Article Text

Abstract
AIM To investigate if early changes in concentrations of proinflammatory cytokines in tracheobronchial aspirate fluid (TAF) from preterm infants could be used to detect infants at risk of chronic lung disease (CLD) and help in the selection of patients for early steroid treatment.
METHODS Twenty eight preterm infants less than 34 weeks of gestation (median 26 weeks) were intubated and daily measurements of TAF concentrations of tumour necrosis factor α (TNFα) and the interleukins IL-1β, IL-6, and IL-8 were made, using enzyme immunoassay techniques.
RESULTS Seventeen of the infants developed CLD. The infants who developed CLD had significantly increased concentrations of TNFα, IL-1ß, IL-6 on days 2 and 3. TNFα, IL-6, and IL-8 concentrations were significantly related to gestational age and duration of supplemental oxygen; TNFα, IL-6, and IL-8 concentrations also correlated with length of time on the ventilator.
CONCLUSION These data indicate that tracheobronchial aspirate fluid cytokine concentrations may be used as a predictor of subsequent CLD and may help select a group of preterm infants at high risk of developing CLD for early treatment.
- cytokines
- chronic lung disease
- tracheobronchial aspirate fluid
- mechanical ventilation
Statistics from Altmetric.com
The major advances in neonatal intensive care in recent years have produced an increase in survival of very low birthweight (VLBW) infants. In these immature babies the incidence of chronic lung disease (CLD) is high. CLD increases the length of stay in neonatal intensive care and is also the most common chronic lung disorder in infants.1 Pathophysiological changes in CLD include epithelial and endothelial cell damage, increased permeability, surfactant inactivation, and recruitment/activation of neutrophils and alveolar macrophages.2 3 Proinflammatory cytokines are thought to have an important role in modulating and promoting the initial lung tissue response to injury.4 Expression of individual inflammatory mediators in tracheobronchial aspirate fluid (TAF) from preterm infants has been described.5-8 In a cross sectional study we found increased concentrations of proinflammatory cytokines in infants with CLD, and a decrease after treatment with corticosteroids.9
Our hypothesis is that the early appearance of cytokines in TAF can help to identify patients at high risk of developing CLD, and to select infants for early treatment with intravenous or inhaled corticosteroids. We therefore compared the antigen titres of the proinflammatory cytokines tumour necrosis factor α (TNFα) and the interluekins IL-1β, IL-6, and IL-8 in TAF from intubated infants during the first weeks of life, who subsequently developed CLD, with those in a control group of infants with respiratory distress syndrome (RDS) that resolved without sequelae. We also studied the effect of gestational age, fraction of inspired oxygen (FIO2) and insufflation pressure during mechanical ventilation on the proinflammatory cytokine values.
Methods
This study was conducted from January through December 1994 on mechanically ventilated infants, of 34 weeks gestation or less, admitted to the neonatal intensive care unit at the Karolinska Hospital in Stockholm, Sweden. Tracheobronchial fluid (TAF) was collected daily. A total of 32 patients were sampled. The median (range) gestational age for all infants was 26 (24–33) weeks and the birthweight was 871 (530–2356) g. Infants with perinatal infections (two infants, one withUreaplasma urealyticum and the other with group B Streptococcus), congenital malformations and/or syndromes (n = 2) were excluded from further analysis. Of the remaining 28 infants, 17 developed CLD and these were compared with the remaining 11 patients with uncomplicated RDS. Data on perinatal factors (mode of delivery, rupture of membranes, prenatal steroid treatment) were documented.
Respiratory distress syndrome was diagnosed in infants on the basis of characteristic radiographic findings, respiratory distress, and an increasing FIO2 requirement.10 Infants diagnosed with RDS and an FIO2 > 0.6 received rescue treatment with natural porcine surfactant 200 mg/kg (Curosurf, Serono, Italy), after intubation.
The infants were mechanically ventilated using a Sechrist 100B infant ventilator (Sechrist Corp., Anaheim, California, USA) with initial ventilator settings of FIO2 > 0.6, a rate of 60 breaths per minute, a peak inspiratory pressure (PIP) of < 30 cm H2O, a positive end expiratory pressure (PEEP) of 3–4 cm H2O, and an inspiration:expiration ratio (I:E) of 1:2. If, despite conventional ventilation and surfactant administration, the infant had increasing pCO2, hypoxia and acidosis, high frequency oscillatory ventilation was started using the Sensor Medics 3100A oscillator (Sensor Medics Corp., CA).
Chronic lung disease (CLD) was diagnosed in infants who had been ventilated during the first week of life, had respiratory symptoms, an oxygen requirement and radiological findings at 28 days of age. Air leak was defined as the radiological presence of pulmonary interstitial emphysema and/or pneumothorax. Patent ductus arteriosus (PDA) was diagnosed from clinical signs and confirmed by echocardiography.
The study was approved by the local ethics committee of the Karolinska Hospital.
SAMPLING PROCEDURE
The collection of TAF samples was begun on day 2 of life and was repeated daily, in the same 8 hour period. TAF samples were only collected when endotracheal suctioning was clinically indicated. No additional procedures were needed. Parental consent was obtained for this modified nursing procedure. Before initiating the procedure FIO2 was adjusted to maintain saturation between 92–94% by pulse oximetry. In infants who received surfactant the first sample was taken at least 6 hours after administration.
With the infant supine 0.5 ml of 0.9% sterile saline was instilled endotracheally via a 6.0 French catheter (Vygon, Ecouen, France) and a deep gentle endotracheal suctioning of lung and airway secretions was done by rotating the catheter and applying suction while withdrawing the catheter. To rinse aspirate from the catheter wall, the catheter was flushed with 0.5 ml of sterile saline. All remaining aspirated material was thus flushed into a sterile specimen trap. Tree to five manual breaths were given and the lavage procedure repeated. The total duration of each instillation was less than 40 seconds. The recovery of aspirated fluid ranged between 70–80% of the amount instilled. Samples from the two instillations were pooled. Samples were excluded from further analysis if blood was visible in the aspirate.
Samples were centrifuged at 1200 rpm for 10 minutes. The supernatant fluid was frozen at −70°C until subsequent assay.
CYTOKINE ANALYSIS
The supernatant fluids were used for cytokine determination by enzyme immunoassay (EIA). TNFα, IL-1β, IL-6 and IL-8 kits were obtained from R&D systems (Abingdon, Oxon, UK). The limit of detection was defined as 0.5 pg/ml for TNFα, 3.9 pg/ml for IL-1β, 3.13 pg/ml for IL-6 and 31.3 pg/ml for IL-8.
Cytokine concentrations are expressed as volume concentrations (pg/ml) as no other satisfactory correction factor is currently available. Albumin content, urea, or IgA secretory component have been used as correction units, but their use has been questioned because all are subject to individual variations depending on the disease state, sampling site, and fluid recovered.6 11-13
STATISTICAL ANALYSIS
Intra- and intergroup differences were first tested using analysis of variance. For comparison of clinical variables and differences in cytokine values between groups, the Mann-Whitney U test was used. Differences in frequencies were tested using the χ2 test. Correlations of cytokine concentrations with clinical variables were tested using the Spearman rank correlation coefficient test. For the correlation analysis only the first sample from each patient was used (n=28). A p value of less than 0.05 was considered significant.
Results
There were no differences in regard to sex, method of delivery, prolonged rupture of membranes (PROM) or prenatal steroid use between infants who subsequently developed CLD and those with uncomplicated RDS (table 1). The infants who developed CLD had significantly lower gestational ages and birthweights than infants with RDS (table 1). There were also significant differences between the groups in time spent on a ventilator and duration of supplemental oxygen (table 2). The infants who developed CLD had significantly more air leaks and PDA (table 2). We found no significant correlation between the time of diagnosis or closure of the PDA with concentrations of individual cytokines. No early deaths occurred in either group of infants. Two infants in the CLD group died at 6 months of age from CLD related complications.
Perinatal characteristics of RDS and CLD infants
Ventilatory and clinical characteristics of study population
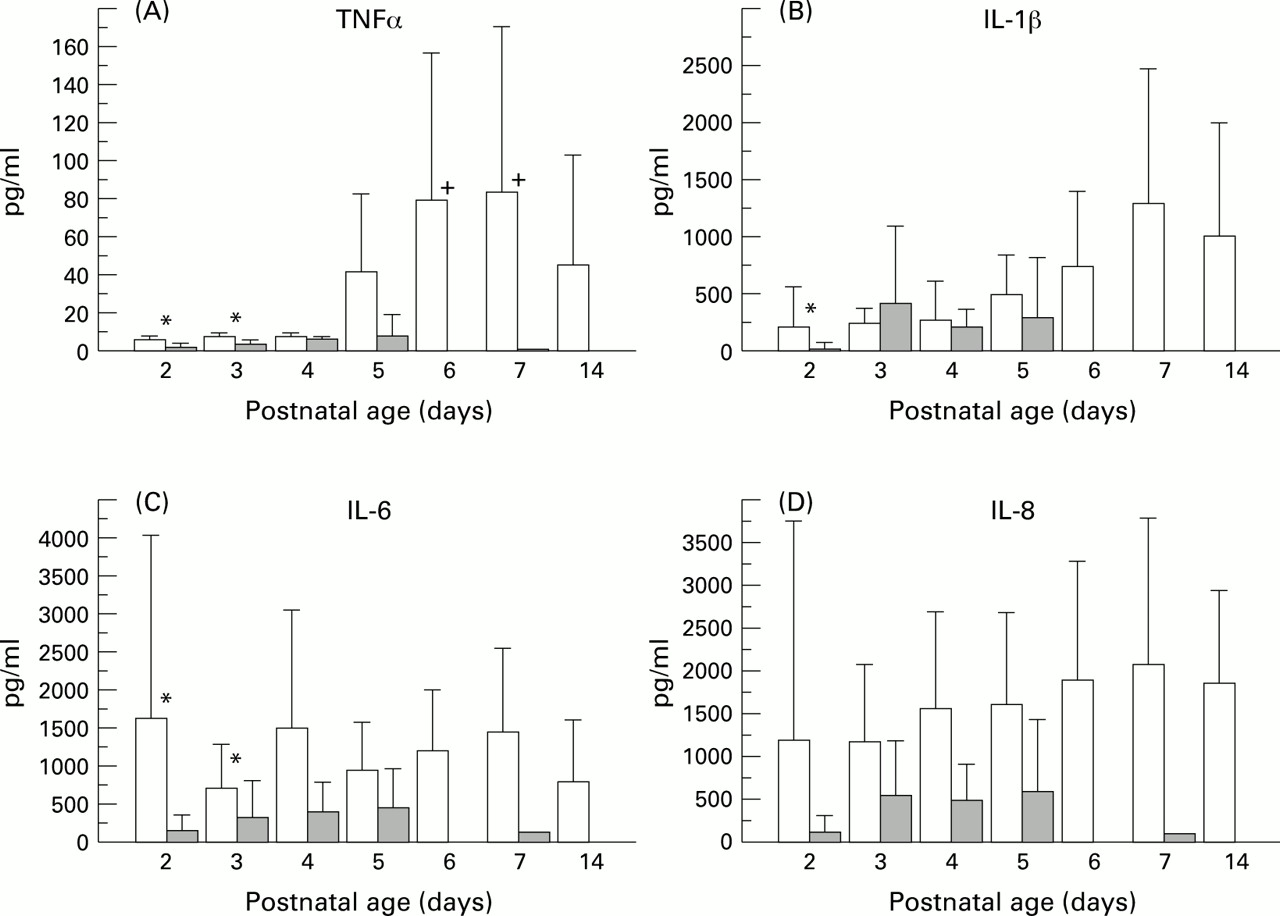
By days 2 (p = 0.0133) and 3 (p = 0.026) neonates who developed CLD had significantly higher TNFα values than the RDS group of infants (fig1A). In CLD infants and RDS control infants median (range) TNFα values on day 2 were 6.5 (3–9) pg/ml and 2.5 (1–4) pg/ml, respectively. On day 2 TNFα concentrations of ⩾ 5 pg/ml were found in six of seven samples in infants who subsequently developed CLD compared with none of the five control infants. In CLD infants TNFα values were significantly higher on days 6 and day 7 compared with day 3 (p = 0.044 and 0.041, respectively). TNFα concentrations were significantly correlated with lower gestational age, birthweight, time spent on a ventilator and duration of supplemental oxygen (table3).

{kind=link}
TAF fluid concentrations of proinflammatory cytokines in infants who subsequently developed CLD and infants with uncomplicated RDS (shaded area). Bars indicate mean values with 95% confidence intervals, on separate days. (A) TNFα concentrations: *denotes p<0.05 on days 2 and 3 between CLD and RDS infants;+ p>0.05 on days 6 and 7 compared with days 2 and 3 for CLD infants. (B) IL-1β antigen titres:*p <0.05 between RDS and CLD infants on day 2. (C) IL 6 concentrations: *p<0.05 on days 2 and 3 between the two groups of infants. (D) IL 8 concentrations
Correlation between cytokine concentrations and clinical variables (Spearman rank correlation showing rs (P value))
IL-1β concentrations were significantly higher only in CLD infants on day 2 (p = 0.046; fig 1B). IL-6 concentrations were significantly higher in CLD infants on days 2 (p = 0.014) and day 3 (p = 0.05) (fig1C) compared with the RDS group. On day 2 median IL-6 concentrations were 1130 (390–3800) pg/ml in CLD infants and 106 (38–350) pg/ml in RDS infants. On day 2 IL-6 concentrations over 350 pg/ml were found in all five samples in CLD infants but in none of the six control infant samples. IL-6 concentrations correlated with lower gestational age, birthweight, time spent on a ventilator and duration of supplemental oxygen (table 3).
Overall, using an analysis of variance, IL-8 concentrations were significantly increased from day 2 to day 7 (p = 0.012) in CLD infants. There was no significant difference in values on separate days between the CLD and the RDS infants (fig 1D). IL-8 concentrations were significantly related to lower gestational age, duration of supplemental oxygen, time spent on a ventilator and maximal PIP (table3).
Discussion
We have shown that proinflammatory cytokines are increased in TAF from as early as day 2 of life in mechanically ventilated preterm infants who subsequently developed CLD. Compared with the control RDS infants their concentrations of TNFα, IL-1β, and IL-6 were significantly higher on days 2 or 3 of life. Our finding of increased cytokines early in the course of CLD supports the hypothesis that they are important mediators in the early inflammatory response in the preterm lung. On day 2 a cutoff limit of 350 pg/ml of IL-6 and 5 pg/ml of TNFα in all cases selected only those infants who subsequently developed CLD. However, our study is to small to define such cutoff limits, but we suggest that further multicentre studies should aim at defining these break points, which could then indicate the potential for early treatment of evolving CLD.
The presence of a major ductal shunt is common in infants weighing less than 1000 g and is related to an increased incidence of CLD.14 PDA can increase pulmonary capillary pressure and promote the formation of oedema, and thus affect the concentrations of cytokines. We found that cytokine concentrations were higher in infants of lower gestational age and correlated with the duration of mechanical ventilation and oxygen exposure. This can reflect an exaggerated tissue response in the more immature lung, and the common presence of PDA and air leak are certainly important in this respect. Recent findings of decreased expression of the down-regulatory cytokine IL-10 in mechanically ventilated preterm infants suggests that an imbalance between proinflammatory and down-regulatory cytokines could be of great importance in the development of CLD.15
Increased concentrations of IL-1β or IL-6 have been associated with chorioamnionitis and bacterial colonisation of the airways at birth in preterm infants.11 16 17 In mechanically ventilated preterm infants increased IL-6 concentrations precede the influx of neutrophils into the airway.18 No previous study has reported the concentrations of all four pro-inflammatory cytokines at the same time (TNFα, IL-1β, IL-6, IL-8) during the first days of life. However, increased concentrations of individual cytokines, such as TNFα,19 IL-1β,20 IL-66and IL-88 have been described in lung secretions of infants who develop CLD.
In this study high IL-8 concentrations were found in the infants who developed CLD compared with the control infants with RDS. In infants with resolving RDS IL-8 concentrations decrease while the infants who develop CLD seem to have a sustained secretion of IL-8 with a continued influx of inflammatory cells into the lung. These cells release toxic products such as elastase which has been implicated in the development of CLD.21 22
Different surfactant preparations down regulate the release of pulmonary cytokines (TNFα, IL-1β, IL-6).23 Natural porcine surfactant decreases the release of TNFα from human monocytes.24 In our study most infants received natural porcine surfactant as rescue treatment for RDS. The first samples were collected at least six hours after surfactant administration. It was not possible to evaluate the down regulatory effect of surfactant in this study as almost all infants received surfactant, but surfactant administration seems to have been insufficient to halt the significant increase in cytokine release.
Corticosteroids are thought to down regulate the release of inflammatory mediators. They are commonly used in the management of infants with developing or established CLD, often after the first week of life.25 The effect of intravenous or inhaled steroids on tracheal aspirate concentrations of inflammatory markers in CLD has been documented.7 9 26 As far as we are aware, no study has examined the effect of steroids administered during the first days of life on proinflammatory cytokine levels, in infants at risk of developing CLD.
In conclusion, we have demonstrated increased concentrations of proinflammatory cytokines in TAF from infants during the first days of life. The values correlate with gestational age and iatrogenic trauma in the form of oxygen exposure and mechanical ventilation. Increased concentrations of proinflammatory cytokines can therefore be the most valuable early indicator of developing CLD and will assist in selecting infants for interventions such as corticosteroid treatment or more selective blockage of components of inflammation.
Acknowledgments
This study was supported by the Swedish Heart Lung Foundation, Sällskapet Barnavård and the Swedish Medical Research Council (Grant B95-16X-08302-08A).