and 48 hours of onset, C-reactive protein was the best single marker, with an overall sensitivity and specificity of 84% and 96%, respectively. The use of serial and multiple markers in the first 48 hours further enhanced the sensitivity and specificity of these tests. Performing IL-6 and C-reactive protein on day 0, together with either TNFα on day 1 or C-reactive protein on day 2, showed the best overall sensitivity (98%) and specificity (91%) for the diagnosis of late onset infection.
CONCLUSIONS Optimal cutoff values for these markers in detecting late onset systemic infection in very low birthweight infants have been defined. Withholding antibiotic treatment at the onset of infection could be fatal and is not recommended, but the concomitant use of IL-6 and C-reactive protein or TNFα should allow antimicrobial treatment to be discontinued at 48 hours without waiting for microbiological results, provided that the infants are in good clinical condition.
- C-reactive protein
- E-selectin
- interleukin 1β
- interleukin-6
- tumour necrosis factor α
- very low birthweight
Statistics from Altmetric.com
Late onset nosocomial bacterial infection and septic shock in preterm very low birthweight (VLBW) infants carry a high risk of morbidity and mortality.1 Early warning signs and symptoms are often non-specific, subtle, and can easily be confused with non-infective causes such as apnoea of prematurity, variation in environmental temperature, and acute exacerbation of chronic lung disease. Although in most cases the onset is often inconspicuous, the clinical course may be alarmingly fulminant, leading to septic shock, disseminated intravascular coagulation, and death within hours of onset. Infected infants must, therefore, be promptly identified and differentiated from non-infected cases, and antibiotic treatment started without delay. As microbiological culture results are not usually available until at least 48–72 hours after the specimen reaches the laboratory, early identification of infected cases is recognised as a major diagnostic problem in VLBW infants. Equally difficult is the exclusion of infection in infants with suspected sepsis. Continuation of antibiotics for presumptive bacterial infection frequently leads to unnecessary treatment. In recent years, haematological and biochemical markers such as immature:total neutrophil ratio,2-4 platelet count,4C-reactive protein (CRP),3 5 and various cytokines6-10 have all been suggested as being useful indicators for early identification of septic infants. Although most studies have shown a positive correlation between these markers and infection, most were performed on newborns with wide ranges of birthweight and gestational age,6-9 involved only a small sample size,8-10 assessed only one or two markers at any one time,3 6 7 10 and did not serially monitor the profile of these markers.7 8 Hence, the best single biochemical marker or combination of markers for the detection of late onset neonatal sepsis in VLBW infants have not been determined.
This study aimed to: (1) evaluate the usefulness of the commonly used biochemical markers, namely, interleukin-6 (IL-6), tumour necrosis factor α (TNF α), interleukin-1β (IL-1β), CRP, and E-selectin, both individually and in combination, for the early identification of late onset neonatal sepsis (>72 hours of age) in preterm VLBW infants. The sensitivity, specificity, positive and negative predictive values of each marker or combination of markers were also determined; (2) to minimise the number of misclassified cases within the first 24 hours of infection over all cutoff values using receiver operating characteristics (ROC), in an attempt to define the optimal cutoff value for each marker in detecting late onset sepsis; (3) to assess whether these markers could assist in the early discontinuation of antibiotic treatment in those infants who were subsequently shown not to be infected; and (4) to delineate the pattern or profile of these markers by serial measurements during systemic bacterial infection, and in relation to successful treatment.
Methods
All VLBW infants with suspected clinical sepsis who were >72 hours of age in the neonatal intensive care unit at the Prince of Wales Hospital during the six months beginning in June 1995, were eligible for study. Signs and symptoms suggestive of clinical sepsis were: unstable temperature (<36.5°C or >37.5°C on two occasions within 24 hours), lethargy, irritability; gastrointestinal dysfunction with milk intolerance, vomiting, abdominal distension or bloody stool; respiratory dysfunction, as evidenced by a progressive increase in ventilator settings or oxygen requirement in a previously stable infant, apnoeic spells, sudden increase in respiratory rate or persistent tachypnoea (>60 breaths/min); cardiovascular dysfunction including sudden increase or decrease in heart rate or persistent tachycardia (>160/min) or bradycardia (<100/min), poor peripheral circulation, prolonged capillary filling time (>3 seconds), hypotension or sudden increase in requirement of inotropic support to sustain a mean arterial blood pressure of 30 mm Hg; and unexplained abnormal biochemical and haematological parameters such as persistent metabolic acidosis (base deficit ⩾10), hyperglycaemia (>10 mmol/l), thrombocytopenia (<100 × 109/l), leucopenia (<5 × 109/l) or leucocytosis (>20 × 109/l) in infants not recently started on dexamethasone treatment.
The infants were recruited into the study at the time of evaluation for suspected clinical sepsis. In each episode, a full sepsis screen was performed which included cerebrospinal fluid (CSF), blood, stool, urine and endotracheal aspirate (infants on mechanical ventilation) cultures for bacteria and fungi; removal and culture of indwelling central lines; and cultures of specific sites and surgical specimens, such as peritoneal swab, abscess, needle aspirate material and biopsy specimen. Chest and abdominal radiographs were routinely performed. Haematological and biochemical laboratory investigations including a complete blood count, differential white cell and platelet counts; arterial blood gases; blood glucose; and the cytokines (IL-6, TNFα, IL-1β), CRP and E-selectin were serially measured. The initial sample was taken on day 0 (at the time of sepsis evaluation) and four further samples taken on days 1, 2, 4 and 7 for monitoring the clinical progress and response to treatment. This schedule of blood sampling coincided exactly with our unit policy for serial blood count and CRP measurements after a suspected episode of infection had been identified. Parenteral antibiotics were started immediately after the infection screen and the first set of blood sample had been performed.
CLASSIFICATION OF “INFECTIVE” EPISODES
Three categories of “infective” episodes were prospectively defined:
Group 1 The infected group consisted of episodes that had been confirmed as septicaemic from positive blood cultures when the same organism was isolated from both blood culture bottles, and each isolate showed an identical pattern of antibiotic sensitivity and biochemical profile. Pneumonia was diagnosed on the basis of changes in the quality and an increase in the quantity of pulmonary secretions, plus chest radiograph abnormalities compatible with pneumonia and isolation of a predominant organism from at least two bronchopulmonary lavage specimens. Microbiologically confirmed infections other than septicaemia, such as peritonitis, meningitis, systemic fungal infection, and necrotising enterocolitis (stage II or above in Bell’s classification11 with or without positive blood culture) were also included.
Group 2 The non-infected group consisted of episodes which met the initial screening criteria for suspected clinical sepsis but were subsequently found not to have positive bacterial or fungal cultures in blood, cerebrospinal fluid or urine specimens; radiological evidence of pneumonia or necrotising enterocolitis; and the infant continued to improve after antibiotic treatment was stopped.
Group 3 The control group consisted of blood samples taken from 20 well, preterm, VLBW infants between weeks 1–8 for cytokines, C reactive protein, and E-selectin measure ments. The collection of these blood samples coincided with the weekly routine screening of haemoglobin concentration and liver function.
Blood samples obtained from an indwelling arterial line or venepuncture were transferred into chilled containers containing heparin. These specimens were immediately immersed in ice and transported to the laboratory for processing. Plasma was separated by centrifugation at 4°C and stored in 200 μl aliquots at −80°C until analysis. Plasma C reactive protein concentrations were measured by a turbidity assay against control standards, as specified by the manufacturer (Behring Diagnostics Inc., Westwood, MA, USA). Plasma IL-6, TNFα, IL-1β, and E-selectin concentrations were measured using the commercially available enzyme linked immunoassay kits (R & D System Inc., Minneapolis, MN, USA). The interassay and intra-assay variability were within the 5% limits specified by the manufacturers.
STATISTICAL ANALYSIS
Results of the three groups were compared using the Wilcoxon rank sum test and Fisher’s exact test where appropriate.
The sensitivity and specificity for all possible cutoff values were calculated for days 0 and 1 to construct the receiver operating characteristic curves for each biochemical marker. This allowed these markers to be compared, regardless of the selected or recommended diagnostic cutoff values which were not well defined in preterm VLBW infants. From these curves, the best or optimal cutoff value for each biochemical test was determined by minimising the number of misclassified episodes over this period. The calculation was based on the assumption that a false positive result is of equal importance to a false negative result. The sensitivity, specificity, positive and negative predictive values were worked out using the optimal cutoff values, to allow the selection of the best combination of tests at the most appropriate sampling times for the diagnosis of late onset sepsis in VLBW infants. For the purpose of this study, a combination of tests was judged positive if any one of the selected markers, within the specified time period, exceeded their respective optimal cutoff values.
The study was approved by the Research Ethics Committee of the Chinese University of Hong Kong. Informed consent was obtained from the parents or guardians for all study patients.
Results
The clinical characteristics of the study groups are summarised in table 1. There were no significant differences between gestational age, birthweight, Apgar scores <7 at 1 and 5 minutes, or male:female ratio between the three groups (p>0.10, Wilcoxon rank sum test and Fisher’s exact test where appropriate). Infection episodes, however, occurred significantly later than non-infection episodes (p<0.005, Wilcoxon rank sum test).
Clinical characteristics of the study populations
One hundred and one episodes of suspected clinical sepsis were investigated in 68 preterm VLBW infants. One, nine, and 12 patients had infection screens performed four, three, and two times, respectively. The remaining 46 infants had only one sepsis screen. Forty five of 101 episodes of suspected infection were confirmed, of which 25 (55%), 12 (27%), four (9%) and four (9%) were due to Gram positive, Gram negative, fungal, and unidentified organisms, respectively. One infant died of Enterobacter sp septicaemia. Detailed accounts of the pathologies and organisms are summarised in table 2.
Characteristics of the episodes of infection (n=45)
BIOCHEMICAL MARKERS
Profile
In episodes of confirmed infection all biochemical markers except C reactive protein reached their peak plasma concentrations at the time of evaluation for suspected clinical sepsis (day 0). In contrast, the maximum C reactive protein response occurred around 24 hours after onset (day 1). Thereafter, the plasma concentrations of all biochemical markers decreased progressively with time and successful treatment (figs 1A–E). All five biochemical markers in the infected group were significantly increased when compared with the corresponding values of the non-infected group on days 0–4 (p<0.005, Wilcoxon rank sum test). The concentrations of TNFα, C reactive protein, and E-selectin remained significantly increased on day 7 in the infected group (p<0.05, Wilcoxon rank sum test). Likewise, the plasma concentrations of all biochemical markers in the infected group on the first four days were significantly higher than in the control group (p<0.02, Wilcoxon rank sum test). In contrast, no significant differences were detected between the non-infected group and controls (p>0.10, Wilcoxon rank sum test).

(A–E) Plasma concentration of the biochemical markers during the first seven days of suspected infection. Each figure compares the range of a biochemical marker between the infected and non-infected episodes. Data are expressed as median, 25th, and 75th percentiles. Bold line and upper and lower boundaries of the shaded area represent 50th, 75th, and 25th percentiles, respectively, of the infected episodes. Asterisks and thinner lines and their upper and the lower boundaries of the 50th, 75th, and 25th percentiles, respectively, of the non-infected episodes. The vertical axis of Il-6 (A) is in a logarithmic scale.
Comparison of tests
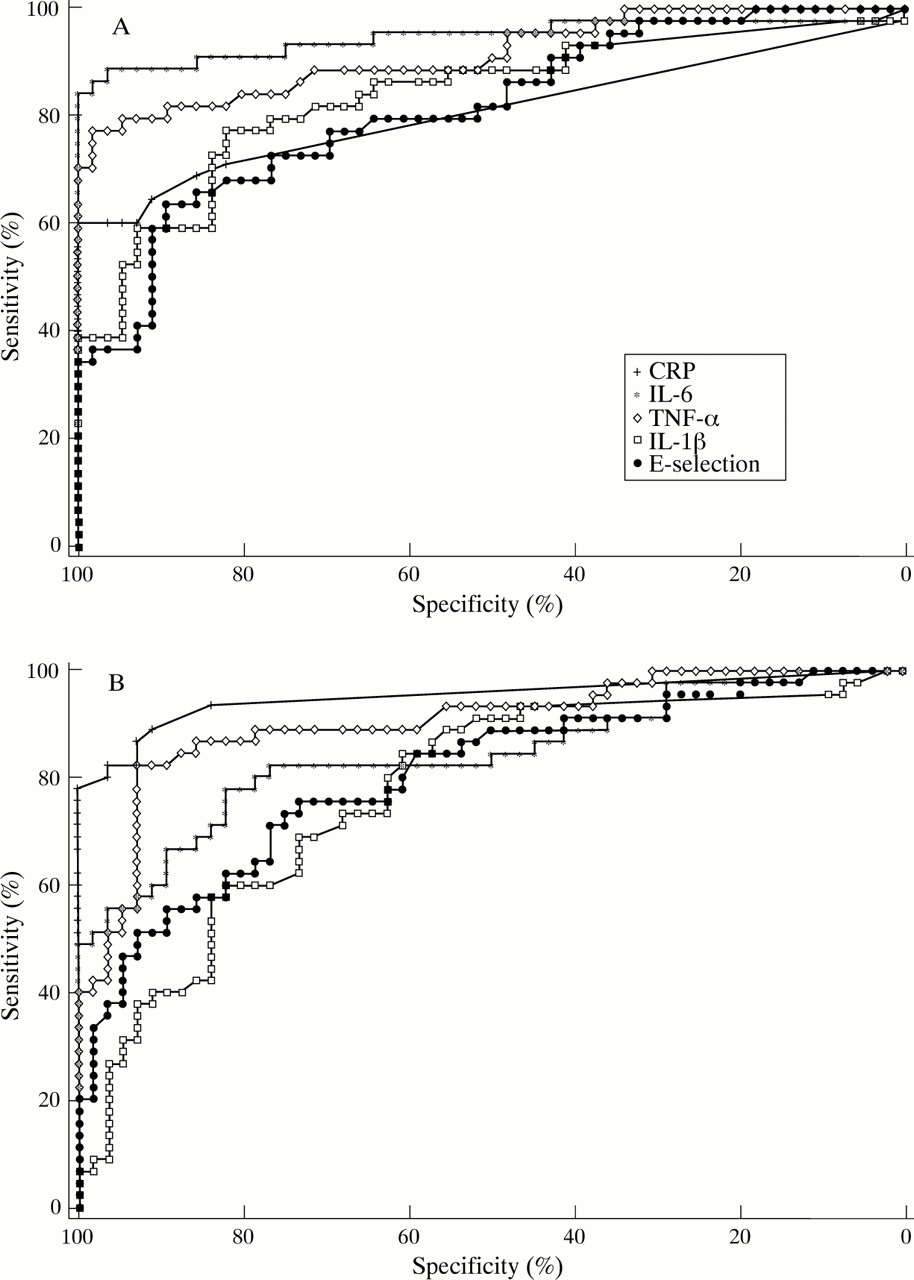
Table 3 summarises the sensitivity, specificity, positive and negative predictive values of the five biochemical markers and combination of these markers, using the cutoff values recommended by the manufacturers (IL-6 13 pg/ml, TNFα 16 pg/ml, IL-1β (4 pg/ml, CRP 10 mg/l and E-selectin 64 ng/ml), and the optimal cutoff values (IL-6 31 pg/ml, TNFα 17 pg/ml, IL-1β 1 pg/ml, CRP 12 mg/l and E-selectin 174 ng/ml), calculated by minimising the number of misclassified episodes over all possible cutoff values for days 0 and 1. The ROC curves of each biochemical parameter for days 0 and 1 are shown in figs 2A and B, respectively.
Comparison of the sensitivity, specificity, positive and negative predictive values of the biochemical tests using the calculated optimal cutoff values and the manufacturers’ recommended values (in parentheses) during the first 48 hours of suspected clinical sepsis

{kind=link}
{kind=link}
Receiver operating characteristics of the biochemical markers on days 0 (A) and 1 (B).
A comparison of each individual test using the optimal cutoff values showed that IL-6 has a higher sensitivity and negative predictive value for detecting late onset infection in VLBW infants than all other biochemical markers on the day of onset of infection (table 3). Although C reactive protein is highly specific, it had a relatively low sensitivity on day 0. The situation, however, changed in the next 24 and 48 hours with C reactive protein having the best overall sensitivity and specificity (table 3). TNFα was also a sensitive marker and simulated the characteristics of IL-6. In contrast, IL-1β and E-selectin had rather low sensitivity for detecting infection within the first 48 hours (table3).
A comparison of the sensitivity, specificity, positive and negative predictive values of the best three markers—namely, IL-6, TNFα and C reactive protein in combination, with those of individual markers—suggested that the use of multiple markers was associated with higher sensitivity and better negative predictive values (table 3). In particular, the use of C reactive protein with either IL-6 or TNFα seemed to be most sensitive for confirming infection (table 3). Furthermore, if these markers were serially monitored, the sensitivity and negative predictive value of these tests were further enhanced. After calculating all possible combinations and permutations for these three tests within the first 48 hours of infection, C reactive protein and IL-6 on day 0 combined with either TNFα on day 1 or C reactive protein on day 2 provided the best overall sensitivity (98%) and specificity (91%) for the diagnosis of late onset infection in VLBW infants. Table 4 summarises the permutations of these tests with the highest sensitivity and negative predictive value. The addition of further tests either on days 1 or 2 did not seem to improve the sensitivity and negative predictive value, but significantly lowered the specificity and positive predictive value.
Comparsion of the sensitivity, specificity, positive and negative predictive values of different combinations of biochemical tests using the calculated optimal cut off values and the manufacturers’ recommended values (in parentheses) during the first 48 hours of suspected clinical sepsis
Discussion
Cytokines (IL-6, TNFα, and IL-1β), an adhesion molecule (E-selectin), and a commonly used acute phase reactant protein (C reactive protein) were serially measured in this study in an attempt to identify a set of tests which can reliably confirm or refute the diagnosis of systemic infection at an early stage. As the optimal diagnostic cutoff values for these tests in preterm VLBW infants have not been defined, we first attempted to determine the best cutoff values by minimising the number of misclassified cases on days 0 and 1, and demonstrated using the ROC curves (figs 2A and B) that the IL-6, TNFα, IL-1β, C reactive protein and E-selectin values of 31 pg/ml, 17 pg/ml, 1 pg/ml, 12 mg/l and 174 ng/ml, respectively, are best suited to be the optimal diagnostic cutoff points for this cohort of preterm infants. These values are very similar to those recommended by the manufacturers (IL-6 13 pg/ml, TNFα 16 pg/ml, IL-1β 4 pg/ml, C reactive protein 10 mg/l and E-selectin 64 ng/ml), and in keeping with the results of other recent studies.5 8 12
We also delineated the characteristic patterns and profiles of these tests during the first week of infection and in response to successful treatment (figs 1A–E). Early in the course of neonatal sepsis, IL-6 was produced rapidly7 9 and peaked on day 0, but its half life was short13 and could fall back to its baseline value within 24 hours. This specific property of IL-6 rendered it useful as a very early alarm hormone, but because of its short half life, clinicians could not rely on this marker alone for the diagnosis of infection, because in most circumstances it was uncertain at which stage of infection blood was taken for IL-6 determination. In contrast, the peak concentration of C reactive protein occurred slightly later and it was highly specific for confirming infection (table 3). Hence, an abnormally increased C reactive protein with normal plasma IL-6 concentration in an infected infant suggests that the infection has been present for 24 to 48 hours. TNFα behaved similarly to IL-6 and had relatively good sensitivity and specificity on days 0 and 1. IL-1β and E-selectin, however, were less satisfactory markers. Unlike older children and adults, newborn infants have relatively little or no febrile response to infection.14 Our data indicate that the plasma concentrations of IL-1β in infected infants were remarkably low (fig 1D) when compared with those of adult septic patients (120–1500 pg/ml).15 16 It seems that the monocytes of preterm infants may be unable to secrete adequate IL-1β for mounting a febrile response during sepsis and hence, not surprisingly, IL-1β was a comparatively insensitive marker of neonatal infection. Although high plasma concentrations of E-selectin have been associated with severe organ dysfunction and irreversible damage to endothelium and end organs in adult septic patients,17 high values (>500 ng/ml) were predominantly observed in VLBW infants with severe Gram negative septicaemia (6 of 12 cases) and multiorgan failure rather than in Gram positive infection (1 of 25 cases). However, its overall sensitivity and specificity were poor (table 3).
Considering the high mortality and potential morbidity associated with neonatal sepsis, diagnostic tests with high sensitivity and negative predictive value are most desirable because all septic infants have to be identified. The lack of reliable clinical signs and laboratory tests often results in anticipatory antimicrobial treatment. In order to minimise the unnecessary use of antibiotics in false positive cases, tests need to have a reasonably high specificity and good positive predictive value. We found that the use of serial and multiple diagnostic tests at appropriate times significantly improved our diagnosis of infection. Measuring IL-6 and C reactive protein on day 0, together with either TNFα on day 1 or C reactive protein on day 2 (table 4) gave the best sensitivity (98%) and specificity (91%) for the diagnosis of late onset infection. Introducing more frequent or additional tests into the regimen did not improve the sensitivity but adversely affected the specificity of these tests.
Only one of 45 infected cases was not positively identified, as none of the markers was increased within the first seven days of infection (IL-6 <6.4 pg/ml, TNFα <12 pg/ml, IL-1β <0.64 pg/ml, C reactive protein <5 mg/l, and E-selectin <66 ng/ml). This infant had intermittent fever (37.8°C) and was found to have fungal ventriculitis. The ventricular fluid grew Candida albicans(only one colony isolated) and the cranial ultrasound scan demonstrated a web-like structure in the lateral ventricles, probably indicating the chronic nature of the infection. We postulated that the localised and possibly chronic low grade nature of the infection were the main reasons for the persistent normal plasma values observed. Obviously in this case, performing more frequent tests would not have improved the sensitivity or specificity. By contrast, five episodes of non-infection were misclassified as infections. Four of the five cases had only marginal increase in plasma inflammatory markers (IL-6 <59 pg/ml, TNFα <30 pg/ml, C reactive protein <14 mg/l), but the fifth case had very high plasma IL-6 and C reactive protein concentrations (248 pg/ml and 81 mg/l, respectively), caused by ventriculo-peritoneal shunt surgery 20 hours before blood sampling.
In conclusion, we have determined the optimal cutoff value for each biochemical marker in a cohort of preterm VLBW infants, and have thus provided a model with which future studies could be compared. The sensitivity, specificity, positive and negative predictive values of these tests depend to some extent on the cutoff point chosen for each test. Our optimal cutoff values for IL-6, TNFα, and C reactive protein are similar to those defined for normal healthy adults and suggest that the biochemical pathways (except IL-1β) are mature at these early gestational ages. Serial determination of IL-6 and C reactive protein are particularly useful in the management of late onset nosocomial systemic infection. IL-6 is a highly sensitive early alarm hormone and C reactive protein is a very specific late marker of infection. Thus in the clinical setting IL-6 and C reactive protein in the first 48 hours of infection should be the ideal combination for early diagnosis of neonatal bacterial sepsis. Withholding antibiotic treatment at the onset of infection could be fatal and is not recommended, but the high sensitivity (98%) and negative predictive values (98%) of IL-6 and C reactive protein indicated that antibiotics could be confidently discontinued at 48 hours without waiting for microbiological results, provided that the infants are in good clinical condition. The high specificity (91%) of this combination also suggested that only 9% of infants suspected of having an infection were unnecessarily treated with antibiotics. Moreover, if the results were interpreted with care and in combination with the clinical history, such as recent surgery or vaccination, it would allow even more precise classification of infected and non-infected cases. Although IL-1β and E-selectin were poor predictors of sepsis, high plasma concentration of E-selectin were more commonly associated with Gram negative septicaemia and end organ dysfunction.