Article Text

Abstract
Objective To compare outcomes at hospital discharge for preterm infants born before 29 weeks of gestation who had at least one episode of isolated hypotension during their first 72 hours of life for which they did or did not receive antihypotensive treatment.
Design Etude Epidémiologique sur les Petits Ages Gestationnels 2 (EPIPAGE 2) French national prospective population-based cohort study in 2011.
Setting 60 neonatal intensive care units.
Patients All infants with a minimum mean arterial blood pressure less than gestational age (in weeks) (minMAP<GA) within 72 hours of birth. Infants whose reason for receiving antihypotensive treatments was isolated hypotension only were compared with untreated hypotensive infants by propensity score matching.
Treatments Fluid bolus and/or inotropes and/or corticosteroids.
Main outcomes and measures The primary outcome was survival at hospital discharge without major morbidity, defined as any of necrotising enterocolitis, severe cerebral abnormalities, severe bronchopulmonary dysplasia or severe retinopathy of prematurity.
Results Among the 1532 infants with available data, 662 had a minMAP<GA; 206 were treated for unknown or other reasons than isolated hypotension, 131 were treated for isolated hypotension only and 325 were untreated; 119 infants from each of these last two groups were matched. Treated infants had a significantly higher survival rate without major morbidity (61.3% vs 48.7%; OR, 1.67, 95% CI 1.00 to 2.78, p=0.049) and a lower rate of severe cerebral abnormalities (10.1% vs 26.5%, p=0.002).
Conclusions In this population, antihypotensive treatment was associated with improved short-term outcomes. Therapeutic abstention should be cautiously considered for early isolated hypotension in extremely premature infants.
- Neonatology
- Circulatory
- Epidemiology
- Intensive Care
Statistics from Altmetric.com
What is already known on this topic?
Low blood pressure values are frequent in the first 3 days after birth in extremely premature infants.
Both hypotension and antihypotensive treatments have been identified as risk factors for poor outcome.
Equipoise currently exists between abstention and antihypotensive treatments for isolated hypotension, that is, without other clinical or paraclinical signs suggesting poor perfusion.
What this study adds?
In this prospective national cohort study, antihypotensive treatment was associated with improved outcomes at hospital discharge when compared with abstention for infants with isolated hypotension.
These results challenge the currently popular ‘permissive hypotension’ strategy.
Long-term outcomes and results from ongoing randomised trials are needed to help clinical decision making in extremely premature infants with early isolated hypotension.
Introduction
In extremely low gestational age neonates (ELGANs), many issues remain unresolved concerning the measurement, interpretation and management of blood pressure (BP).1 Whichever definition is used, around 50% of ELGANs experience perceived low BP, usually referred to as hypotension, in their first postnatal days.2 ,3 Moreover, around half of all ELGANs receive antihypotensive treatments, even in the absence of low BP values.4 Randomised controlled trials conducted decades ago have not found volume expansion to be either beneficial or harmful,5 and we lack long-term data for most drugs used in this context.6–8 More recent observational studies have suggested a potentially harmful effect of antihypotensive therapies on long-term outcome.4 ,9
The concept of permissive hypotension,10 defined as therapeutic abstention and careful observation, has gained popularity among neonatologists11 and justifies the completion of the ongoing large, multicentre randomised controlled trial comparing dopamine with placebo in ELGANs with early hypotension (Management of Hypotension In the Preterm Extremely Low Gestational Age Newborn trial).12 Its design includes a saline bolus in both treatment arms and it is not assessing the impact of the complete therapeutic abstention that occurs in daily practice.2
Etude Epidémiologique sur les Petits Ages Gestationnels 2 (EPIPAGE 2),13 a national population-based prospective cohort study, provided a unique opportunity to evaluate the association between strategies used in daily practice—such as management of early isolated hypotension and in-hospital outcomes among preterm infants. Because arterial BP alone is a poor surrogate for systemic blood flow,14 we hypothesised that any antihypotensive treatment in ELGANs based only on a low BP value (ie, without any other sign of haemodynamic compromise) would challenge the limited adaptive capacities of the neonatal circulation and thus be associated with worse outcomes than therapeutic abstention.15 Our objective was to compare survival without major morbidity at discharge in preterm infants born before 29 weeks of gestational age (GA) who had at least one episode of isolated hypotension during the first 72 hours after birth and did or did not receive antihypotensive treatment for it.
Methods
Study cohort
EPIPAGE-2 is a birth cohort scheduled to follow preterm children to the age of 12 years, whose details were previously published.13 ,16 Recruitment took place at birth in all maternity units in France from March 2011 through December 2011, during an 8-month period for births occurring at 24–26 weeks and a 6-month period for births occurring at 27–28 weeks. In the present study, eligible patients were neonates born between 24 and 28 weeks with at least one episode of hypotension before day 3 of life, defined as a minimum mean arterial blood pressure value (minMAP) lower than GA (in weeks) (minMAP<GA). Exclusion criteria were: infants born at 22 or 23 weeks who were usually provided palliative care and rarely survived in France in 2011,17 congenital malformations, treatment limitation or withdrawal within 72 hours of birth and missing data for minMAP or antihypotensive treatment. We focused our study on infants who were either untreated or treated only because of a low BP value. Infants for whom the decision for antihypotensive treatment was motivated by hypotension associated with additional clinical signs, echocardiographic findings or abnormal laboratory results suggesting haemodynamic compromise were used for sensitivity analysis.
Treatments
Infants in the treated group received any of these antihypotensive treatments: fluid bolus, inotropes or corticosteroids. The study questionnaire collected detailed information about infants' haemodynamic management the first 3 days of life, including the reason for treatment according to the attending physician (isolated low BP value; low BP value associated with other clinical signs and/or echocardiographic findings and/or laboratory results suggesting haemodynamic compromise). All data were collected prospectively during hospitalisation from medical records and obstetric and neonatal staff and verified by the local paediatric study coordinator.13 The frequency of BP measurements was not collected.
Outcomes
The primary outcome was survival without any of the following severe morbidities at discharge: severe bronchopulmonary dysplasia, defined as administration of oxygen for at least 28 days plus need for 30% or more oxygen and/or mechanical ventilatory support or continuous positive airway pressure at 36 weeks' postmenstrual age; stage II and III necrotising enterocolitis according to Bell's staging; severe retinopathy of prematurity (ROP), defined as stage 3 or more and/or laser treatment; any of the following severe cerebral abnormalities on cranial ultrasonography: intraventricular haemorrhage with ventricular dilatation (grade III IVH); intraparenchymal haemorrhage (IPH), defined as a large unilateral parenchymal hyperdensity or a large unilateral porencephalic cyst or cystic periventricular leukomalacia (PVL), defined as periventricular white matter echolucencies. Ultrasound abnormalities were based on the most severe lesion observed among all sequentially performed exams until discharge or death.
Secondary outcomes included death before hospital discharge, causes of death and the severe morbidities listed above.
Statistical analysis
Primary analysis
We sought to control for the non-random assignment of patients to the treated and untreated groups with a propensity score approach. The propensity score was defined as the infant’s probability of exposure to antihypotensive treatment based on his/her individual observed covariates and estimated with a logistic regression model. In this model, antihypotensive treatment was the dependent variable and was studied in relation to the baseline characteristics that were clinically or statistically associated with the exposure and/or the outcome (see selection of covariates in the online supplement). Management of missing data is detailed in the online supplement. We used a 1:1 matching algorithm without replacement to match treated and untreated newborns for GA and the propensity score with a calliper width measuring 0.2 of the SD of the score's logit.18 Matching was performed with the %GMATCH SAS macro (Mayo Clinic, Rochester, Minnesota, USA). Matching balance was assessed by the standardised difference, that is, the difference in means or proportions divided by the SE. A standardised difference of less than 10% is considered to indicate an acceptable imbalance between groups.19 Outcome analysis after matching for the propensity score used logistic regression fit by generalised estimating equations to account for paired data20 and assessed the average treatment effect in the treated group (ATT).21 For analyses performed on the overall cohort, we used weighted percentages and GA adjustments in the multivariable analysis to take into account the differences in the recruitment times for the infants born at 24–26 weeks of gestation or at 27 and 28 weeks of gestation. All tests were two sided. p Values <0.05 were considered significant. All analyses were performed with SAS software (V.9.4).
supplement data
Sensitivity analyses
Six sensitivity analyses were performed (details in the online supplement): (1) model (1): logistic regression model after multiple adjustments; (2) model (2): generalised estimating equation logistic regression model weighted by the propensity score;21 (3) multiple imputation for missing data for variables included in the propensity score;22 (4) multiple imputation for missing antihypotensive treatment's indications; (5) analysis of the group of infants who received antihypotensive treatment for any other reason than isolated hypotension (symptomatic treated group) and (6) negative control.23
Subgroup analysis
The primary outcome was studied with a propensity score matching approach in the subgroup of infants with minMAP≤GA-5 to assess the effect of exposure on outcomes according to the severity of hypotension.
Results
Population
During the study period, 1633 ELGANs were admitted to the neonatal intensive care unit (NICU). Among the 662 infants with a min mean arterial blood pressure (MAP)<GA, 206 were treated for unknown or other reasons than hypotension only, 131 received some hypotensive treatment for isolated hypotension only (treated group) and 325 received no antihypotensive treatment (untreated group) (figure 1). These infants were hospitalised in 60 NICUs, in which the percentage of antihypotensive treatment varied from 0% to 100%. This percentage was not significantly related to the volume of patients per NICU (Pearson correlation r=0.010, p=0.94; online supplementary figure S1). Figure 2 and online supplementary table S1 present the differences between treated and untreated infants. The antihypotensive treatments used before and after day 3 and the management of patent ductus arteriosus (PDA) in both groups are summarised in online supplementary table S2.
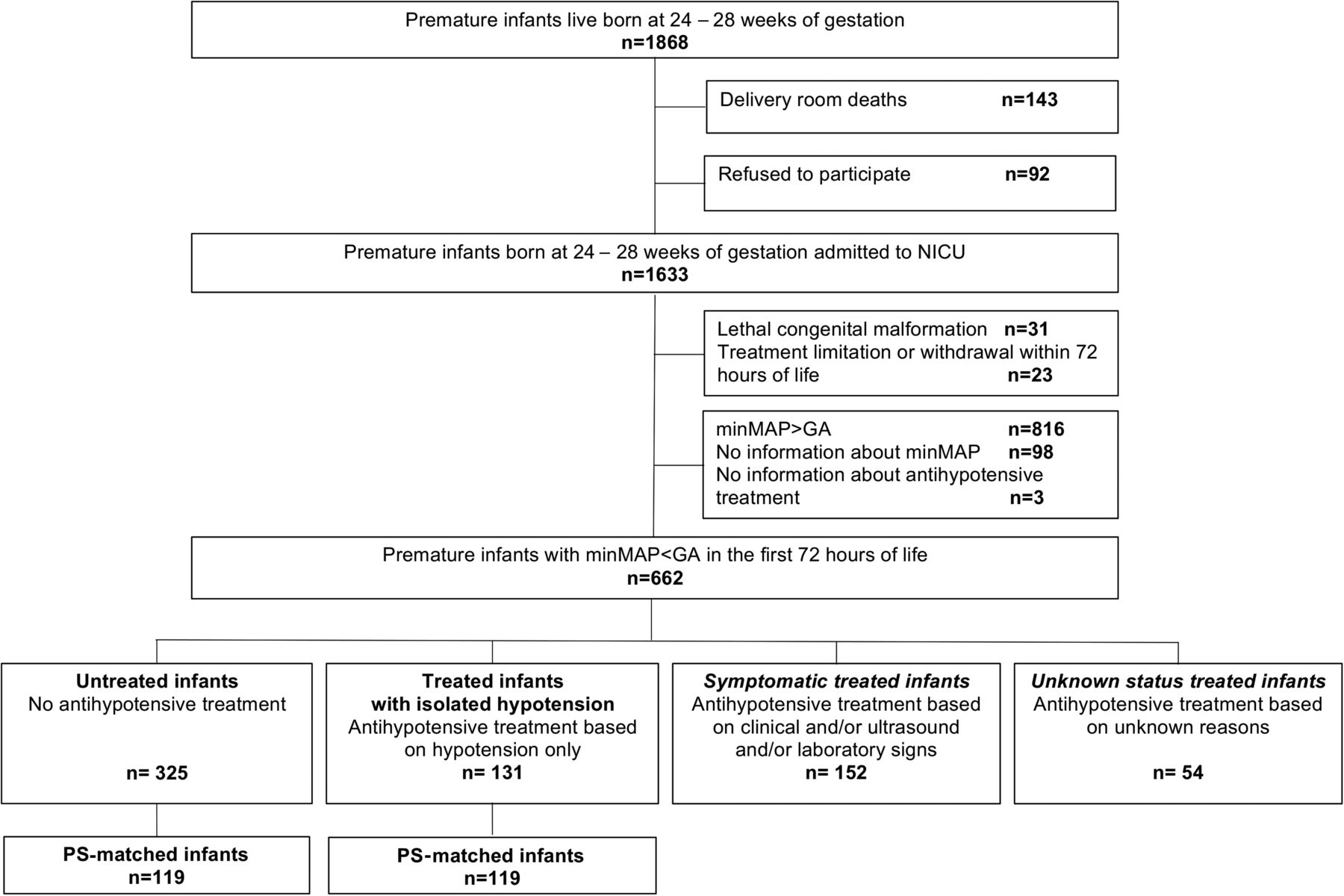
Population flow chart. GA, gestational age; minMAP, minimum mean arterial pressure; NICU, neonatal intensive care unit; PS, propensity score.
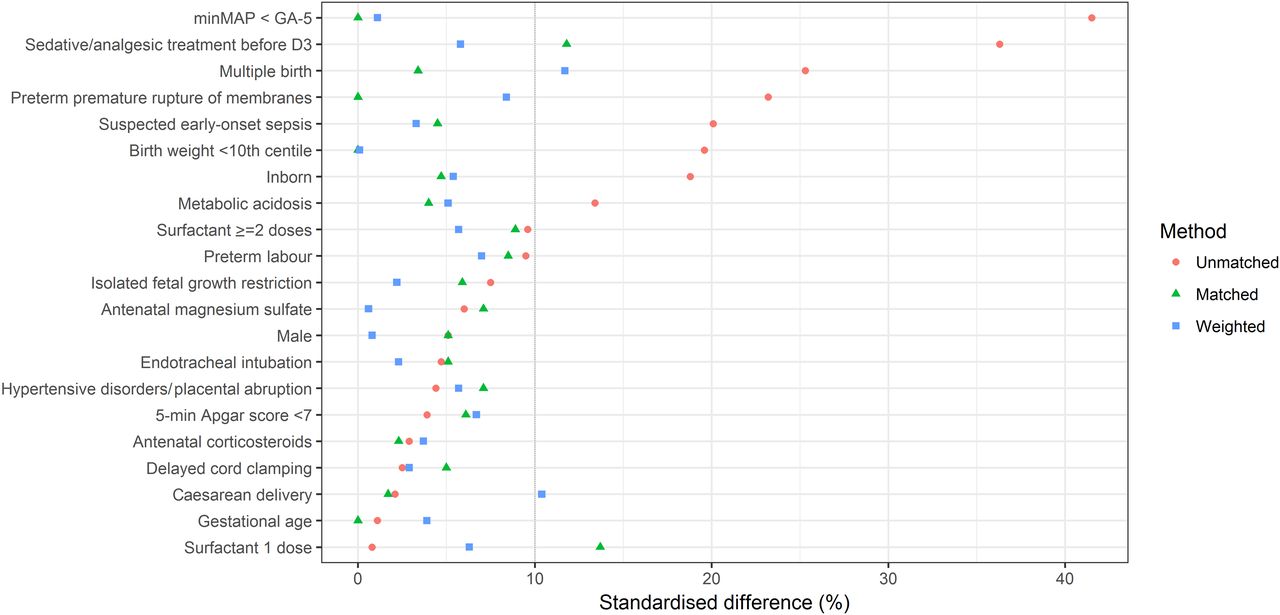
Standardised differences for covariates used in the propensity score. Each point illustrates the standardised difference for each variable in the overall cohort (red circles), the propensity score-matched cohort (green triangles) and the propensity score weighted model (model (2)) (blue squares). The vertical line at 10% illustrates the standard cut-off for acceptable imbalance between groups. D3, day 3 of life; GA, gestational age; minMAP, minimal mean arterial blood pressure.
Propensity score-matched cohort analysis
Among the 456 ELGANs with propensity scores ranging from 0.03 to 0.95 (see online supplementary figure S2), 238 could be matched, with 119 in each group, treated and untreated, who were rather well balanced for all recorded baseline variables (see online supplementary table S1 and figure 2).
In the matched cohort, survival at discharge without severe morbidity was significantly higher in the treated compared with the untreated group (OR, 1.67; 95% CI 1.00 to 2.78, p=0.049); the treated group had significantly lower rates of severe cerebral abnormalities (10.1% vs 26.5%, p=0.002) and of grade III IVH or IPH (10.1% vs 22.2%, p=0.015) (table 1). Other secondary outcomes were similar between groups. Neurological complications accounted for 63% and 25% of the causes of death in the untreated and treated groups, respectively (see online supplementary table S3).
Survival and severe neonatal morbidity at discharge according to antihypotensive treatment
Sensitivity analyses
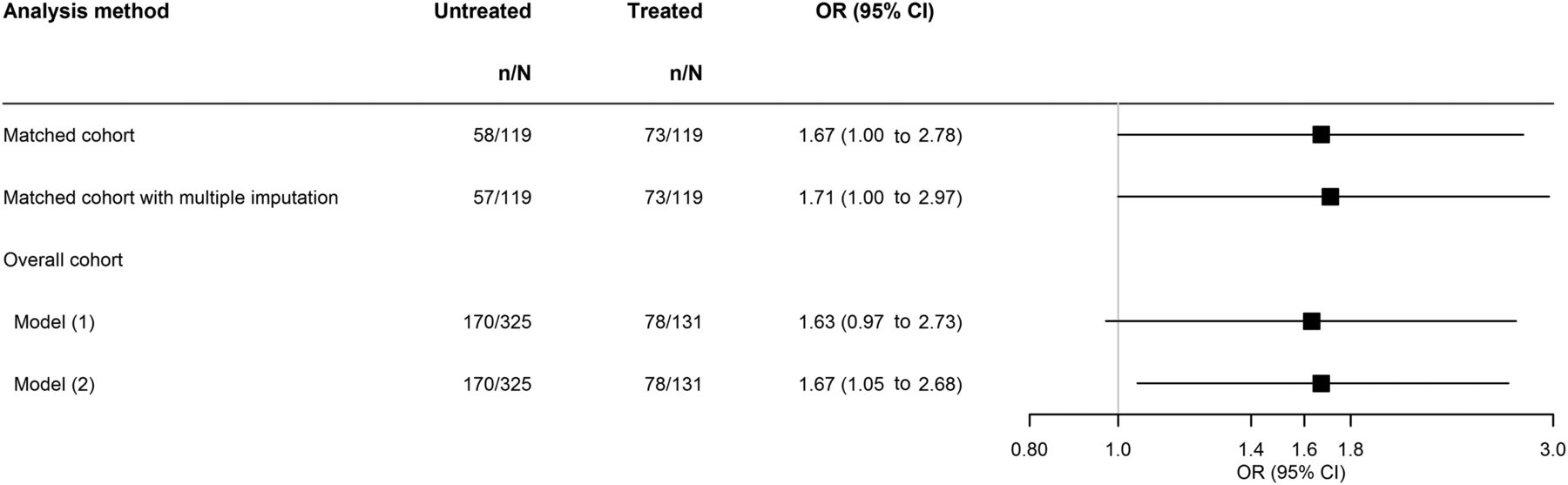
Logistic regression analysis showed no statistically significant differences between the treated and untreated groups in model (1) (figure 3). Model (2) resulted in a good balance of the covariates included in the propensity score (figure 2) and provided significant results consistent with the primary analysis (OR, 1.67; 95% CI 1.05 to 2.68) (figure 3).

{kind=link}
{kind=link}
{kind=link}
Multivariable analysis for survival without major morbidity at hospital discharge. Model (1) adjusted for gestational age (GA), cause of preterm birth, multiple births, birth weight centile, sex, surfactant therapy, suspected early-onset sepsis, analgesic or sedatives before day 3, minMAP<GA-5, metabolic acidosis (defined as a base excess<−7 in the first 12 hours of life), inborn and volume patient of neonatal unit. Model: (2): generalised estimating equation logistic regression model weighted by the propensity score. Denominators vary according to the number of missing data items for adjustment variables.
After multiple imputation for missing data in the propensity score, treated infants had a significantly better outcome than untreated infants (OR, 1.71, 95% CI 1.00 to 2.97, p=0.049) (figure 3).
After multiple imputation for missing treatment indications in treated hypotensive infants (n=54), the association between treatment and the primary outcome remained significant in the propensity score-matched analysis (OR, 1.75; 95% CI 1.02 to 2.95).
Outcomes for infants from the treated, untreated and symptomatic treated groups are summarised in table 2. Infants in this last group had significantly poorer survival without severe morbidity, a higher in-hospital death rate and higher rates of severe cerebral lesions and severe ROP than the other two groups.
Outcomes for the treated, untreated and symptomatic treated groups in the overall cohort
The negative control analysis showed no significant association between antihypotensive treatment and late-onset infection in the propensity score-matched cohort (OR, 0.95 (95% CI 0.54 to 1.69)).
Subgroup analysis
In the subgroup of infants with a minMAP≤GA-5, survival without severe morbidity was significantly higher for the treated group (OR, 3.15; 95% CI 1.28 to 7.74) (see online supplementary table S4).
Discussion
Contrary to our initial hypothesis, antihypotensive treatment was associated with significantly higher survival without severe morbidity at discharge and a lower rate of severe cerebral lesions than was permissive hypotension in ELGANs with early isolated hypotension.
The results from prospective randomised trials currently neither justify the permissive hypotension approach nor demonstrate adequate safety and efficacy for any antihypotensive therapies. Therefore, the numerous observational studies reporting no beneficial effect of antihypotensive treatment3 ,4 ,9 ,10 ,24 probably encourage therapeutic abstention by most clinicians today.
In their initial report on the permissive hypotension strategy, Dempsey et al10 defined hypotension using a criterion very similar to ours (mean arterial blood pressure (MAP)<GA in the first 72 hours). However, according to their protocol, infants with signs of good perfusion—named isolated hypotension in our study—did not receive antihypotensive treatments. All infants who received antihypotensive treatments in Dempsey's study had other predefined signs of poor perfusion. Therefore, the poorer outcome of these treated infants is consistent with our results comparing the untreated and symptomatic treated groups. The treated group as defined in our study, that is, with isolated low BP value and treated with antihypotensive therapy, did not exist in Dempsey et al's study. Batton et al3 compared short-term and long-term outcomes in infants born below 27 weeks GA with treated or untreated low BP. As compared with untreated infants, treated infants had higher mortality in the first postnatal week and comparable neurodevelopmental outcome at 18–22 months postmenstrual age, except for deafness. These results might seem contradictory with ours; however, the reasons for antihypotensive treatment initiation were not provided. Therefore, it is likely that treated infants in Batton's study included both infants with isolated hypotension and symptomatic infants. Our results are thus original and difficult to compare with previous reports because we identified a so far unstudied population of infants.
Severe cerebral lesions on ultrasonography were significantly more frequent in the untreated group and contributed substantially to this group's mortality. The recent German cohort study on more than 4900 preterm infants found that inotropes in the first 24 hours of life were independently associated with all grades of IVH.2 It did not, however, specifically report results for grade III IVH, IPH or PVL and did not collect treatment indications.2 Comparison with our results is therefore difficult. Our observations on IVH are consistent with physiological studies25 ,26 illustrating the pressure passive property of neonatal cerebral perfusion.27
In the subgroup of infants with the most severe hypotension, we found a strong association between antihypotensive treatment and improved outcome, confirming the previously identified threshold of minMAP≤GA-5 as a relevant clinical cut-off for considering antihypotensive treatment.2 ,12
Our study has limitations that mandate caution in the interpretation of our results. We recorded only the lowest MAP value and do not know if the number of BP measurements was identical in untreated and treated groups. We did not record the method used to measure BP (invasive or non-invasive), which is a potential bias. Our definition of hypotension (minMAP<GA in the first 72 hours) is not consensual and certainly imperfect but it is simple, consistent with clinical situations and has been used in previous studies.2 ,10 Among untreated infants, we did not distinguish those who potentially had other signs of poor perfusion, as we did in the treated population. However, not treating a hypotensive infant with signs of poor perfusion is currently considered suboptimal practice10 ,12 and should thus be a rare event. We could not determine with certainty the temporality for some clinical events, that is, if these events included as variables into the propensity score preceded hypotension and/or antihypotensive treatments or if these events happened after. However, clinical considerations favoured the hypothesis that these events preceded any antihypotensive treatment (see online supplement). Finally, our study does not allow any statement as to what the best treatment modality might be.
The strengths of the EPIPAGE 2 study include its population-based design and prospective enrolment of all infants born prematurely in France in 2011 reinforcing its representativeness. The wide variability of bedside practices and our statistical results support the validity of our propensity score. Here, as for other clinical policies, such as PDA screening strategies,28 our analysis can provide results otherwise difficult to identify in randomised trials.29 Finally, this study is the first to our knowledge that has the ability to distinguish, among hypotensive infants who received antihypotensive treatments, those who had only isolated low BP values from those who had additional signs of haemodynamic compromise. As we await pending results from current prospective trials, therapeutic abstention for isolated hypotension in the first 3 days of life is not supported by our study, especially in infants with the lowest BP values.
References
Footnotes
Collaborators Group information: members of the Hemodynamic EPIPAGE2 Study Group: Gilles Cambonie, MD, PhD (Department of Neonatal Medicine, Montpellier University Hospital, Montpellier, France); Jean-Christophe Rozé, MD, PhD (Department of Neonatal Medicine, Nantes University Hospital, Nantes, France); Pierre-Yves Ancel, MD, PhD (INSERM, U1153, Obstetrical, Perinatal and Pediatric Epidemiology Team, Epidemiology and Biostatistics Sorbonne, Paris, France); Laetitia Marchand-Martin, MS (INSERM, U1153, Obstetrical, Perinatal and Pediatric Epidemiology Team, Epidemiology and Biostatistics Sorbonne, Paris, France); Mélanie Durox, MSc (INSERM, U1153, Obstetrical, Perinatal and Pediatric Epidemiology Team, Epidemiology and Biostatistics Sorbonne, Paris, France); Veronique Gournay, MD, PhD (Pediatric Cardiology Unit, Nantes University Hospital, Nantes, France); Xavier Durrmeyer, MD, PhD (Department of Neonatal Medicine, Intercommunal Hospital, Creteil, France); Laurent Storme, MD, PhD (Department of Neonatal Medicine, Lille University Hospital, Lille, France); Raphael Porcher, PhD (INSERM, U1153, METHODS Team, Epidemiology and Statistics Sorbonne Paris Cité Research Center, Paris, France); Patrice Morville, MD (Department of Neonatal Medicine, Reims University Hospital, Reims, France);Olivier Brissaud, MD (Department of Neonatal Medicine, Bordeaux University Hospital, Bordeaux, France); Patrick Truffert, MD, PhD (Department of Neonatal Medicine, Lille University Hospital, Lille, France); Antoine Bouissou, MD (Department of Neonatal Medicine, Tours University Hospital, Tours, France); Isabelle Ligi, MD, PhD (Department of Neonatal Medicine, Marseille University Hospital, Marseille, France); Marie-Odile Marcoux, MD (Department of Neonatal Medicine, Toulouse University Hospital, Toulouse, France); Fabrice Cneude, MD (Department of Neonatal Medicine, Grenoble University Hospital, Grenoble, France); Geraldine Gascoin, MD, PhD (Department of Neonatal Medicine, Angers University Hospital); Gerard Thiriez, MD, PhD (Department of Neonatal Medicine, Besançon University Hospital, Besançon, France); Hugues Patural, MD, PhD (Department of Neonatal Medicine, St Etienne University Hospital, St Etienne, France); Doriane Madeleneau, MD (Department of Neonatal Medicine, Cochin University Hospital, Paris, France); Antoine Burguet, MD, PhD (Department of Neonatal Medicine, Dijon University Hospital, Dijon, France) and Patrick Pladys, MD, PhD (Department of Neonatal Medicine, Rennes University Hospital, Rennes, France).
Contributors XD, RP, GC, J-CR, LS, P-YA and GC initiated and designed the protocol. XD and LM-M participated in the data collection. LM-M performed all data analysis and RP validated them. XD and GC wrote the first draft. All authors participated in data interpretation and reviewing of the manuscript. All the coauthors approved the final manuscript.
Funding This study was supported by the French Institute of Public Health Research /Institute of Public Health and its partners the French Health Ministry, the National Institute of Health and Medical Research, the National Institute of Cancer and the National Solidarity Fund for Autonomy; grant ANR-11-EQPX-0038 from the National Research Agency through the French Equipex Program of Investments in the Future and the PremUp Foundation.
Competing interests None declared.
Ethics approval EPIPAGE-2 was approved by the National Data Protection Authority (Commission Nationale de l'Informatique et des Libertés (CNIL) n°911009) and by two ethics committees: consultative committee on the treatment of information on personal health data for research purposes (approval granted 18 November 2010; reference 10.626) and the committee for the protection of people participating in biomedical research (approval granted 18 March 2011; reference Comité de Protection des Personnes (CPP) SC-2873).
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Fantoms