Article Text

Abstract
Fifty preterm infants weighing 1200 g or more with clinical and radiographic evidence of respiratory distress syndrome, requiring both mechanical ventilation and exogenous surfactant replacement, were randomly allocated to receive either volume controlled ventilation or time cycled, pressure limited ventilation. Tidal volume delivery in each group was deliberately controlled at 5–8 ml/kg so that the only difference between the two groups was the ventilatory modality, the manner in which tidal volume was delivered. The rest of the ventilatory management and clinical care was done according to protocol. The two modes of ventilation were compared by determining the time required to achieve pre-determined success criteria, based on either the alveolar–arterial oxygen gradient or the mean airway pressure as a standard against which the speed of weaning could be objectively assessed. Infants randomised to volume controlled ventilation met success criteria sooner and had a shorter duration of mechanical ventilation. These babies also had a significantly lower incidence of intraventricular haemorrhages and abnormal periventricular echodensities on ultrasound scans.
Volume controlled ventilation seems to be both safe and effective in this group of patients.
- assisted ventilation
- alveolar–arterial oxygen gradient
- mean airway pressure
- respiratory distress syndrome
Statistics from Altmetric.com
- assisted ventilation
- alveolar–arterial oxygen gradient
- mean airway pressure
- respiratory distress syndrome
Assisted mechanical ventilation of preterm newborns with respiratory failure has traditionally been accomplished using time cycled, pressure limited (TCPL) devices over the past three decades, primarily because of their ease of application and relative safety. However, the recent introduction of newer, microprocessor based mechanical ventilators now gives clinicians the opportunity to provide ventilatory support in various ways which were not previously available. One of these modes, volume controlled ventilation (VC), differs from TCPL in that the primary gas delivery target is tidal volume, and peak inspiratory pressure may vary from breath to breath. Earlier attempts at VC ventilation of the newborn in the 1970s and 1980s were severely hampered by technological limitations, especially the inability to monitor accurately the relatively small tidal volumes required by newborns, and the technique was largely abandoned. Recent technological advances in microprocessor based respiratory technology, improved flow, and pressure transducers, and reliable and accurate monitoring and data displays have produced substantial improvements in ventilator performance, allowing the safe application of VC ventilation to infants as small as 1200 g.1 2 The purpose of this clinical trial was to compare the safety and efficacy of VC ventilation with that of TCPL ventilation in a population of preterm infants with respiratory distress syndrome (RDS) who weighed more than 1200 g.
Methods
The clinical trial was performed in the neonatal intensive care unit at South Cleveland Hospital after approval by the district ethics committee. Infants were deemed eligible for participation if they weighed 1200 g or more at birth and had RDS severe enough to warrant assisted mechanical ventilation and exogenous surfactant replacement. The diagnosis of RDS was based on a composite of clinical and radiological criteria along with evidence of pulmonary insufficiency according to arterial blood gas analysis. Babies with confirmed or suspected sepsis/pneumonia, congenital malformation, or lack of arterial access were excluded.
Success outcome criteria for this trial were determined a priori, and consisted of either AaDO2 <13 Kpa (100 torr), or a mean airway pressure <8.0 cm H2O maintained for at least 12 hours. If successful (>12 hours) extubation occurred, either inadvertently or as a part of clinical management before reaching success criteria; this was also regarded as an end point. The period of mechanical ventilation from the time of entry into the study until achievement of success criteria, as well as the total duration of mechanical ventilation was calculated for each baby. Secondary outcome measures were also noted and included complications frequently associated with mechanical ventilation, such as intraventricular haemorrhage (IVH), periventricular leucomalacia (PVL), patent ductus arteriosus (PDA), and chronic lung disease or bronchopulmonary dysplasia (BPD), defined as oxygen dependency beyond the 36th postconceptional week with suggestive radiological changes.
Informed parental consent was obtained for each patient before enrolment in the study. Assignment of ventilatory mode was done by block randomisation using sealed envelopes. Once randomised, the mode of ventilation was not allowed to cross over. If deemed necessary, on the basis of severe respiratory failure characterised by AaDO2 >80 Kpa (600 torr), oxygenation index >25, or intractable air leak, high frequency oscillatory ventilation (HFOV) was an option. However, analysis of data was done on an intention to treat basis, based on the originally assigned mode. We hypothesised that infants assigned to VC would require 33% less time to achieve the success end points and determined that 50 patients would be required to demonstrate significance (<0.05) with a power of 0.8.
Fifty consecutive patients were assigned to either VC or TCPL ventilation. Both groups were ventilated with the VIP bird Infant/Paediatric Ventilator (Bird Products Corp., Palm Springs, California, USA). This permitted monitoring of proximal airway inspiratory and expiratory tidal volumes, breathing rate, and minute ventilation. All babies in the study were initially placed in the PTV (assist/control) setting to assure adequate minute ventilation and the lowest possible work of breathing. The triggering mechanism for each mode is slightly different: VC is pressure triggered, requiring a 1.0 cm H2O deflection below baseline, whereas TCPL is flow triggered, requiring a 0.2 LPM change in airway flow.
Infants were managed with a standardised unit clinical protocol (table1). In both groups we deliberately controlled the tidal volume delivery at 5–8 ml/kg.3 By matching tidal volume, the only difference between the two groups was the ventilatory modality, or in other words, the manner in which flow was delivered. Infants in the TCPL group received fully synchronised ventilation by using termination sensitivity, which is an expiratory trigger.1 Babies in the VC group were weaned using pressure support ventilation because of its striking similarity to flow synchronised assist/control: it is flow cycled, pressure limited, and patient triggered.4 Weaning in the two modes was thus very similar. All remaining clinical care was provided according to routine ward practices and included intravenous caffeine administration during the process of weaning, routine cranial ultrasound scans, and colour Doppler echocardiography. Clinical information relevant to the study was recorded prospectively for each infant. The timing of chest radiographs on babies in the study was governed by clinical practice. However, the final radiological assessment of the severity of the lung disease and complications was done by the study radiologist (MM) who was unaware of the mode of ventilation at the discharge of each patient. A modified scoring system was used for each lung, with special reference to parenchymal opacities, pulmonary interstitial emphysema, and gross air leaks requiring pleurocentesis.5 6 The final grade was that assigned to the worst radiographic appearance.
Ventilatory management protocol
Results
Three infants in each group required a change in ventilatory mode on clinical grounds during the study. Three infants in the VC group and two in the TCPL group received high frequency oscillatory ventilation; one infant in the TCPL group was crossed over to VC in error and responded to treatment. One baby in each group failed to survive despite rescue treatment. The two groups were demographically nearly identical (table 2). No significant differences were found in any of the parameters examined. Antenatal corticosteroid administration occurred with equal frequency. The degree of respiratory illness in each group at study entry, as assessed by comparison of the AaDO2, mean airway pressure, oxygenation index, and initial radiographic scores, was also similar.
Clinical/demographic results
Infants randomised to the VC group achieved success criteria faster than those randomised to the TCPL group, with a mean time of 65.6vs 125.6 hours; p<0.001, Wilcoxon Rank Sum test (table3). Four infants in the VC group and eight infants in the TCPL group achieved one of the success criteria simultaneously with extubation. The total duration of mechanical ventilation was also significantly shorter in the VC group compared with the TCPL group (mean time 122.4vs 161.9 hours, p<0.001; Wilcoxon Rank Sum). No infant in either group required reintubation.
Study results
Among the secondary outcome measures, the frequency of major scan abnormality (large IVH, ventriculomegaly, and intraparenchymal echodensities), was lower, with none found in the VC group and five found in the TCPL group (p=0.5, Fisher’s exact test). There was less bronchopulmonary disease in the VC group (1 vs 6), but this did not reach significance (p=0.09; Fisher’s exact test). There were also no significant differences in the incidence of air leaks or patent ductus arteriosus requiring intervention.
Discussion
In this clinical trial of VC vs TCPL ventilation in a closely matched population of preterm infants weighing more than 1200 g at birth, infants randomised to VC ventilation achieved the arbitrary success criteria faster than infants randomised to TCPL, with an approximate 50% reduction in ventilated hours. Although 96% of the infants in each group survived, the frequency of major abnormalities seen on ultrasound brain scans and bronchopulmonary disease was less in infants treated with VC. Because of the relatively small number of patients with these complications, the findings should be interpreted with caution.
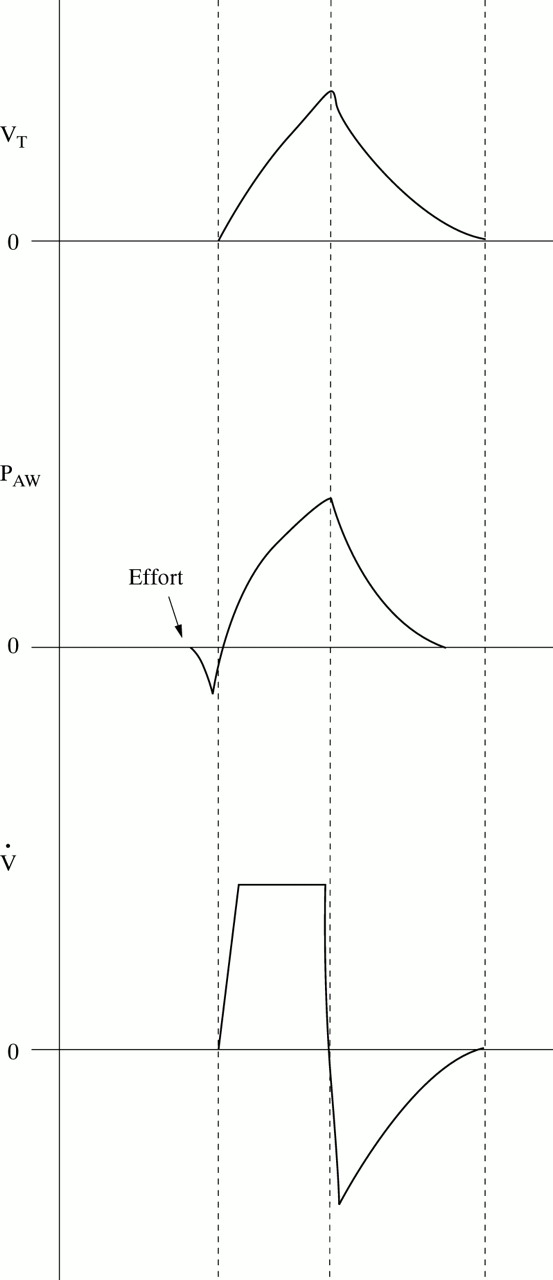
Features of VC include an additional demand flow system designed to augment the continuous flow, a square flow waveform, and consistent tidal volume delivery despite variable peak inspiratory pressure.7 TCPL ventilation is continuous flow with a sharp or spike flow waveform, consistent peak inspiratory pressure, and variable tidal volume delivery that is dependent on the patient’s lung compliance.8 As tidal volume delivery was carefully controlled in both groups, changes in respiratory outcome may be related to the differences in flow delivery (figs 1 and 2). Infants assigned to VC ventilation in this study may have benefited from better alveolar recruitment, tidal volume delivery, and ventilation–perfusion matching.

Characteristic waveforms (volume, VT: pressure, PAW; and flow, V̊) for time cycled, pressure limited ventilation. Note contour of the flow waveform, which peaks rapidly and then promptly decelerates.
{kind=link}
{kind=link}
Characteristic waveforms for volume controlled ventilation. Note the contour of the flow waveform, which is square. The volume waveform (top) indicates that peak volume delivery occurs simultaneously with peak pressure and is just before flow deceleration.
Although the use of VC in neonates and older children has been described,7 9 there have been no randomised clinical trials to date. There are now proponents of the concept that volume, rather than pressure, is the critical variable in producing lung injury, and it seems that many of the commonly observed pathological changes in RDS could be the result of “volutrauma,” a term which refers to excessive tidal volume delivery in lungs with diminished capacity.10 11 It may be argued, however, that control of tidal volume delivery may be advantageous in newborns with RDS because of the rapidly changing pulmonary compliance, particularly after the administration of exogenous surfactant. Limitation of excessive tidal volume delivery through VC ventilation and sequential reduction in peak inspiratory pressure might improve venous return and cardiac output, thus improving cerebral blood flow.12 13 This may be one possible explanation for the lower frequency of intracranial abnormalities observed among babies who received volume controlled ventilation.
In summary, volume controlled ventilation was both safe and efficacious when used in a group of preterm infants with RDS who weighed more than 1200 g. Compared with infants who received time cycled, pressure limited ventilation, infants treated with volume controlled ventilation achieved successful outcome criteria sooner and had fewer complications.
Acknowledgments
This study was supported by the Research and Development Committee of South Cleveland Hospital.