Article Text

Abstract
Objective To compare health-related quality of life (HRQOL) at 8 years in children born extremely preterm (EP) with contemporaneous term-born controls over three epochs: 1991–92, 1997 and 2005.
Design Prospective recruitment of geographic cohorts across three distinct eras. Utilities were calculated from the parent-completed Health Utilities Index (HUI), version 2 (1991–92 and 1997 cohorts) and version 3 (2005 cohort). Differences in utilities >0.05 are clinically important.
Setting The state of Victoria, Australia.
Patients 475 EP (<28 weeks’ gestation) and 570 term controls.
Main outcome measures Utilities of children born EP compared with term controls within each era, and paired differences between an EP and matched controls compared across eras.
Results Overall, 86% of survivors had utility data at 8 years of age; 475 EP and 570 controls. In all eras, parent-reported utilities were lower for children born EP compared with controls (difference in medians (95% CIs); 1991–92, −0.053 (–0.071 to –0.035); 1997, –0.053 (−0.072 to –0.034); 2005, –0.082 (−0.097 to –0.068)). Mean differences (MD) between EP children and matched controls within each era were lower in the 2005 cohort compared with both the 1991–92 cohort (MD −0.054, 95% CI −0.097 to –0.010) and the 1997 cohort (MD −0.053, 95% CI −0.097 to –0.009).
Conclusion Children born EP in the postsurfactant era have clinically important reductions in parent-reported HRQOL compared with controls, which may be worsening over time.
- neonatology
- statistics
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Deidentified individual participant data will not be made available.
Statistics from Altmetric.com
What is already known on this subject?
Children born extremely preterm (EP) have higher rates of neurodevelopmental impairment compared with controls born at term.
Some studies suggest children born EP also have poorer health-related quality of life (HRQOL) compared with controls born at term.
What is not known is if the trend to poorer HRQOL in children born EP compared with controls has changed during the postsurfactant era.
What this study adds?
Survivors born EP have a poorer parent-reported HRQOL at 8 years compared with controls on repeated occasions during the postsurfactant era.
The difference in HRQOL between children born EP and term-born controls appears to be widening over time.
Introduction
As survival rates of infants born extremely preterm (EP, <28 weeks’ gestation) have increased with advances in perinatal and neonatal care,1 2 the quality of their survival assumes more importance. Compared with their term-born counterparts, children born EP have higher rates of cerebral palsy, intellectual disability and visual and hearing deficits,3–6 as well as increased behavioural, attention and learning difficulties.7–12 Higher rates of functional limitations have also been demonstrated in this population, including reduced participation in physical activity, difficulty in communicating and socialising and greater rates of mental health issues.3 13 Of concern, we have reported that outcomes may not be improving as survival rates have increased; indeed, some outcomes at early school-age may be worse, including academic performance,14 motor function15 and executive function.16
It is one thing for clinicians and researchers to determine impaired functioning in specific domains in children born EP compared with controls in clinical or research settings. It is another for the families themselves to provide assessments of their child’s everyday functioning at home in multiple domains, such as self-care, pain and emotional functioning. Such information from parents is important to estimate their child’s health-related quality of life (HRQOL). Given the higher rate of impairments in children born EP compared with controls, and that some outcomes may be deteriorating over time, as described above, one might expect HRQOL to be worse in children born EP compared with controls, and that the gap might be widening over time. Studies assessing HRQOL in preschool and school-aged children born preterm or low birth weight, using parental proxies, have reported significantly worse HRQOL scores compared with controls,17–21 but these studies mostly predate the introduction of surfactant into clinical practice in the early 1990s. What is not known is whether HRQOL in children born EP has changed over time in the postsurfactant era.
The aim of this study was to compare HRQOL at 8 years of age of children born EP with controls born at term across three epochs after surfactant was introduced into clinical care in 1991 in Victoria, Australia. It was hypothesised that HRQOL would be poorer in the EP group compared with term-born controls, and since other outcomes at school-age had deteriorated, as described above,14–16 that the difference in HRQOL between groups would have widened across eras.
Methods
This study is a secondary analysis of data collected from cohorts of consecutive survivors born EP in the state of Victoria in three discrete epochs: 1991–92, 1997 and 2005 and contemporaneous term-born controls who have been followed from birth and assessed most recently at approximately 8 years of age, as described elsewhere.14 Children born EP were matched with controls born at term (≥37 weeks’ gestational age) who were randomly selected from births in one of the three tertiary maternity hospitals in the state for the expected date of delivery of an EP survivor, sex, the mother’s health insurance status (as a marker of socioeconomic status) and the primary language spoken in the mother’s country of birth (English or other). Other sociodemographic data collected included years of maternal education (dichotomised into lower and higher around the median years of schooling for that cohort), and social class (based on the occupation of the major income earner in the family and categorised as lower (unskilled or unemployed) or higher (semi-skilled, skilled or professional)).
For this report, parents of children self-completed different versions of the Health Utilities Index; the Health Utilities Index 2 (HUI2) for the 1991–92 and 1997 cohorts, and the Health Utilities Index 3 (HUI3) for the 2005 cohorts. The HUI2 and HUI3 are widely used tools to provide a measure of health status and HRQOL. The HUI2 assesses seven domains (number of levels) of sensation (4) mobility (5) emotion (5) cognition (4) self-care (4) pain (5) and fertility (3) the last of which is not relevant to children aged 8 years. The HUI3 assesses eight domains of vision (6) hearing (6) speech (5) ambulation (6) dexterity (6) emotion (5) cognition (6) and pain (5). For each index scoring is based on community preference measurements and then converted to utility scores using an algorithm, with 1.00=perfect health, and less than perfect health <1.00, and even <0 under some circumstances.22 The HUI3 is a reliable and valid tool that has been demonstrated to be sensitive to change in health status over time.23 A mean utility score difference of 0.05 is considered clinically meaningful, with some studies suggesting that differences of 0.03 could also be considered clinically important.24 25
Data were analysed using STATA V.16.0 and SPSS for Windows V.26. Since the distribution of utilities was skewed, differences between EP and control groups within each era were compared using quantile regression. To normalise the distribution of utility data, differences in utilities between EP and control individuals within each era were computed within pairs formed by aligning an EP survivor with the next available control, with both groups in chronological order of expected date of birth. Differences in paired utilities between 2005 and each of the earlier eras were compared using regression models fitted with generalised estimating equations with robust SEs to allow for a lack of independence of data within multiples from the same family, with and without adjustment for lower social class and lower maternal education.
Results
Participant flow for each cohort within each era is summarised in table 1.
Participant data flow
Survival rates to 8 years of age were lowest in 1991–92 before increasing in 1997, and falling again in 2005. Follow-up rates to obtain utility data were high for all cohorts, ranging from 85% to 89%. Perinatal characteristics between survivors with and without utility data were similar across cohorts (online supplemental table 1). table 2
Supplemental material
Perinatal data and 8-year characteristics of the cohorts with utility data at 8 years of age
Perinatal and 8 years data are shown for each cohort in each era in table 2. The mean gestational ages and birth weights were similar across all three cohorts. Antenatal corticosteroids were prescribed more, and caesarean births were more common in 1997 and 2005 compared with 1991–92, while postnatal corticosteroids were prescribed less in 2005 than either of the earlier cohorts. Rates of grade 3 or 4 intraventricular haemorrhage were similar in the 1991–92 and 2005 cohorts, with a drop in the 1997 cohort. Rates of IQ <−2 SD, cerebral palsy, blindness and deafness were comparable across the three cohorts. In all cohorts, there was a greater proportion of mothers with lower education and socioeconomic status in the EP groups, compared with those in the control groups.
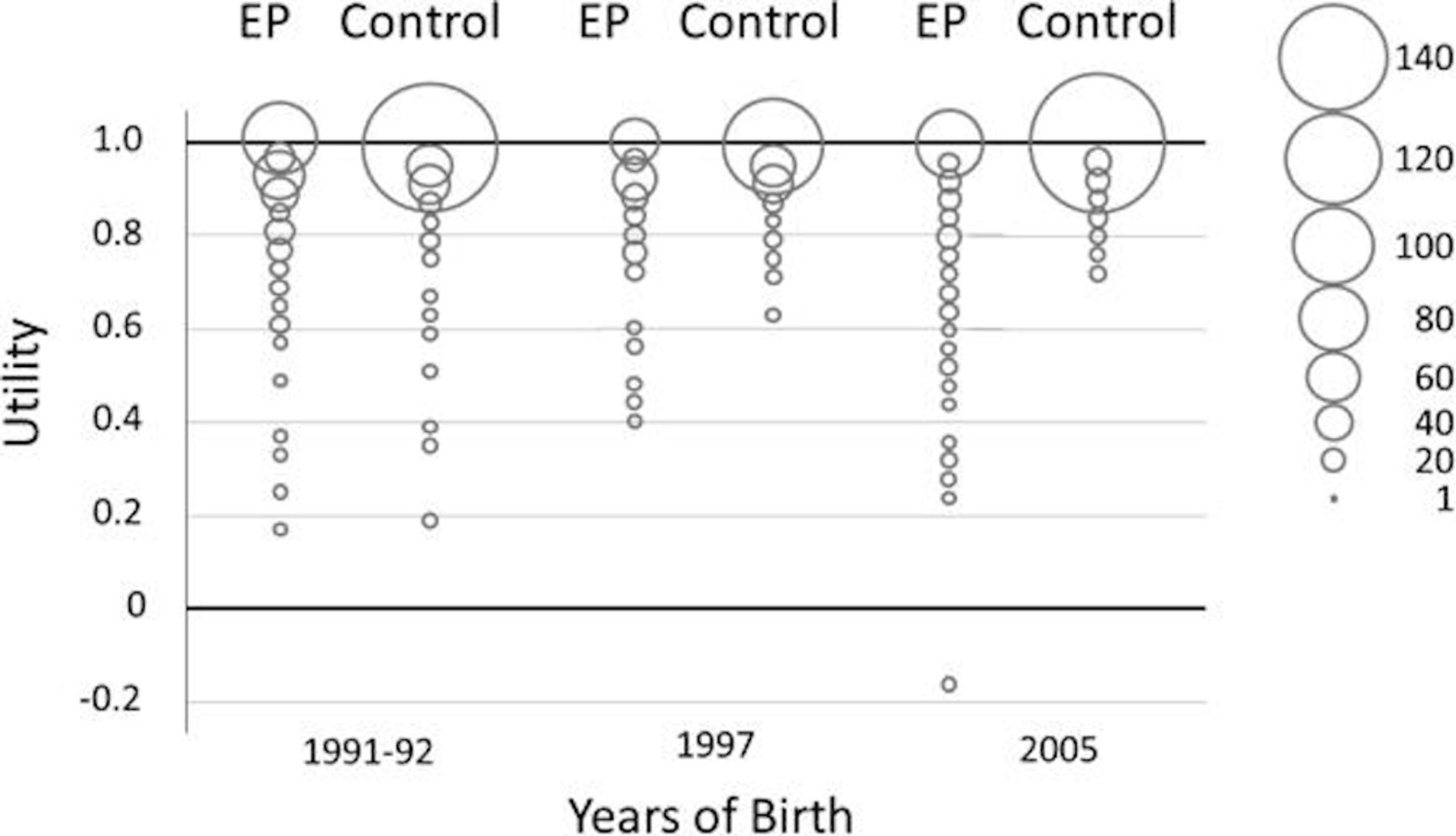
In all eras, most survivors had utilities close to 1.0 (figure 1), but there was a wide range documented. The utilities were more widely distributed in the EP groups than in controls in each era.

Distribution of utilities across groups and eras. Size of circles is proportional to sample size with similar values. EP, extremely preterm.
There was strong evidence that median utilities were lower for children born EP compared with controls within each era (table 3), with differences in the median utilities between EP and control groups all larger than 0.05 in all epochs.
Median utilities compared between groups, within each era
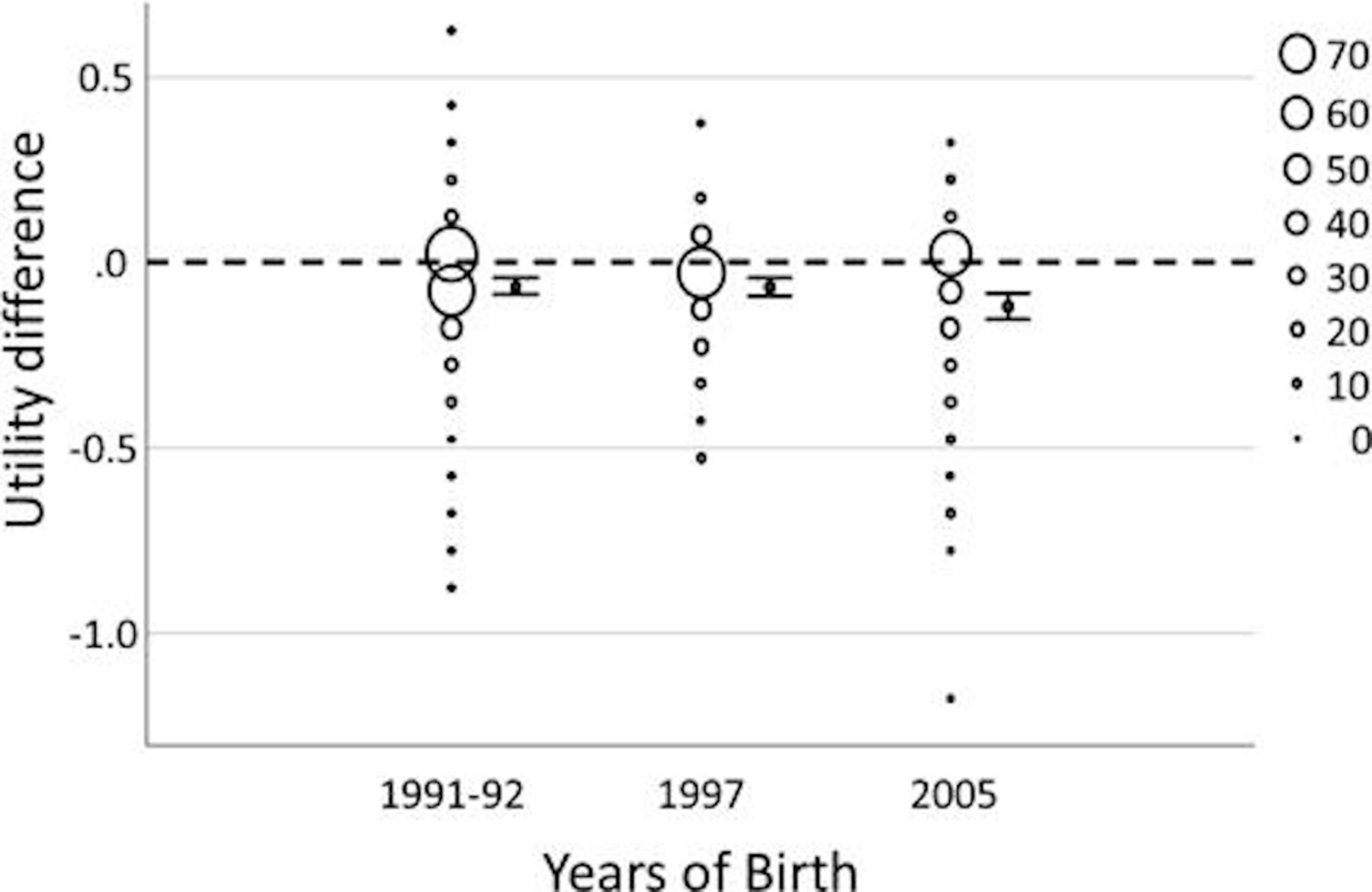
Mean differences (MD) in utilities within pairs between EP and control groups were substantially below zero in each era (figure 2), consistent with the differences in median utilities between EP and control groups in each era.

{kind=link}
{kind=link}
Differences in utilities between extremely preterm and control individuals within pairs for each era. Size of circles is proportional.
There was evidence that the MDs were lower between EP and control groups in the 2005 cohort compared with both the 1991–92 cohort (MD −0.054, 95% CI −0.097 to –0.010, p=0.015) and the 1997 cohort (MD −0.053, 95% CI −0.097 to –0.009, p=0.018). For all groups combined, lower maternal education and lower social class were both associated with lower utility scores (lower maternal education; MD −0.026, 95% CI −0.041 to –0.011; lower social class MD −0.049, 95% CI −0.066 to –0.031). Adjusting for lower social class and lower maternal education did not alter any conclusions for the MDs between EP and control groups in the 2005 cohort compared with both the 1991–92 cohort (adjusted MD −0.051, 95% CI −0.087 to –0.015, p=0.006) and the 1997 cohort (adjusted MD −0.040, 95% CI −0.076 to –0.004, p=0.028).
Discussion
The findings in the current study confirm that children born EP have worse parent-reported HRQOL compared with controls born at term. Not only is the difference between groups remaining across eras, it appears to be widening over time, which we hypothesised would occur because of the poorer academic, motor and executive functioning in the 2005 cohort born EP compared with the earlier eras.14–16 Moreover, the magnitudes of the differences between groups and across eras are clinically important, exceeding 0.05. We are unaware of any other studies that have reported changes in HRQOL of children born EP across different eras in the postsurfactant era.
The differences demonstrated between EP and control groups in our study are in keeping with previous studies in preschool and school-aged children born preterm or low birth weight which have demonstrated significantly worse HRQOL scores compared with controls.17–21 Chien et al reported that children aged 3–4 years born <1500 g birth weight in Taiwan in 1998–2000 had lower physical, emotional, social and cognitive function as reported by parents than controls born >2499 g birth weight.17 Similarly, Theunissen et al found that preschool children born <32 weeks’ gestation in The Netherlands in 1996 had poorer function in several domains than children born more mature on parental report.18 In the first school-age report of quality of life, Saigal et al 19 20 studied 156 children aged 8 years who were born weighing <1001 g between 1977 and 1982 and 145 controls; children born <1001 g had lower overall utility scores as well as more limitations in cognition, sensation mobility and self-care than did controls, but not in emotion or pain. In a study of 35 children aged 10 years born <28 weeks or <1000 g birth weight in 1991–1992 and an equal number of term-born controls in Norway, Vederhus et al reported that the preterm group had more difficulties identified on the Child Health Questionnaire-Parent Form than did controls.21 In a large study from France, Gire et al reported that children aged 8 years born <28 weeks’ gestation in 2004–2007 had lower HRQOL than reference children, although the children themselves identified different areas of concern than did their parents.26
Findings are more variable when assessing HRQOL in adolescents and young adults born preterm or low birth weight; results have been synthesised in several different reviews.27 28 In these older ages most studies report no substantial differences in HRQOL between those born preterm or low birth weight and controls, particularly if the participant was reporting on their own HRQOL. Although the 1991–92 cohort born EP in the current study had lower utility scores than controls at 8 years on parental report, when they were 18 years of age their HRQOL on self-report was no different from controls.29
The strengths of the current study include the prospective recruitment of geographic cohorts across three distinct eras, with contemporaneous matched controls, and high follow-up rates. A major limitation includes the use of two different editions of the HUI, which assess mostly different domains with different levels within each domain, and thus we could not compare groups within individual domains across all eras. Utilities obtained from the HUI3 tend to be lower than the HUI2; in our study, the utilities obtained with the different versions were similar across the three different control groups, as seen in table 3. However, the distribution of utilities was lower for the EP group born in 2005 compared with the earlier two eras, and the widening gap between EP and control groups in the 2005 cohorts may in part be explained by the different versions of the HUI rather than a true deterioration in the EP group in 2005 compared with earlier eras. On the other hand, we attempted to address the possible problems with different versions of the HUI by calculating MDs between EP and control groups within each era, and then contrasting the MDs across eras. Thus, it remains possible that the widening of the gap between the EP and control groups in the 2005 era represents a deterioration in everyday functioning, and is consistent with the poorer academic, motor and executive performance noted in the 2005 cohort compared with earlier eras when these variables were assessed independently in previous reports.14–16 Another limitation is the use of parent-reports, rather than self-reports. An individual’s HRQOL is reliant on their own self-perception of their current state and future ambitions, whereas parental reports are likely to be influenced by the parent’s own values and beliefs, which may be incongruous with the child’s experience. However, at age 8 years, there may be issues related to reliability of self-reports of HRQOL.
Given the disparity in the literature on self-reported HRQOL, it is important to continue to follow these cohorts to assess their self-reported HRQOL in adolescence and young adulthood, with the same version of the HUI, and to compare results across eras. It would also be useful to assess the difference in utility scores between the EP and control groups within each domain, to gain an idea of what areas are contributing most to overall poorer HRQOL. Knowing more precisely the areas of difficulty could direct the focus for interventions designed to optimise long-term outcomes for the increasing numbers of EP survivors now reaching adulthood.
In conclusion, children born EP in the postsurfactant era have worse parent-reported HRQOL compared with term-born controls, and the gap may be widening over time. We need to understand why these differences are occurring and reduce or eliminate the discrepancy between EP and control groups in HRQOL in future cohorts.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Deidentified individual participant data will not be made available.
Ethics statements
Ethics approval
The study was approved by the Human Research Ethics Committees at the Royal Women’s Hospital, Mercy Hospital for Women, and Monash Medical Centre (Melbourne, Australia) (2005 04/44 1997 97/04 1991-92 08/06). The follow-up was considered part of the routine clinical care for children born EP in the 1991–92 and 1997 cohorts.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Collaborators The Victorian Infant Collaborative Study Group: Jeanie Cheong (Neonatal Services, Royal Women’s Hospital, Melbourne, Australia; Victorian Infant Brain Studies, Murdoch Children’s Research Institute, Melbourne, Australia; Department of Obstetrics & Gynaecology, University of Melbourne, Melbourne, Australia; Premature Infant Follow Up Program, Royal Women’s Hospital, Melbourne, Australia), Collaborators (in alphabetical order): Peter Anderson (Victorian Infant Brain Studies, Murdoch Children’s Research Institute, Melbourne, Australia; Department of Obstetrics & Gynaecology, University of Melbourne, Melbourne, Australia; Premature Infant Follow Up Program, Royal Women’s Hospital, Melbourne, Australia), Merilyn Bear (Victorian Infant Brain Studies, Murdoch Children’s Research Institute, Melbourne, Australia; Premature Infant Follow Up Program, Royal Women’s Hospital, Melbourne, Australia), Rosemarie Boland (Victorian Infant Brain Studies, Murdoch Children’s Research Institute, Melbourne, Australia; Department of Obstetrics & Gynaecology, University of Melbourne, Melbourne, Australia), Alice Burnett(Victorian Infant Brain Studies, Murdoch Children’s Research Institute, Melbourne, Australia; Department of Obstetrics & Gynaecology, University of Melbourne, Melbourne, Australia; Department of Paediatrics, University of Melbourne, Melbourne, Australia; Department of Neonatal Medicine, Royal Children’s Hospital, Melbourne, Australia), Margaret Charlton (Department of Neonatology, Monash Medical Centre, Melbourne, Australia), Marissa Clark (Premature Infant Follow Up Program, Royal Women’s Hospital, Melbourne, Australia), Janet Courtot (Department of Neonatology, Monash Medical Centre, Melbourne, Australia), Noni Davis (Premature Infant Follow Up Program, Royal Women’s Hospital, Melbourne, Australia), Lex Doyle (Neonatal Services, Royal Women’s Hospital, Melbourne, Australia; Victorian Infant Brain Studies, Murdoch Children’s Research Institute, Melbourne, Australia; Department of Obstetrics & Gynaecology, University of Melbourne, Melbourne, Australia; Premature Infant Follow Up Program, Royal Women’s Hospital, Melbourne, Australia; Department of Paediatrics, University of Melbourne, Melbourne, Australia), Julianne Duff (Premature Infant Follow Up Program, Royal Women’s Hospital, Melbourne, Australia), Rachel Ellis (Victorian Infant Brain Studies, Murdoch Children’s Research Institute, Melbourne, Australia; Premature Infant Follow Up Program, Royal Women’s Hospital, Melbourne, Australia), Anjali Haikerwal (Premature Infant Follow Up Program, Royal Women’s Hospital, Melbourne, Australia), Leah Hickey (Department of Paediatrics, University of Melbourne, Melbourne, Australia; Department of Neonatal Medicine, Royal Children’s Hospital, Melbourne, Australia), Marie Hayes (Department of Neonatology, Monash Medical Centre, Melbourne, Australia), Elisha Josev (Neonatal Services, Mercy Hospital for Women, Melbourne, Australia), Elaine Kelly (Premature Infant Follow Up Program, Royal Women’s Hospital, Melbourne, Australia; Neonatal Services, Mercy Hospital for Women, Melbourne, Australia), Katherine Lee (Clinical Epidemiology and Biostatistics, Murdoch Children’s Research Institute, Melbourne, Australia), Marion McDonald (Premature Infant Follow Up Program, Royal Women’s Hospital, Melbourne, Australia), Emma McInnes (Victorian Infant Brain Studies, Murdoch Children’s Research Institute, Melbourne, Australia; Premature Infant Follow Up Program, Royal Women’s Hospital, Melbourne, Australia), Bronwyn Novella (Neonatal Services, Mercy Hospital for Women, Melbourne, Australia), Joy Olsen (Victorian Infant Brain Studies, Murdoch Children’s Research Institute, Melbourne, Australia; Premature Infant Follow Up Program, Royal Women’s Hospital, Melbourne, Australia), Gillian Opie (Department of Obstetrics & Gynaecology, University of Melbourne, Melbourne, Australia; Neonatal Services, Mercy Hospital for Women, Melbourne, Australia), Gehan Roberts (Victorian Infant Brain Studies, Murdoch Children’s Research Institute, Melbourne, Australia; Department of Paediatrics, University of Melbourne, Melbourne, Australia; Population Health, Murdoch Children’s Research Institute, Melbourne, Australia), Katherine Scott (Neonatal Services, Mercy Hospital for Women, Melbourne, Australia), Alicia Spittle (Neonatal Services, Royal Women’s Hospital, Melbourne, Australia; Victorian Infant Brain Studies, Murdoch Children’s Research Institute, Melbourne, Australia; Department of Physiotherapy, University of Melbourne, Melbourne, Australia), Penelope Stevens (Department of Neonatology, Monash Medical Centre, Melbourne, Australia), Anne-Marie Turner (Neonatal Services, Mercy Hospital for Women, Melbourne, Australia).
Contributors SP interpreted the data, and drafted and revised the article. JLYC and LWD conceived and designed the study, analysed and interpreted the data and revised the article. PJA conceived and designed the study, and revised the article. GR and ND were involved in data collection and revised the article.
Funding Supported by grants from the National Health and Medical Research Council of Australia (Centre of Clinical Research Excellence #546519; Centres of Research Excellence #1060733 and #1153176; Project Grant #108702, Leadership Fellowship #1176077 to PJA), Medical Research Future Fund (Career Development Fellowship #1141354 to JC) and the Victorian Government’s Operational Infrastructure Support Program.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.