Article Text

Abstract
Objective To evaluate the performance of a novel rapidly responsive proportional-integral-derivative (PID) algorithm for automated oxygen control in preterm infants with respiratory insufficiency.
Design Interventional study of a 4-hour period of automated oxygen control compared with combined data from two flanking periods of manual control (4 hours each).
Setting Neonatal intensive care unit.
Participants Preterm infants (n=20) on non-invasive respiratory support and supplemental oxygen, with oxygen saturation (SpO2) target range 90%–94% (manual control) and 91%–95% (automated control). Median gestation at birth 27.5 weeks (IQR 26–30 weeks), postnatal age 8.0 (1.8–34) days.
Intervention Automated oxygen control using a standalone device, receiving SpO2 input from a standard oximeter and computing alterations to oxygen concentration that were actuated with a modified blender. The PID algorithm was enhanced to avoid iatrogenic hyperoxaemia and adapt to the severity of lung dysfunction.
Main outcome measure Proportion of time in the SpO2 target range, or above target range when in air.
Results Automated oxygen control resulted in more time in the target range or above in air (manual 56 (48–63)% vs automated 81 (76–90)%, p<0.001) and less time at both extremes of oxygenation. Prolonged episodes of hypoxaemia and hyperoxaemia were virtually eliminated. The control algorithm showed benefit in every infant. Manual changes to oxygen therapy were infrequent during automated control (0.24/hour vs 2.3/hour during manual control), and oxygen requirements were unchanged (automated control period 27%, manual 27% and 26%, p>0.05).
Conclusions The novel PID algorithm was very effective for automated oxygen control in preterm infants, and deserves further investigation.
- Neonatology
- Respiratory
- Intensive Care
Statistics from Altmetric.com
What is already known on this topic?
Automation of oxygen delivery for preterm infants has the potential to more effectively target the desired oxygen saturation (SpO2) range and avoid the extremes of oxygenation.
Previous automated control devices are known to be more effective than routine manual control in SpO2 targeting, but the benefits have generally been modest.
Our recently developed algorithm for automated oxygen control (VDL1.0) was found to be very effective in SpO2 targeting in preclinical testing, and now requires evaluation in preterm infants.
What this study adds?
The VDL1.0 algorithm was considerably more effective in SpO2 targeting than routine manual control, with 25% more time in the desired SpO2 range.
The extremes of oxygenation were largely avoided, and prolonged episodes of hypoxaemia and hyperoxaemia were virtually eliminated.
Effective oxygen control was achieved with very few manual fraction of inspired oxygen adjustments, and similar exposure to oxygen.
Introduction
Oxygen therapy for preterm infants with respiratory dysfunction aims to target a predetermined range of oxygen saturation (SpO2) with the hope of normalising arterial partial pressure of oxygen. Despite the best efforts of bedside caregivers manually adjusting fraction of inspired oxygen (FiO2), this approach regularly finds SpO2 outside the target range for a considerable proportion of the time, both in ventilated infants, and those on non-invasive support.1–3 Automating this process has been seen as a logical goal for nearly four decades,4 and offers the hope of more effective SpO2 targeting, and the benefits that may follow.5
Devices for automated control of oxygen therapy have at their heart an algorithm which compares incoming SpO2 readings with a desired setpoint (normally the midpoint of the target range), and calculates an updated value for FiO2, which is actuated mechanically.5 ,6 Recently reported algorithms differ considerably one from another, both in their responsiveness and the nature of the algorithm for adjusting FiO2.7–9 Nevertheless, each algorithm has been found to more effectively control SpO2 than manual control, although the benefit has generally been modest.7–17 Additionally, in some studies an improvement at one extreme of oxygenation (eg, less hyperoxaemia) has been at the cost of no improvement at the other (eg, equivalent or more hypoxaemia).7 ,9 ,10 Finally, no study has reported an analysis of the performance of the algorithm in each individual, which has relevance given the possibility that an underpowered or overpowered control algorithm could in some cases result in worse SpO2 targeting than manual control.
We have recently developed a rapidly responsive and adaptive algorithm (VDL1.0) for automated oxygen control in preterm infants, in which a proportional-integral-derivative (PID) controller has been enhanced to mitigate iatrogenic hyperoxaemia and adapt to the severity of lung disease. In preclinical testing using simulation, this algorithm has been noted to effectively target a given SpO2 range, with minimisation of hypoxaemia and hyperoxaemia.18
Herein, we report our initial clinical appraisal of the VDL1.0 algorithm in preterm infants on non-invasive respiratory support. We aimed to examine whether, compared with routine manual care, automated oxygen control using the VDL1.0 algorithm would result in a greater proportion of time in the SpO2 target range, less time in both hypoxaemia and hyperoxaemia and fewer prolonged episodes with undesired SpO2 readings. Furthermore, we wished to examine whether the control algorithm performed satisfactorily in each individual, and whether the overall oxygen requirement differed between automated and manual control.
Methods
Study setting
The study was conducted in the Neonatal and Paediatric Intensive Care Unit at the Royal Hobart Hospital. Our unit provides care for ∼70 preterm infants <32 weeks gestation per year, and has an ethos of using non-invasive respiratory support whenever possible for this patient group, including continuous positive airway pressure (CPAP) and high flow nasal cannulae (HFNC). The SpO2 target range for titration of oxygen therapy has been revised to 90%–94%, having previously been 88%–92%.3 The study was approved by our local Ethics Committee, and the automated control device was registered with the Australian Therapeutic Goods Administration. Written informed consent was obtained from parents of each infant prior to study.
Study infants
Preterm infants <37 weeks gestation and <4 months of age were eligible for study if on non-invasive respiratory support (CPAP or HFNC) and receiving supplemental oxygen at the outset of the study period. Infants with acute instability or congenital abnormalities (including cardiac malformations other than patent ductus arteriosus) were excluded.
Automated control equipment
The development of the VDL1.0 algorithm for automated oxygen control is described in full in a companion paper.11 The design and function of the oxygen control device used in this clinical study, including the approach to SpO2 validation and manual override, is outlined in the online supplementary text and depicted in online supplementary figure S1.
Supplemental material
Study procedures
This was a prospective interventional study of a 4-hour period of automated oxygen control, which was compared with two flanking periods of standard manual control totalling 8 hours (4 hours before and after automated control). There was a 15 min interval between study periods to avoid carryover effects. Study personnel were in attendance for the duration of the automated control period, but were not to interact with bedside clinical staff unless there was a critical system malfunction. During automated control, caregivers could override the control device output to the customised air-oxygen blender used in the study by turning the blender dial (see online supplementary text). During the recordings of manual control, bedside caregivers were instructed to use their usual approach to SpO2 targeting, with the standard SpO2 target range (90%–94%). Based on previous studies, it was expected that with manual control the upper end of this range would be preferentially targeted.3 Given that the automated algorithm targets the midpoint of the SpO2 range, during automated control the target range was set at 91%–95%, with the expectation that the manual and automated SpO2 histograms would overlap, with a similar median SpO2. For both manual and automated study epochs, the SpO2 alarm settings were identical—lower limit 89%, upper limit 96%.
Prior to the study, the oximetry probe was placed in a postductal position, and not moved during the three study epochs unless there was a clinical need or a consistently poor SpO2 signal. Care times were scheduled to fall outside the data recording periods where possible. For automated control a constant value for reference FiO2 (rFiO2) was selected in each infant based on most recent basal supplemental oxygen requirements.
Data collection and analysis
Relevant demographic and clinical data were recorded for each infant, including gestation, birth weight and details of clinical state and level of respiratory support at the time of the study. SpO2 and FiO2 were recorded at 1 Hz during both manual and automated control. Analysis of these recordings allowed evaluation of SpO2 instability in each infant, assessed by SpO2 coefficient of variation, and number and mean duration of episodes outside the target range. Furthermore, the proportion of time in each of the following oxygenation states was ascertained: SpO2 in target range, eupoxia (SpO2 in target range or above target range in room air), SpO2 in alarm range (89%–96%) and SpO2<80%, 80%–84%, 85%–88%, 97%–98% in oxygen and >98% in oxygen. For calculation of these values, the denominator was the usable time after exclusion of data during periods of missing SpO2 signal. Frequency of prolonged episodes of hypoxaemia and hyperoxaemia were identified, as was frequency of SpO2 overshoot, defined as SpO2 readings above the target range for at least 60 s over the 2 min following a hypoxaemic event with SpO2<85%.7 ,14 The number of FiO2 adjustments (change in measured FiO2 by 1% or greater) during manual and automated recordings was determined, as was the average oxygen exposure (mean FiO2) in each case.
Data were expressed as median and IQR unless otherwise stated. Comparisons were made between automated and manual control epochs using Wilcoxon matched pairs test. For these analyses data from both manual control epochs were pooled, but additionally the best manual control epoch for each infant (ie, the manual recording of duration ≥2 hours with the greatest proportion of time in eupoxia) was also used as the comparator. The primary outcome was proportion of time in eupoxia. The chosen sample size for the study (20 infants) was primarily based around need to gain an initial clinical experience of control algorithm performance and safety in a sufficient number of subjects. In a previous study of 45 infants, we found proportion of time in the target range when in oxygen to be 30±15% (mean±SD).3 Assuming a similar SD for the differences between paired automated and manual control values in the present study, a sample of 20 infants thus allowed detection of a 10% difference in eupoxia time between automated and manual epochs with 80% power and α error 0.05.19
Results
The study was conducted from May to December 2015. Enrolled infants (n=20) were of median gestational age at birth 27.5 weeks (IQR 26–30 weeks) and birth weight 1130 (940–1400) g. 15 of the 20 infants were male (75%). The infants were studied at a postnatal age of 8.0 (1.8–34) days, corrected gestational age of 31 (29–33) postmenstrual weeks and body weight of 1400 (1120–1960) g. For infants studied on CPAP (n=13), the pressure level at the start of recording was 6 (5–8) cm H2O; for those studied on HFNC (n=7), starting flow rate was 6 (5.5–6.5) L/min. Nurse:patient ratio was 1:2 in all cases.
Data from two flanking periods of manual control were available in 18 infants, with data logging failure and need for intubation immediately after automated control being the reasons for unavailability of a second manual control data recording (one case each). The proportion of missing signal was 2.9 (0.5–5.4)%, 1.7 (0.7–3.4)% and 1.5 (0.8–7.1)% in the first manual, automated and second manual recordings, respectively, leaving 3.8 (3.7–4.0), 3.8 (3.7–3.9) and 4.0 (3.8–4.0) hours of usable time for analysis.
Exemplary data recordings are shown in figure 1, and reveal the typical variability of SpO2 during manual control of FiO2 (figure 1A), which was less prominent during automated control (figure 1B). The capacity of the VDL1.0 algorithm to overcome steady state error even with a fixed value for rFiO2 was also apparent, with effective SpO2 targeting in the face of a rising oxygen requirement well beyond the rFiO2 value (figure 1C).

Representative data recordings. Sample recordings of SpO2 (solid line, Y-axis: % saturation) and FiO2 (dashed line, Y-axis: % oxygen). (A) Infant 5 born at 27 weeks gestation, studied on day 40, on high flow nasal cannulae (HFNC) 6 L/min. Manual control. Eupoxia time 59%. (B) Infant 5, automated control. Eupoxia time 79%. (C) Infant 6 born at 28 weeks gestation, studied on day 1, on continuous positive airway pressure (CPAP) 8 cm H2O. Automated control with rFiO2 set at 29% throughout. Eupoxia time 82%. Note increasing oxygen requirement from 17:30 hours. Clinical staff requested cessation of the study at 19:20 hours, after which the infant was intubated. ⊗: SpO2 data missing for ≥30 s.
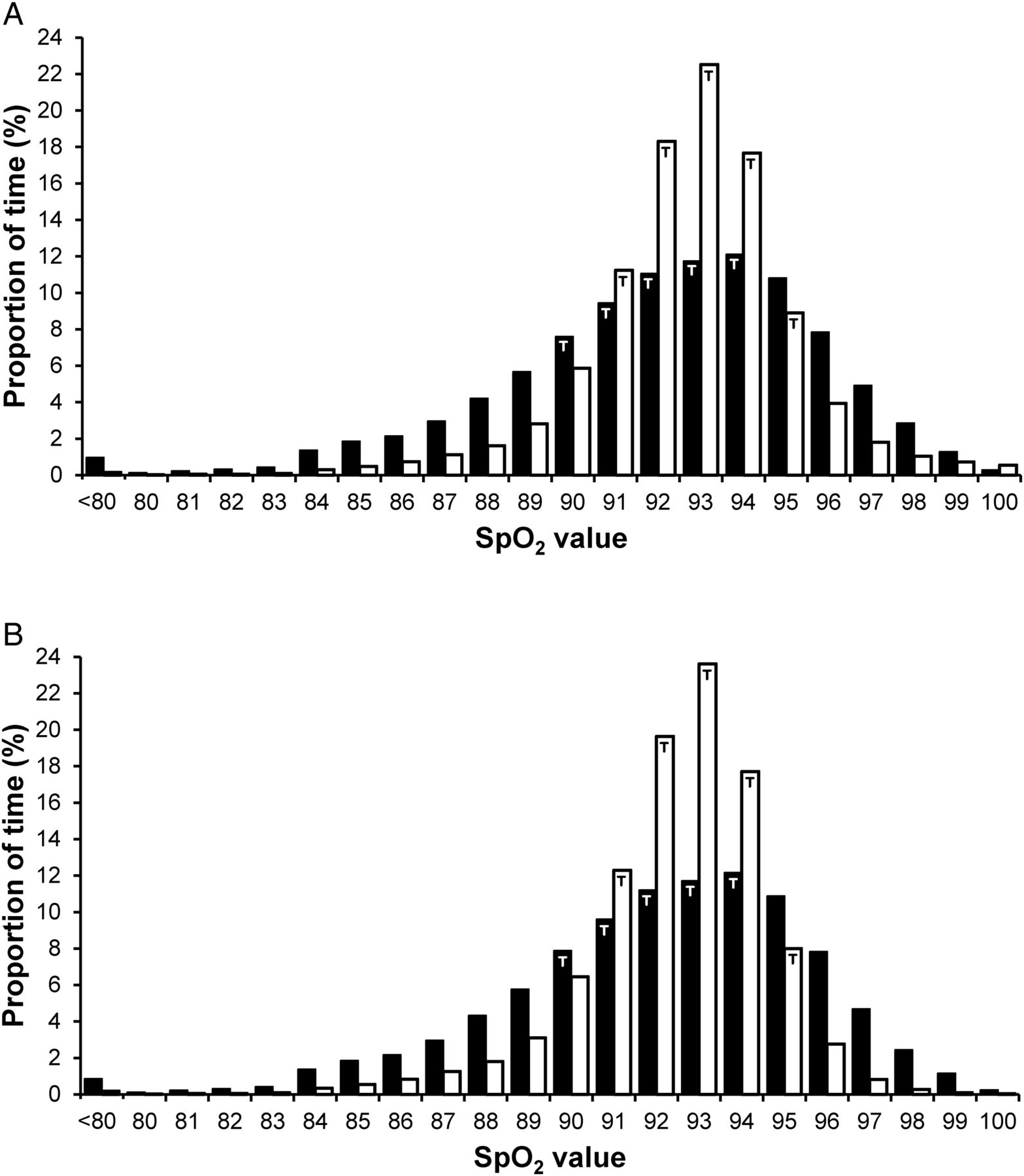
Frequency histograms of pooled SpO2 data show a substantial increase in proportion of time within the target range with automated control (figure 2), with both low and high SpO2 values under-represented compared with manual control. The SpO2 targeting profile during manual control appeared very similar to that published previously,20 ,21 with the peak of the curve at the upper end of the targeted range. By contrast, and as expected, automated control targeted the midpoint of the set target range (ie, SpO2 93%). When receiving supplemental oxygen, median SpO2 in pooled data was 93% for both manual and automated control.
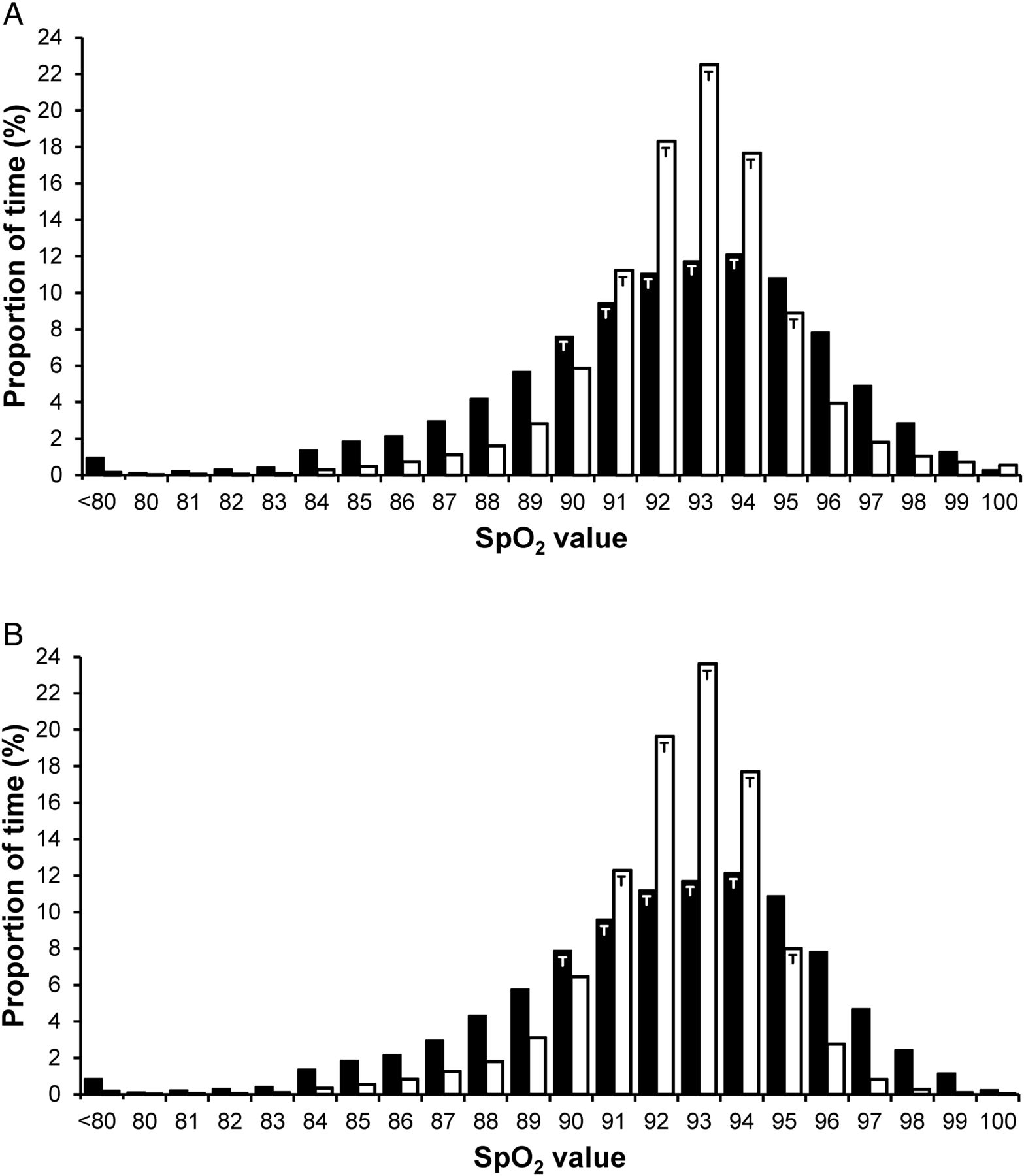
SpO2 histograms. Pooled frequency histograms for proportion of time spent at each SpO2 value, when receiving supplemental oxygen or ambient air (A), or only when receiving supplemental oxygen (B). Black bars: manual control; white bars: automated control. T=SpO2 values within target range (90%–94% for manual control, 91%–95% for automated control).
Oxygenation was considerably more stable during automated control, with fewer SpO2 deviations below target range and below 80%, and a shorter duration of all episodes outside target range compared with manual control (online supplementary table S1). The SpO2 coefficient of variation also differed considerably (manual: 3.8 (3.2–4.7)%, automated: 2.3 (1.8–3.0)%, p<0.0001).
Compared with both manual control epochs combined, automated control resulted in 23% and 25% more time in the target and eupoxic ranges, respectively (table 1). Time spent within the alarm range (89%–96%) was also higher. Automated control considerably diminished time at both extremes of oxygenation, virtually eliminating hypoxaemia with SpO2<80% and hyperoxaemia in oxygen with SpO2>98%. Time spent in the lesser ranges of hypoxaemia and hyperoxaemia was also reduced.
Oxygen saturation (SpO2) targeting
These findings were mirrored in the analysis of prolonged episodes of SpO2 deviation, which occurred with modest frequency during manual control (table 2), but were distinctly uncommon during automated control. No overshoot episodes were identified in any of the automated control recordings.
Hypoxaemic and hyperoxaemic episodes
When measured against the best of the two manual control epochs, the apparent benefit of automated control persisted (figure 3), with time in the eupoxic range being 60 (50–72)% and 81 (76–90)% for best manual and automated control, respectively (p<0.001). Moreover, automated control was associated with better SpO2 targeting in each individual studied, with the relative improvement in eupoxia time ranging from 2.2% to 55% (figure 3).

{kind=link}
{kind=link}
{kind=link}
Comparison of best manual control epoch with automated control. Individual paired values of time in eupoxia for the best manual control epoch compared with automated control. Horizontal bar=median. Eupoxia=SpO2 in target range, or above target range when in room air.
Effectiveness of SpO2 targeting during manual control appeared to diminish somewhat in the period after the automated control trial (eupoxia time manual epoch 1: 63 (57–71)%; epoch 2: 60 (51–72)%, p=0.041).
No differences in performance of the algorithm in SpO2 targeting were noted between infants on CPAP and those on HFNC, infants with or without a patent ductus arteriosus or between subjects with higher or lower oxygen requirements (data not shown).
During manual control epochs, FiO2 adjustments of at least 1% were made 2.3 (1.3–3.4) times/hour by bedside staff. During automated control, the minimum alteration to FiO2 of 0.5% was being actuated by the servomotor frequently (9.9 alterations/min overall), and changes to measured FiO2 of at least 1% occurred at a frequency of 64 (49–98) /hour. When in automated control, a total of 18 manual adjustments were made in all 20 recordings (0.24 adjustments/hour), a reduction by 90% from the rate of manual adjustments observed during manual control (2.3/hour). The maximum number of manual adjustments in an individual subject during automated control was four in a 4-hour recording (ie, 1/hour). No critical system malfunctions occurred.
Median values for oxygen requirement (average FiO2) were 27 (25–30)%, 27 (25–30)% and 26 (24–31)% for first manual, automated and second manual recordings, respectively. Oxygen requirements did not differ between automated and either manual recording (p>0.05, Wilcoxon matched pairs test).
Discussion
Automated control of oxygen therapy in the preterm infant affords the possibility of more effectively targeting a given SpO2 range and avoiding the extremes of oxygenation. In this first clinical study of a novel control algorithm, we found automated oxygen control to result in a 25% increase in the proportion of time spent in the desired SpO2 range compared with manual control, with a benefit noted in each individual studied. Time in hypoxaemic and hyperoxaemic ranges was considerably reduced during automated control, and prolonged episodes of significant SpO2 deviation (SpO2<80% and SpO2>98% when in oxygen) were virtually eliminated. During automated control, there was a 90% reduction in manual FiO2 adjustments, suggesting that automated control can optimise oxygen administration while reducing staff workload.
We chose to make an initial clinical evaluation of the VDL1.0 algorithm in preterm infants receiving non-invasive respiratory support (CPAP or HFNC) and supplemental oxygen. Our focus on non-invasive respiratory support was in recognition of the high proportion of time that preterm infants spend on these modalities, combined with the difficulties in SpO2 targeting that are regularly encountered in this group.3 ,14 Our study group was 1–2 weeks more mature in gestation at birth than most previous reports, but were studied at an earlier postnatal age (median 8 days) than most other investigations.
The reshaping of the manual control SpO2 histogram that was noted during automated control (figure 2) demonstrates the potential effectiveness of the VDL1.0 algorithm, with a more prominent peak in frequency within the SpO2 target range, narrowing of the shoulders of both mild hypoxaemia and hyperoxaemia, and near extinction of the undesired tails of the SpO2 distribution at the extremes of oxygenation. Numerically, this amounted to a greater divergence between automated and routine manual control in relation to time in the desired SpO2 range than has been noted in other studies (25% as against 24%,9 16%,10 13%,15 11%,12 9%,8 8%,11 7%,13 5%14 and 4%16). The VDL1.0 algorithm also appeared to more effectively eliminate serious hypoxaemia with SpO2<80% (0.15% of time overall vs 0.9%,14 1%,15 2%,16 3%13 and 10%11), and iatrogenic hyperoxaemia with SpO2>98% in oxygen (0.13% vs 0.2%,16 0.4%,14 0.7%11 and 3%10). These comparisons between studies are presented with the acknowledgement that the propensity to SpO2 instability among the infants, and assiduousness of the caregivers in providing manual control, are likely to have differed between them. Differences in the SpO2 target ranges used in the studies may also have contributed to the individual study results.
The virtual elimination of prolonged episodes of hypoxaemia and hyperoxaemia was an important finding of our study. A reduction in such episodes perhaps represents the greatest potential for a lasting clinical benefit of automated oxygen control. The relationship between long-lasting hyperoxaemic episodes and retinopathy of prematurity is well-established,22 and their avoidance appears to reduce the incidence of this complication.23 Similarly, intermittent hypoxaemic episodes appear to be an important contributor to the risk of adverse outcomes in early life in preterm infants, including mortality24 and retinopathy.25 Prolonged hypoxaemic episodes in early life may also have later consequences, with a high frequency of 60 s events with SpO2<80% being associated with a 53% higher risk of late death (beyond 36 postmenstrual weeks) or serious neurological disability.26 The duration of these events has been found to be a more important determinant of outcome than the mere presence of hypoxaemia.26
A further significant finding of the present study was that during automated control an improvement in SpO2 targeting was achieved with far fewer manual FiO2 adjustments than during manual control. The implication is that bedside caregivers rapidly gain confidence in the control algorithm, which they can observe to be making frequent alterations to FiO2 (one every 6 s on average) in order to maintain SpO2 in the target range. While the presence of a researcher at the bedside may have also been a deterrent to adjusting FiO2, evidence for a degree of reliance on the control algorithm comes from the slight diminution in time in the SpO2 target range during the period of manual control following the automated control trial.
Our study has several limitations beyond those already identified. The study was not blinded, with both clinicians and researchers aware of the study intervention sequence. Automated control was only tested over a 4-hour period, with a researcher at the bedside throughout. Further trials over a longer period are clearly necessary, during which clinicians interact autonomously with the control device. The automated control algorithm was neither programmed to evaluate performance and auto-tune, nor to detect and respond to hypoxaemia-provoking events such as apnoea or loss of circuit pressure. These novel features will be evaluated in future studies, and may further enhance SpO2 targeting in the most vulnerable preterm infants. We elected not to invoke a specific guideline for SpO2 targeting during the manual control epochs, which may have led to a more consistent approach to manual FiO2 adjustments, although perhaps not an improvement in SpO2 targeting.27 Finally, for consistency we chose a postductal position for the SpO2 sensor, which may have influenced SpO2 stability in infants with patent ductus arteriosus, although equally so for automated and manual control.
Conclusion
The novel PID algorithm was very effective for automated oxygen control in preterm infants, with a considerable improvement in time in the desired SpO2 range, and near-elimination of hypoxaemic and hyperoxaemic episodes. This algorithm, with further enhancements to individualise its performance, deserves more protracted and wide-ranging investigation, including studies in ventilated infants, and during resuscitation.
References
Footnotes
Correction notice This paper has been amended since it was published Online First. References 17 and 18 were in the wrong order.
Acknowledgements We thank the clinical staff of the Royal Hobart Hospital Neonatal and Paediatric Intensive Care Unit and the parents of participating infants for their cooperation and engagement in this study.
Contributors GKP: conducted the study, compiled and analysed the data (with PAD), co-wrote the first draft of the manuscript (with PAD) and approved the final version. KIW: co-conceived the study (with PAD, TJG), reviewed and edited the manuscript and approved the final version. SKMA: assisted with study conduct, reviewed and edited the manuscript and approved the final version. OSF, RJ: identified enhancements to the automated control algorithm, reviewed and edited the manuscript and approved the final version. TJG: conceived the algorithm (with PAD) and this study (with PAD, KW), oversaw its conduct, reviewed and edited the manuscript and approved the final version. PAD: conceived the algorithm (with TJG) and this study (with TJG, KW), oversaw its conduct, co-wrote the first draft of the manuscript (with GKP) and approved the final version.
Funding Supported by a starter grant (12-019) from the Royal Hobart Hospital Research Foundation.
Competing interests The University of Tasmania and Royal Hobart Hospital have jointly lodged a provisional patent application concerning automated control of inspired oxygen concentration in the newborn infant.
Ethics approval University of Tasmania Human Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Original study data available for sharing on request.