Article Text

Abstract
AIM To evaluate the efficiency and side effects of ibuprofen for the early treatment of patent ductus arteriosus (PDA)and compare it with indomethacin.
METHODS Forty preterm infants with gestational ages of less than 33 weeks, with respiratory distress syndrome (RDS) and echocardiographically confirmed PDA, were randomly assigned at days 2 to 3 of life to receive either intravenous indomethacin 3 × 0.2 mg/kg at 12 hour intervals or intravenous ibuprofen 1 × 10 mg/kg, followed by 5 mg/kg 24 and 48 hours later.
RESULTS PDA closed in 15 of 20 patients from the indomethacin group (75%) and in 16 of 20 (80%) from the ibuprofen group. Seven patients (three indomethacin, four ibuprofen) required a second treatment with indomethacin and in five (three in the indomethacin group and two in the ibuprofen group) the duct was ultimately ligated. Ibuprofen patients had a better urinary output and showed no increase in serum creatinine concentrations compared with the indomethacin group. Ibuprofen was not associated with any other side effect.
CONCLUSIONS Ibuprofen treatment seems to be as efficient as indomethacin in closing PDA on the third day of life in preterm infants with respiratory distress syndrome and seems to have fewer renal side effects.
- patent ductus arteriosus
- respiratory distress syndrome
- ibuprofen
- indomethacin
- Doppler echocardiography
Statistics from Altmetric.com
The incidence of patent ductus arteriosus (PDA) in very low birthweight infants with respiratory distress syndrome (RDS) is about 40% on the third day of life.1 2 Left to right shunting through a PDA causes several undesirable pulmonary, haemodynamic, renal and gastrointestinal effects and increases the risk of intraventricular haemorrhage and bronchopulmonary dysplasia. Therefore, treatment of PDA in preterm neonates with RDS is indicated before important left to right shunting occurs.3 4
Although indomethacin is effective in closing PDA,1-6 its use may be associated with complications such as decreased cerebral, gastrointestinal, and renal blood flow, gastrointestinal perforation or haemorrhage and altered platelet function.7-13 Some side effects such as oliguria, anuria, and transient renal failure are common.14-16 Ibuprofen, another non-steroidal anti-inflammatory drug, can also close the ductus arteriosus in animals, without affecting intestinal haemodynamics.17 18It further enhanced cerebral blood flow autoregulation and exhibited some neuroprotective effect following oxidative stress in the animal model.19-21 When ibuprofen was administered in preterm neonates in early postnatal life, a reduced incidence of PDA was observed.22
As no comparative trials are available, we wanted to examine whether ibuprofen is as efficient as indomethacin in closing PDA, but with fewer side effects. We report the results of a prospective randomised study comparing the effectiveness and the side effects of ibuprofen and indomethacin in the treatment of PDA in preterm infants with RDS.
Methods
The study was conducted in the neonatal intensive care unit of the University Hospital of Antwerp, Belgium. Neonates admitted to the unit were eligible for enrolment if the following criteria were met : (1) gestational age below 33 weeks; (2) RDS treated with mechanical ventilation (intermittent positive pressure ventilation (IPPV) or high frequency oscillatory ventilation (HFOV) with additional oxygen requirements above 30%; (3) postnatal age between 48 and 72 hours. Neonates with major congenital malformations including congenital heart defect, persistent pulmonary hypertension of the newborn, or hydrops fetalis, or in whom either indomethacin or ibuprofen were contraindicated, were excluded. Contraindications for treatment with either drug were: (1) recent (less than 48 hours) intraventricular haemorrhage; (2) clinical bleeding tendency as revealed by haematuria, blood in the gastric aspirate or in the stools, blood in the endotracheal tube aspirate, oozing from venous or capillary puncture sites; (3) thrombocyte count of less than 60 000/mm3; (4) oliguria of less than 1 ml /kg /h during the preceding eight hours; (5) blood urea nitrogen in excess of 14 mmol/l, serum creatinine concentration in excess of 140 μmol/l; (6) hyperbilirubinaemia for which exchange transfusion was required.
Daily clinical care was performed by attending neonatologists who did not take part in the study. All infants were nursed on open tables for the first 36 to 48 hours of life and then transferred to humidified incubators during the remaining study period. Fluid intake was primarily guided by body weight, serum sodium concentrations, and serum osmolarity. A weight loss of 5-10% was allowed for during the first postnatal days. Most patients received one or more transfusions of packed red blood cells or plasma. For RDS treatment, surfactant replacement therapy (Alvofact, Boehringer or Survanta, Abbott) was applied in doses of 100 mg/kg according to a strict protocol.
Informed consent was obtained from the parents and the study was approved by the medical ethics committee of the hospital.
In all patients eligible for enrolment in the study, a complete echocardiographic–Doppler evaluation was performed to visualise the PDA and the shunting through it (Hewlett Packard Sonos 1500 with 7.5 MHz transducer; examinations were recorded on videotape and printouts). The internal ductal diameter was registered as the average of four measurements in colour Doppler mode with the same pre- and post processing settings.23 The maximal velocity of the left to right shunt through the ductus was recorded by pulsed or continuous Doppler and the ratio of left atrial to aortic root diameter measured in M-mode was registered. Shunting through the PDA was arbitrarily graded as follows: (1) minor shunting if a small jet was detectable at the pulmonary end of the ductus with colour flow and continuous or pulsed Doppler interrogation, with the proviso that no disturbed flow was detectable at the level of the pulmonary valves and diastolic forward flow in the pulmonary trunk was absent, and if the left atrial to aortic ratio was less than 1.2; (2) moderate shunting if a disturbed diastolic flow was easily detectable at all sites of the pulmonary trunk, a diastolic back flow was present in the aorta immediately beneath the PDA and a forward flow above the PDA; (3) severe shunting if a diastolic back flow was detectable in the aorta and if dilatation of the left atrium was present and expressed as a left atrium to aortic root ratio above 1.6. The maximal velocity of the ductal left to right shunt was noted in order to obtain an estimate of the systemic to pulmonary arterial pressure difference. When there was minor shunting or when the patient showed substantial improvement of his respiratory status during the second day of life, a delay of 24 hours was allowed to see if the patient could be weaned off the respirator. If not, the echocardiographic Doppler ultrasound scan was repeated and if the patient still had PDA s/he was entered.
Enrolled patients were randomised using the sealed envelope technique to receive either intravenous indomethacin (Indocid) three times 0.2 mg/kg at 12 hourly intervals, or intravenous ibuprofen (Ibuprofen-lysine) 10 mg/kg followed by 5 mg/kg after 24 and 48 hours. Both drugs were continuously infused over 15 minutes. The doses and intervals for ibuprofen were chosen in accordance with the recommendations in infants and neonates which are based on preliminary pharmacodynamic data and on the in vitro comparison of the cyclo-oxygenase type 1 isoenzyme inhibitory potencies of different NSAIDs.24-26
A second echocardiographic Doppler ultrasound scan was performed in all patients after the last dose of the randomised treatment regimen and at the age of 7 days to evaluate the ductus as defined earlier. When PDA was still present and the patient was still on mechanical ventilation, s/he was treated with indomethacin (3 × 0.2 mg/kg at 12 hourly intervals). Another echocardiographic-Doppler scan was performed either after the second treatment to assess its efficiency, or after one week in the patients who received only one treatment, in order to detect a possible late reopening of the ductus.
Clinical and biological data were prospectively reported on data sheets designed for this study. The following parameters were registered.
(1) Clinical parameters: date and time of birth, gestational age, sex, antenatal corticosteroid or indomethacin administration, findings on physical examination at the time of echocardiography, grade of RDS, ventilator settings, time, type, dose and number of surfactant administrations, daily crystalloid and colloid fluid intake, urinary output and daily body weight. Bleeding tendency was evaluated using the same criteria as those for contraindications to treatment. Intravenous fluid intake was expressed in ml/kg of birthweight rather than actual daily weight. Similarly, urine output was expressed in ml/kg of birthweight /hour.
(2) Laboratory parameters: serum creatinine, serum electrolytes, serum osmolarity, glycaemia, haematocrit and haemoglobin concentration, thrombocytes, C reactive protein, white cell count and differentiation and cultures when there was suspicion of infection.
(3) Cranial ultrasound scans: these were performed on all infants on days 1, 2, and 3 and weekly thereafter; if clinically relevant additional ultrasound scans were also performed. Haemorrhages were graded as mild, moderate, or severe according to Shankaran.27 28
(4) Outcome: in the surviving patients this was defined on the basis of their respiratory support (mean airway pressure, inspired oxygen concentration) on postnatal days 7 and 14, the total number of days on mechanical ventilation and on additional oxygen, the numbers of patients still on additional oxygen on day 28, the time needed to regain birthweight and the time interval between birth and full enteral feeding.
Statistical hypothesis analysis involved the use of χ2test on contingency tables, the standard t test for independent samples, and paired comparisons test for repeated measurements. For evaluation of non-parametric data the Mann-Whitney U test was used. As our first aim was to detect a clinical difference in the efficiency of ibuprofen compared with indomethacin of at least 30% with P=0.05 and a power of 80%, ibuprofen otherwise not offering any advantage over spontaneous closure, 20 patients were included in each group. Computer software used was CSS-Statistica.
Results
Eighty five patients were eligible for entry in the study and underwent an echocardiographic-Doppler ultrasound evaluation between the second and third day of life. Forty five were excluded because of an already closed duct in 40 (47%), PDA with minor shunting and respiratory improvement in two, severe right to left shunting through the ductus due to pulmonary hypertension in two, and sepsis with bleeding tendency in one patient. The remaining 40 patients had PDA and were randomly allocated to receive either indomethacin or ibuprofen.
The characteristics of the patients before treatment are shown in table1: there were no significant differences between either group. The respiratory status of the patients is expressed by their need for ventilatory support (average mean airway pressure and mean percentage of supplemental oxygen at 24, 48, and 72 hours of life) and the number of patients that received exogenous surfactant treatment. There were no patients with minor shunting or a ductal diameter of less than 1.5 mm at entry.
Patient characteristics before treatment1-150
INCIDENCE OF PDA AND TREATMENT
There was no significant difference in efficiency of either treatment, the closing rate being 75% and 80% in the indomethacin and ibuprofen groups, respectively. In nine patients the ductus arteriosus remained open after the first treatment (five in the indomethacin group and four in the ibuprofen group). Two of these, both from the indomethacin group, received no further treatment for PDA because of a substantial improvement in their respiratory status to spontaneous ventilation. Seven (three in the indomethacin group, four in the ibuprofen group) received a second treatment with indomethacin, on average on the 8.3 (2.2) (± 1 SD) day of life. The efficiency of this backup treatment was 29%: closure of the PDA occurred in only two of the seven patients (one in each group). These seven patients had the lowest birthweights of the whole group (birthweight 940 (200) g, gestational age 27.3 (2.3) weeks). Ultimately, the duct was ligated in five patients, on average on day 11 (three from the indomethacin group and two from the ibuprofen group). In one patient the duct reopened after initial closure with ibuprofen treatment and failure of a second dose of indomethacin. In the nine patients with persistent ductus after the first treatment the maximal velocity of the ductal left to right shunt increased from 1.41 to 1.93 m/second (P=0.03) and the left atrium to aortic root ratio decreased from 1.56 to 1.37 (P=0.02) without significant differences between either group of patients.
RENAL FUNCTION
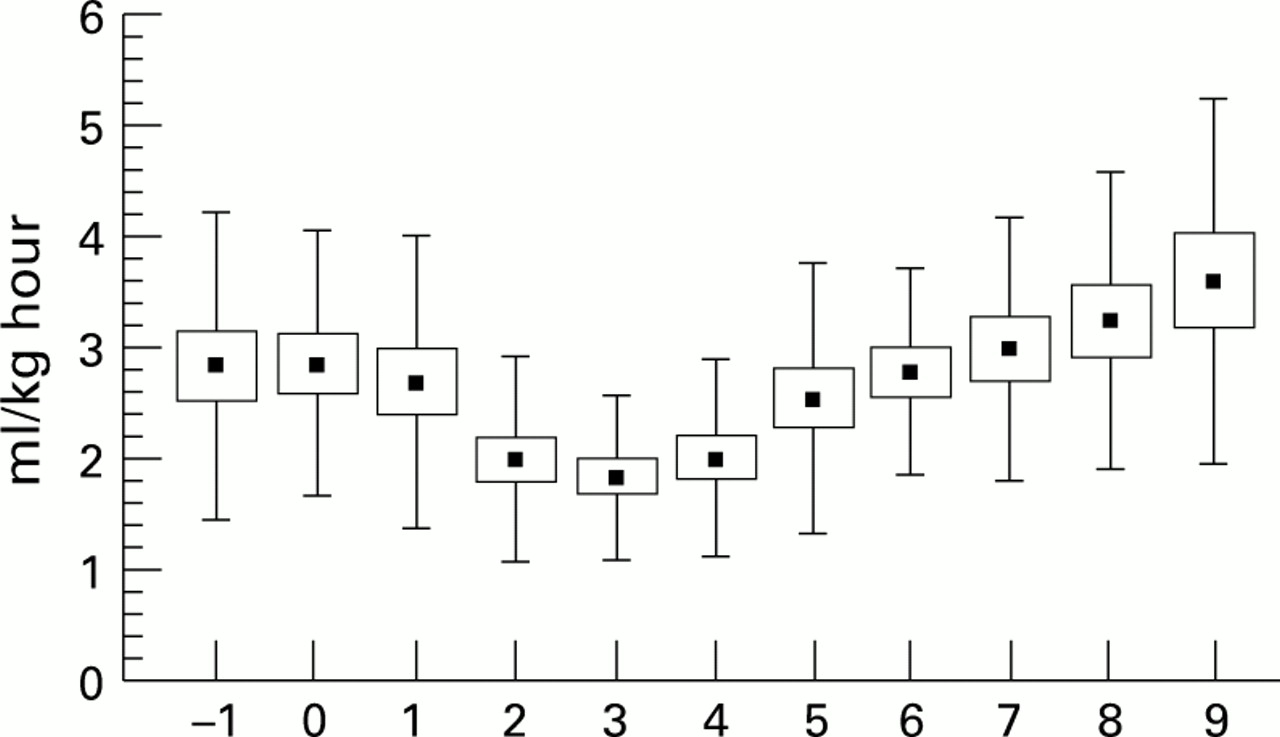
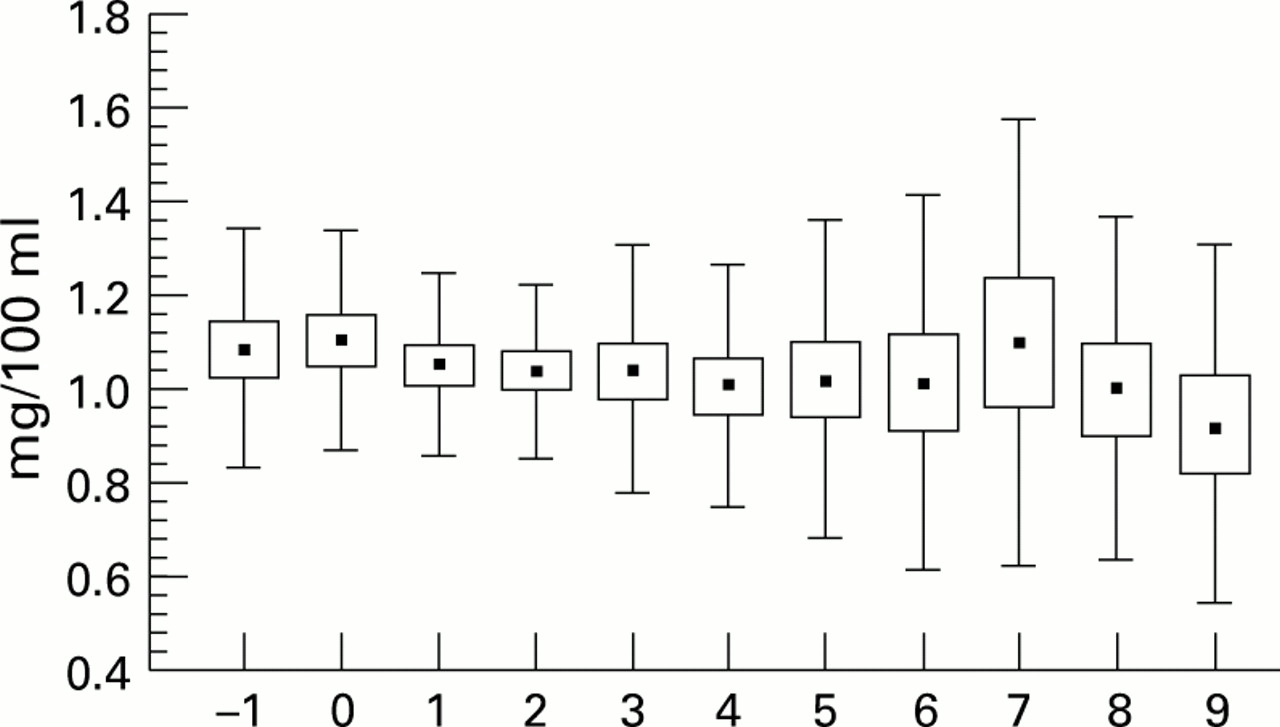
In the indomethacin group urine output decreased significantly on the second day after start of treatment to a minimal mean value of 1.9 ml/kg birthweight/hour (P=0.001) and increased again afterwards in all infants within seven days. But there was no significant decrease in urine output after start of treatment in the ibuprofen group (fig 1). Urine output was significantly less in the indomethacin group than in the ibuprofen group on days 2, 3, and 4 after treatment (P=0.002). In the ibuprofen group urine production varied from 3.0 ml/kg birthweight/hour on the day before treatment to 3.3 ml/kg birthweight/hour on day 7 after treatment. As to the number of patients with oliguria (urine production less than 1 ml /kg/hour), 40% developed oliguria in the indomethacin group compared with 5% in the ibuprofen group (P=0.02). The increase in serum creatinine was larger after indomethacin treatment, reaching a maximum mean value of 1.25 mg/100 ml on the third day after treatment, whereas no significant difference was seen in the ibuprofen group (P=0.07) (fig 2). Diuretics were not used in either group during the first week of life. Daily fluid intake did not differ significantly between both patient groups. The starting rate of crystalloid intake depended on birthweight: patients with birthweights ⩽ 1000 g were given 100-110 ml/kg/day, patients with birthweights >1001 g received 60-75 ml/kg/day. Crystalloid fluid intake was increased day by day for both patient groups to about 120 ml/kg/day by day 10 of life. There was no difference between the groups for the use of colloids or blood products. Daily weight evolution was similar in both treatment groups, with an average weight loss of 7%.
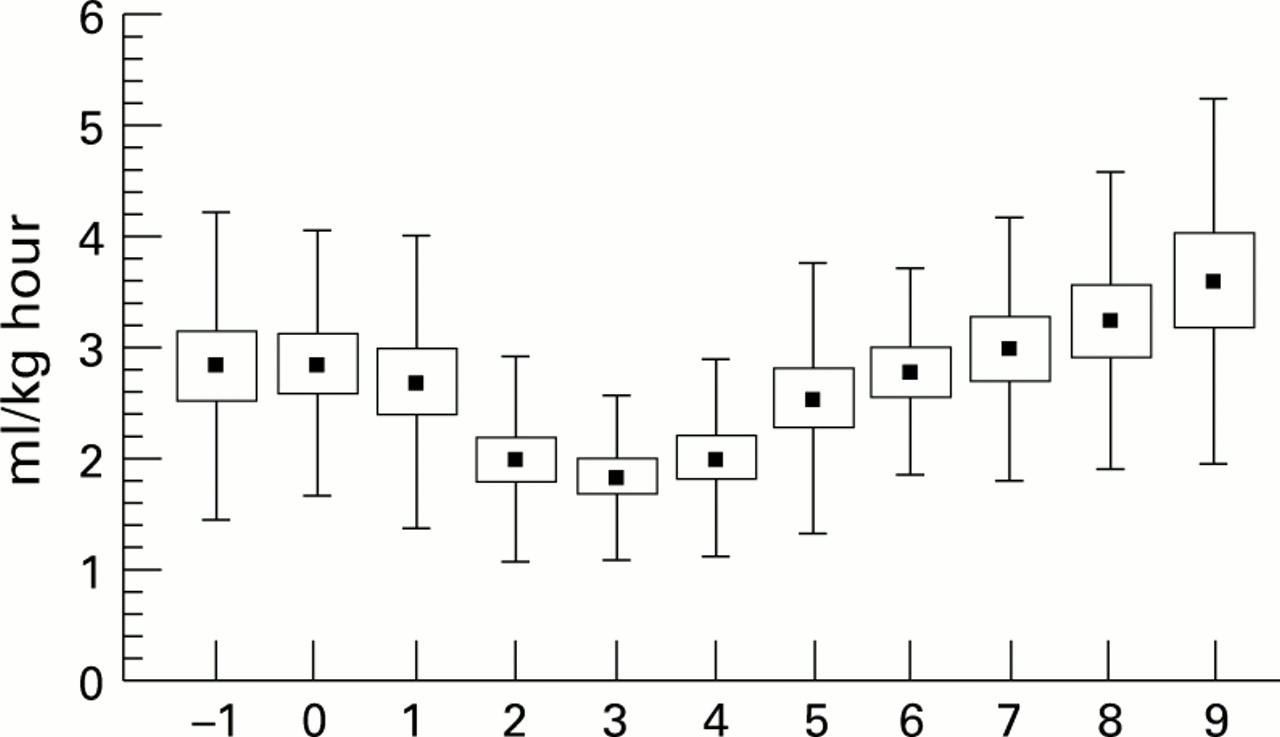

Urine production in the indomethacin group (upper panel) and the ibuprofen group (lower panel) over 11 days. Day 0 = start of treatment; means ± 1 SE, ± 1 SD. There was a significant difference between the two groups on days 2, 3, and 4 (P=0.002).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Serum creatinine concentration in the indomethacin group (upper panel) and the ibuprofen group (lower panel) over 11 days. Day 0 = start of treatment; means ± 1 SE ± 1 SD. Maximal difference between the two groups occurred on day 3 (P= 0.07).
RESPIRATORY FUNCTION
The incidence and severity of RDS were not significantly different between the two treatment groups. The average mean airway pressure and mean fraction of inspired oxygen concentration following PDA treatment was not different in the groups, although a trend toward higher oxygen need was observed in the indomethacin group. Data are given for days 7 and 14 of life (table 2). The number of days on ventilation, the number of days on additional oxygen, and the number of patients that still had additional oxygen requirements on the 28th postnatal day did not significantly differ between the two groups. At the age of 28 days, three patients were still being ventilated and nine still needed supplemental oxygen in the indomethacin group compared with four and 13, respectively, in the ibuprofen group. There were no differences in air leak syndromes or pulmonary haemorrhages between the groups.
Respiratory and cardiovascular evaluation2-150
OTHER VARIABLES
No difference in bleeding tendency, as defined earlier, was observed. Occult blood in the stools was detected in four patients (two in each group). Microscopic haematuria was frequently noted during the first two to three days of life, but its incidence was equal in both groups. No difference was observed in platelet count, bilirubinaemia, or hepatic enzyme values.
No significant differences in sepsis or other infectious complications could be demonstrated (table 3). Bowel perforation was observed in one patient in each group: both had been exposed prenatally to indomethacin. Two other patients had necrotising enterocolitis. There were four neonatal deaths: three in the indomethacin group (major intraventricular haemorrhage, overwhelming sepsis, and intractable respiratory deterioration) and one in the ibuprofen group (intractable respiratory deterioration).
Other outcome variables3-150
No adverse effect of ibuprofen on feeding tolerance was observed; the time to regain birthweight was in fact somewhat shorter in this group, but this difference was not significant. The time interval needed to be exclusively enterally fed, was comparable in both groups. In the indomethacin group, one patient developed retinopathy of prematurity.
Discussion
For many years indomethacin has been the drug of choice in the treatment of PDA but renal and cerebral haemodynamic side effects have been frequently reported.1-16 Strategies to minimise the renal side effects such as its association with furosemide, or with low doses of dopamine or the use of prolonged low doses, have not all been equally successful.29-32 Other NSAIDs have also been tried but either had other side effects, as is the case with mefenamic acid,33 34 or were less efficient in closing the duct, as was shown for aspirin.35
In animals ibuprofen closed the duct more or less as well as indomethacin and had fewer cerebral and gastrointestinal side effects.17-19 Some early studies are available in the human neonate from which it was concluded that ibuprofen is efficient at closing the duct and has less cerebral and renal side effects.36-40 More recently its prophylactic use within the first few hours after birth has been advocated22: the prophylactic treatment of PDA is, however, not yet uniformly accepted.41 The present study is the first which compares the two drugs in a prospective randomised way. We found that ibuprofen as an early treatment of PDA in preterm neonates with RDS, is as efficient as indomethacin and, unlike indomethacin, is not associated with significant side effects, particularly decreased urinary output or increased serum creatinine. The dose of ibuprofen was based on its in vivo inhibitory effect on cyclo-oxygenase 1.26 Although more pharmacokinetic data on ibuprofen are needed in neonates, it has been suggested that it should be administered at longer time intervals than indomethacin24: therefore, dosing intervals of 24 hours were chosen.
The ductal closure rate after either treatment was within the range reported, but lower than we reported earlier.35 This may be due to an increased prenatal use of indomethacin in the patients from the present study which was comparable in both groups (table 1).
The capacity to close definitively the duct and arrest all flow through the ductal lumen is the main effect of successful PDA treatment. However, reduction of shunting through the duct will also result in a substantial decrease in the pulmonary blood flow and, through this, may lead to a reduction of the lung water content and to an improvement in RDS. We therefore compared the degree of ductal shunt in both groups of treated neonates. Not only was there no difference in closure rate, but the degree of shunting through the duct was also identical in the nine patients from both groups with a still open duct. Indomethacin may increase pulmonary vascular resistance, but as we observed a decrease in the pulmonary artery pressure vs systemic pressure, with no differences in either groups, this could be excluded, at least in our patients whose duct remained open. Cardiovascular evaluation of patients who did not need a second treatment because of substantially improved respiratory status, was no different between the groups. As temporary closure and reopening of the duct has been reported as being associated with severe infection and sepsis,42 we investigated this in our patients: the incidence of confirmed or probable sepsis was comparable in both groups; reopening in two patients from the ibuprofen group was not associated with infection (table 3).
We cannot explain the difference in renal side effects between the two drugs. One possibility is that both drugs inhibit the cyclo-oxygenase enzyme system in the neonatal kidney to a different extent. In vitro, in the doses used in this study, both drugs inhibit the cyclo-oxygenase system to the same extent.26 Very little, however, is known about the expression of isozymes in neonatal renal tissue. Another possibility is that, due to different pharmacokinetic characteristics in the neonate, serum indomethacin concentrations remained high enough to influence both the ductus and the renal function, whereas those of ibuprofen were sufficiently high to close the duct but lacked the potential to impair renal function. Finally, the possibility of non-prostaglandin effects should also be considered.
Other side effects of ibuprofen treatment, such as increased bleeding tendency, need for backup treatment, or feeding intolerance, were not observed. There was, on the other hand, a trend towards earlier regain of birthweight and full oral feeding in the ibuprofen group. Our study was not designed to measure cerebral haemodynamics: less impairment of the latter compared with indomethacin, has been reported.38-40
From these preliminary data we conclude that ibuprofen can be used efficiently in premature neonates with RDS for the closure of the ductus arteriosus on the third day of life, with the advantage that it causes fewer side effects than indomethacin. Our findings need to be confirmed by studying a larger number of patients. Other possible side effects should also be investigated.