Article Text

Abstract
Objective Closed-loop automatic control (CLAC) of the fractional inspired oxygen (FiO2) improved oxygen administration to preterm infants on respiratory support. We investigated whether a revised CLAC algorithm (CLACfast, ≤2 FiO2 adjustments/min), compared with routine manual control (RMConly), increased the proportion of time with arterial haemoglobin oxygen saturation measured by pulse oximetry within prespecified target ranges (Target%) while not being inferior to the original algorithm (CLACslow: ≤0.3 FiO2 adjustments/min).
Design Unblinded randomised controlled crossover study comparing three modes of FiO2 control in random order for 8 hours each: RMC supported by CLACfast was compared with RMConly and RMC supported by CLACslow. A computer-generated list of random numbers using a block size of six was used for the allocation sequence.
Setting Two German tertiary university neonatal intensive care units.
Patients Of 23 randomised patients, 19 were analysed (mean±SD gestational age 27±2 weeks; age at randomisation 24±10 days) on non-invasive (n=18) or invasive (n=1) respiratory support at FiO2 >0.21.
Main outcome measure Target%.
Results Mean±SD [95% CI] Target% was 68%±11% [65% to 71%] for CLACfast versus 65%±11% [61% to 68%] for CLACslow versus 58%±11% [55% to 62%] for RMConly. Prespecified hypothesis tests of: (A) superiority of CLACfast versus RMConly and (B) non-inferiority of CLACfast versus CLACslow with margin of 5% yielded one-sided p values of <0.001 for both comparisons.
Conclusions This revised and faster CLAC algorithm was still superior to routine care in infants on respiratory support and not inferior to a previously tested slower algorithm.
Trial registration number NCT03163108.
- Neonatology
- Respiratory
- controller
- ventilation
- hypoxia
Statistics from Altmetric.com
What is already known on this topic?
Keeping pulse oximeter saturation (SpO2) within target range is challenging in preterm infants on respiratory support receiving supplemental oxygen.
Frequent hypoxaemic episodes are associated with clinically relevant long-term outcome.
Support by automatic control of fractional inspired oxygen (FiO2) increases time within desired SpO2 target range.
What this study adds?
A revised and faster algorithm increased the time preterm infants receiving non-invasive respiratory support spent within SpO2 target range compared with routine manual control.
The faster responding algorithm was not inferior to a previously tested more slowly responding algorithm.
Introduction
Supplemental oxygen therapy for extremely preterm infants on respiratory support remains challenging. Recent data suggested a rather narrow target range of 91%–95% arterial haemoglobin oxygen saturation measured by pulse oximetry (SpO2).1 At the same time, pronounced fluctuations in SpO2 should be avoided to prevent oxygen-related morbidity.2–5
Adjustments of the fractional inspired oxygen (FiO2) are usually carried out by staff members. Closed-loop automatic oxygen control (CLAC) systems, however, have been shown to prolong the time SpO2 remains within a desired target range.6 7 This could potentially lead to a reduction in oxygen-related morbidity while reducing workload.
Based on a simple mathematical algorithm, clinical decision rules and software solutions,8 9 we developed a CLAC system and investigated its safety and efficacy in two single-centre10 11 and one multicentre study.6 We found that routine manual control (RMC) supported by CLAC significantly prolonged the time with SpO2 within a desired range compared with RMC alone.
To prevent iatrogenic and/or unnecessarily wide fluctuations in FiO2 and SpO2, we had originally integrated a waiting period of 180 s into the algorithm during which further automated adjustments were suspended. CLAC users, however, demanded faster responsiveness and suggested that this ‘wait time’ may be too long to adequately compensate acute hypoxaemia and/or hyperoxaemia. We, thus, revised the CLAC algorithm now allowing ≥30 s wait time between adjustments (ie, CLACfast). However, we were concerned about the safety and efficacy of the new algorithm and decided to investigate whether CLACfast is still superior compared with RMConly and, if that is confirmed, not inferior to the previously evaluated conventional CLAC algorithm (ie, CLACslow, ≥180 s wait time between adjustments). Only if both requirements are simultaneously fulfilled, we would recommend using the revised algorithm.
Methods
Closed-loop automatic oxygen control
The algorithm and software solutions of CLAC as well as clinical validation data have been presented previously.8 9 11 In short, the algorithm uses a time-oriented data abstraction method to reduce fluctuations in SpO2 by adjusting FiO2 appropriately. The original CLAC algorithm (ie, CLACslow) with its 180 s wait time allowed for a maximum of 20 automated adjustments/hour. The new algorithm (ie, CLACfast) had a 30 s interval between two adjustments, allowing up to 120 automated adjustments/hour. Regarding all other features, both CLAC versions were identical. Since 2014, CLAC is implemented in a commercially available neonatal ventilator (ie, Leoni plus; Löwenstein Medical GmbH; Bad Ems, Germany) together with an on-board oximeter (ie, Masimo; Irvine, California, USA), which was used in this study.
Setting
The study was conducted at two German tertiary neonatal intensive care units (NICUs; University Children’s Hospital Tuebingen (centre 1) and University Medical Centre of the Johannes Gutenberg-University Mainz (centre 2)). Whereas centre 1 used a uniform SpO2 target range of 90%–95%, centre 2 used individualised SpO2 target ranges depending on the severity of apnoea of prematurity with a higher upper limit for more severe manifestations (85%–93% or 85%–96% SpO2, respectively). Nurse-to-patient ratios were 1:1 or 1:2 in both centres during the study.
Study design
A two-centre randomised, controlled crossover study was performed and registered at www.clinicaltrials.gov (NCT03163108). Each institutional review board approved the study (470/2016BO1 and 837.126.17). Written informed parental consent was obtained for each participant. Infants underwent three different modes of FiO2-control (ie, RMConly, RMC supported by CLACslow or by CLACfast) in random order for 8 hours each resulting in six different intervention sequences. Neither a run-in nor a wash-out period was used. A computer-generated list of random numbers using a block size of six was used for the allocation sequence. This list was prepared by a member of the Centre for Paediatric Clinical Studies Tuebingen, who was not involved in patient care or recruitment. After recruitment, infants were randomly assigned to one out of six intervention sequences by opening a sequentially numbered and sealed opaque envelope.
Patients
Preterm infants ≤34 weeks of gestation, on supplemental oxygen (baseline FiO2 >0.21) and invasive or non-invasive respiratory support, and >2 hypoxaemic events with SpO2 <80% within 8 hours prior to inclusion, were eligible for the study. Exclusion criteria were withdrawal of parental consent, congenital pulmonary anomalies and marked changes in the clinical condition of patients not allowing a further study participation. Patient recruitment took place between February and December 2017. Patients with no data or with low signal IQ data for >20% of the study period were excluded from analysis.
Protocol
Eight-hour periods with RMConly were compared with 8-hour periods of RMC supported by CLACslow and CLACfast, respectively. During the study, the nurse on duty remained fully responsible for oxygen administration. Nurses were encouraged to adjust the FiO2 according to the readings of the standard patient monitor (centre 1: Philips IntelliVue MP80, Philips, Eindhoven, Netherlands, with Masimo pulse oximetry module, 8 s averaging, 10 s alarm delay for SpO2 <90% and no alarm delay for SpO2 <80%; centre 2: Philips Intellivue MP70 with Philips FAST pulse oximetry, 10 s averaging time and 10 s default alarm delay).
Alarms of the ventilator’s oximeter were muted but its display not shielded. Thus, personnel were not blinded to the SpO2 data obtained by the ventilator’s oximeter. The local oxygen administration policy was not further specified for the present study. To comply with routine conditions in participating study centres, we allowed centre-specific and patient-specific SpO2 target ranges. Changes in ventilator settings and body position, as well as routine nursing procedures, remained unchanged.
Data acquisition
Data acquisition and processing was similar to our previous study.6 In short, SpO2, pulse rate, perfusion index, signal IQ and FiO2 were continuously recorded without missing values by the ventilator’s data logger with an averaging time of 2 s and a sampling rate of 30/min. At study termination, data were visualised and processed by one of the investigators (AS) using purpose-written data evaluation and plotting software.
Periods with low signal IQ concerning SpO2 data were excluded from analysis, because these data are likely inaccurate due to motion, perfusion or sensor-off artefacts.10 During such periods and because of safety aspects, the controller suspended further FiO2 adjustments. After signal IQ recovery, the controller resumed adjusting the FiO2. Hence, these periods could not be used for FiO2 control or SpO2 analysis.
In a first step, SpO2 values were automatically qualified by the data evaluation software as time periods ‘above target’, ‘within target’ or ‘below target’ according to the individual target range. In the case of room air breathing (ie, FiO2=0.21), all ‘above target’ periods were requalified as ‘within target’ periods, because FiO2 <0.21 was technically not possible with the ventilator.
Primary outcome and sample size calculation
Sample size calculation was based on our previous study6 assuming no carryover effects. The primary outcome was Target%, the proportion of time with: (1) SpO2 within target range, if infants required supplemental oxygen or (2) SpO2 within or above target range, if infants required no supplemental oxygen. Assuming a baseline mean±SD of 60%±15%, a normal distribution and an increase in Target% to 70±15% to be clinically relevant led to a standardised effect size of 0.666. An assumed correlation coefficient of 0.6 between treatment and control period further increased the standardised effect size to 0.745. A power of 90%, a type 2 error of 5% and a one-sided paired t-test yielded a minimum sample size of 17 infants. Based on the study design with six possible intervention sequences and the goal of a balanced allocation (ie, three infants per sequence), the targeted sample size was set to 18.
We planned to sequentially test the hypothesis of CLACfast being superior to RMConly and, if it were confirmed at the one-sided level of 0.05, to test for CLACfast being non-inferior to CLACslow also at the one-sided level of 0.05. We used a non-inferiority margin of 5 percentage points on the scale of the primary outcome variable Target%. The power for confirming the second hypothesis was 88%, if CLACfast was in fact superior to CLACslow by 5 percentage points.
Secondary outcomes
Secondary outcomes comprised indicators of hypoxaemia, hyperoxaemia and staff workload. Some definitions were changed after study registration due to individualised SpO2 target ranges across centres. We defined Above% as percentage of time with SpO2 >target range, if FiO2 was >0.21, and Below% as percentage of time with SpO2 <target range. Hypoxaemia was defined as SpO2 <80% and the rate (in counts per hour) and length of hypoxaemic episodes ≥60 s evaluated. For the latter analysis, 16 s averaging time was used to comply with previous work.2 Staff workload was assessed as the rate (in adjustments per hour) of manual FiO2 adjustments.
Statistical analysis
Descriptive statistics (N and percentage as well as median, minimum and maximum) were used to summarise demographic and clinical characteristics, as well as primary and secondary outcomes.
As outlined in the Introduction, the revised algorithm would be recommended only if it is: (1) superior to RMConly and (2) not inferior to the conventional algorithm. Accordingly, confirmatory analysis consisted of a hierarchical testing procedure involving two one-sided tests, one for superiority and one for non-inferiority. Based on our previous studies, where CLACslow was repetitively found to be superior to RMConly regarding Target%, the null hypothesis for testing superiority was that Target% during CLACfast is lower or equal compared with RMConly. Because of this expected direction of the effect, a one-sided test for superiority was chosen. Only if that null hypothesis was rejected, we were to prove that CLACfast was not inferior to the conventional CLACslow algorithm with a margin of 5 percentage points. Target% (null hypothesis for testing non-inferiority: Target% during CLACfast is 5 or more percentage points lower compared with CLACslow). Due to the expected direction of the effect, a one-sided test for non-inferiority was performed. As Target% was normally distributed in our sample, comparisons between CLACfast and the other treatment modalities in terms of means of Target% were performed by fitting a linear mixed regression model with the factors patient (random effects), period and treatment (fixed effects). For this confirmatory analysis, one-sided p values of <0.05 were considered statistically significant, and the corresponding point estimates were reported with 90% CIs. Carryover effects were evaluated by including the interaction term treatment × period.
For the exploratory analysis of secondary outcomes, the same regression model as mentioned above was used for global testing across treatment modalities. If adequate, post hoc pairwise comparisons were additionally performed using non-parametric, two-tailed Wilcoxon’s signed-rank test for the outcomes rate and duration of severe hypoxaemic episodes and rate of manual adjustments. For this exploratory analysis, treatment effects were given with 95% CIs, two-sided p values presented for descriptive purpose and corrections for multiple testing not performed.
All analyses were performed with statistical software (SAS/STAT V.14.3 and IBM SPSS Statistics V.24).
Results
Parents of 31 infants were approached, and 23 infants finally enrolled and randomised (figure 1). In centre 1, the study was stopped in two infants due to marked changes in their clinical condition (no longer needing supplemental oxygen: n=1; severe sepsis with pulmonary failure: n=1). In centre 2, two infants were later excluded because of technical problems with the data logger resulting in complete loss of data. The remaining 19 infants were included in the final analysis, 13 from centre 1 (all with SpO2 target range 90%–95%) and 6 from centre 2 (one with SpO2 target range 85%–93% and five with SpO2 target range 85%–96%). The allocation was balanced across intervention sequences except for the sequence CLACslow–RMConly–CLACfast to which four (instead of three) infants were allocated. Demographic and clinical characteristics of analysed patients are given in table 1.
Demographic and clinical characteristics (n=19)
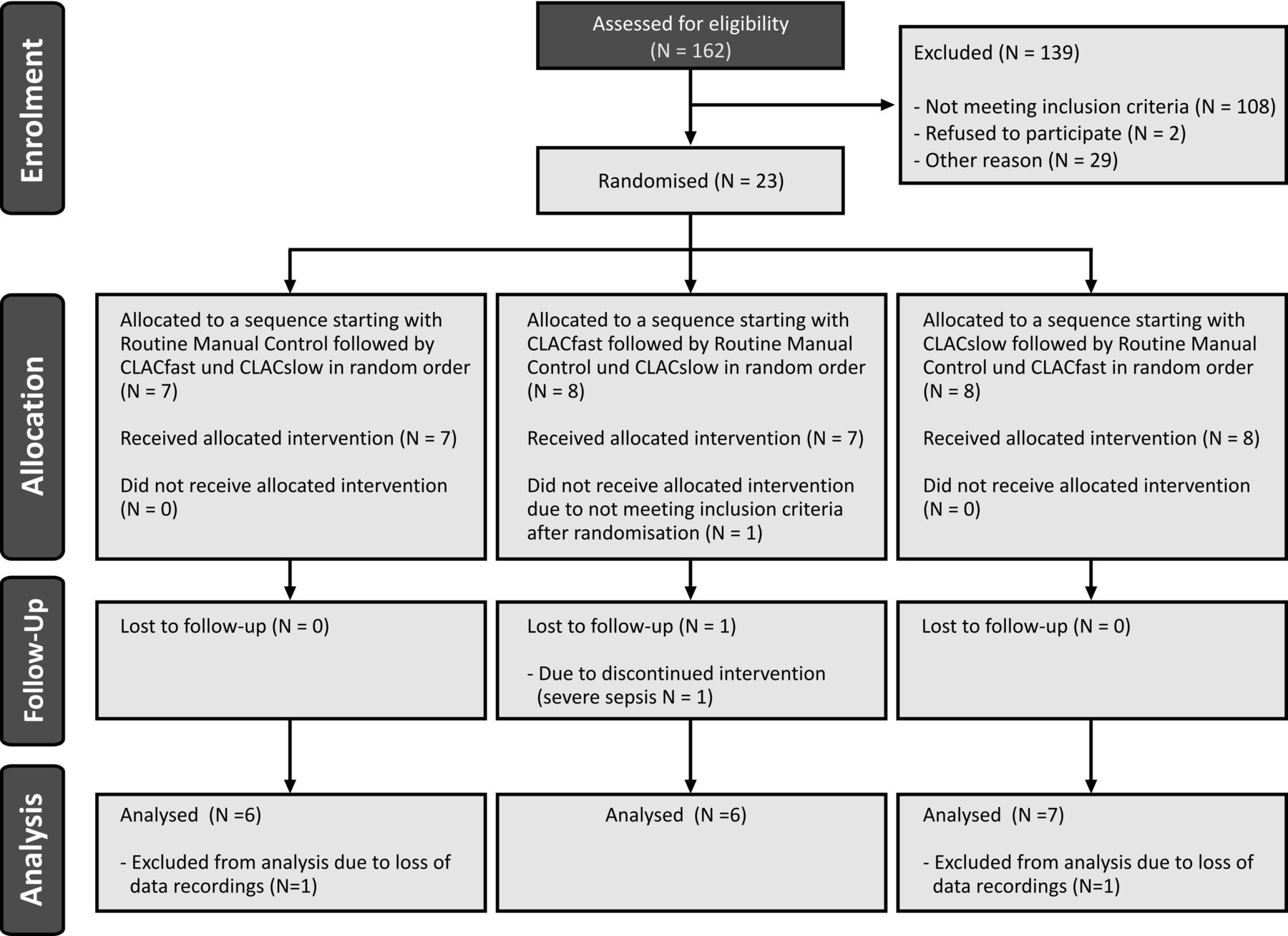
Modified CONSORT flow chart. CLAC, closed-loop automatic control.
The CLAC system performed as expected throughout and all infants tolerated the study procedures well. There were no study interruptions or early terminations related to failures of the CLAC system. By design, CLACfast executed more FiO2 adjustments than CLACslow (mean±SD: 39±13 vs 3±2 per hour).
Results for the primary and secondary outcomes are summarised in table 2. Results of Target% are presented in figure 2. The estimated treatment effect (90% CI; 95% CI) of CLACfast compared with RMConly was an increase by 9.5 percentage points in Target% (5.6, to 13.5; 4.8 to 14.3). CLACfast compared with CLACslow showed a treatment effect of 3.4 percentage points in Target% (−0.6 to 7.3; −1.3 to 8.1). The comparison of CLACslow with RMConly revealed a treatment effect of 6.2 percentage points Target% [95% CI 1.5 to 10.9] (see online supplementary figure 1S). The prespecified hypothesis tests of: (1) superiority of CLACfast versus RMConly and (2) non-inferiority of CLACfast versus CLACslow each yielded one-sided p values of <0.001. The test for treatment by period interaction did not give an indication of carryover effects (p=0.51, 4 degress of freedom).
Supplemental material
Results for primary and secondary study variables (n=19)

{kind=link}
{kind=link}
Primary outcome Target%. Box-and-whisker plot of the primary outcome variable: percentage of time spent within the SpO2 target range (Target%). Comparisons between RMConly and RMC supported by CLACfast or CLACslow, respectively. *CLACfast versus RMConly tested for superiority: one-sided p=0.0001; ** CLACfast versus CLACslow tested for non-inferiority (margin 5%): one-sided p=0.0005. CLAC, closed-loop automatic control; RMC, routine manual control.
Individual comparisons of Target% are given in online supplementary figure 2S and table 1S. Target% was higher in CLACfast compared with RMConly in 16 of 19 infants. Target% was higher during CLACfast compared with CLACslow in 11 of 19 infants, while Target% was highest in either CLAC mode compared with RMConly in 17 of 19 infants.
Supplemental material
Supplemental material
The model-based adjusted means (±SE) for Target% during RMConly, CLACfast and CLACslow were 54.1±2.8, 64.2±2.8 and 62.2±2.8 in centre 1 (n=13) and 67.7±4.1, 76.0±4.2 and 70.4±4.1 in centre 2 (n=6). The test for interaction of treatment by centre did not give an indication for a centre effect (p=0.61).
We found a significant reduction in Below% in CLACfast compared with RMConly (14%±5% vs 22±11%; p<0.001). In contrast, all other secondary outcomes did not differ significantly across treatment modalities (table 2). Individual comparisons of Above% and Below% are given in online supplementary figure 3S, 4S and table 1S. Of note, there was no significant reduction in the number of manual FiO2 adjustments.
Supplemental material
Supplemental material
The analysis of severe hypoxaemic episodes revealed that these had only occurred in 15 out of 19 infants (see table 2). Nine infants had at least one episode during each mode of FiO2 control, two patients only during RMConly, one patient only during CLACslow and no patient only during CLACfast.
Discussion
In this two-centre, randomised controlled, crossover study, a revised and accelerated CLAC algorithm significantly increased the proportion of time with SpO2 levels within predefined target ranges when compared with routine manual adjustments only. In a sample of clinically stable infants mostly receiving non-invasive ventilatory support, this algorithm was not inferior to a previously tested CLAC algorithm. Moreover, concerning the time below target range, the faster algorithm outperformed the conventional one, suggesting that the reduction in ‘wait time’ to 30 s (allowing a higher frequency of FiO2 adjustments) was safe and more effective in most infants. An accelerated algorithm may better meet expectations of NICU staff and enhance acceptance of the CLAC system. However, results may be not applicable to critically ill infants on invasive respiratory support.
We found the treatment effect of CLAC within the current study comparable with our previous studies,6 11 those from other groups12–14 and a recent meta-analysis.15 The latter reported an 8.9% improvement in time spent in target saturation range in the automated control group after removing non-randomised studies in a sensitivity analysis. In this analysis, the results were considerably consistent (I2=0) and the pooled effect remained significant. Study design, but not type of algorithm, turned out to explain the variation in effect size.15 All these data indicate the potential of automatic oxygen control to better meet the supplemental oxygen needs of preterm infants. It can also support NICU staff in their attempts to reduce oxygen exposure as much as possible and to prevent hypoxaemic and hyperoxaemic episodes, which are potentially related to adverse clinical outcomes.2–4
Our initial concern that fast FiO2 responses to SpO2 changes result in more episodes of hypoxaemia and/or hyperoxaemia was not confirmed in our study. Sadeghi Fathabadi et al 16 found a median delay in first order responses in SpO2 following FiO2 increments or decrements of 22 s and 40 s, respectively, which virtually fits our present waiting time of 30 s. However, some SpO2 responses to an FiO2 change occur after this wait time, which may increase the risk of hypoxaemia or hyperoxaemia. In our study, Target% was distinctly higher during CLACslow compared with CLACfast in five patients (see online supplementary figure 2S). Thus, it may be of benefit to extend the wait time in some patients. However, appropriate patient-related criteria for setting the wait time are not known yet.
Strengths of our study include that the device was tested under routine conditions, in two different NICUs and for 8 hours each. Oxygen control was maintained by clinical staff throughout, different ventilation modes were allowed and the centre-specific SpO2 target range was not influenced by the study protocol; thus, the RMC results reflect a real-world scenario. The higher proportion of infants on CPAP, compared with our previous multicentre study,6 may reflect ongoing changes in neonatal care towards an increased use of non-invasive respiratory support.
Limitations
CLAC was not part of standard care in the participating NICUs, and the ventilator’s oximeter display was not shielded. Staff was advised to adjust the FiO2 according to the SpO2 readings of the standard patient monitor and not according to the ventilator’s oximeter. Due to the nature of the intervention, NICU personnel could not be blinded to the actual FiO2 control mode. All these factors could have influenced staff awareness, thoroughness and performance during both, RMConly and CLAC periods. For example, we occasionally observed that during RMConly periods, some nurses were motivated to ‘beat’ the controller, while during CLAC periods, some nurses gave more attention to non-CLAC-cared patients. Both may have led to improved RMConly and impaired CLAC results, leading to an underestimation of the true intervention effect. Moreover, the treatment effect of the revised algorithm could also be underestimated due to the high 1:1 or 1:2 nurse-to-patient ratios applied in participating NICUs.17 Besides other centre-specific factors like the SpO2 target range or structural conditions (eg, short distances between nurses and patients), the nurse-to-patient ratio may influence the effectiveness of automatic oxygen control and limit generalisability of results.6
Conclusions
Automatic oxygen control performed by a new CLAC algorithm improved oxygen therapy in preterm infants on non-invasive respiratory support. Allowing for up to 2 FiO2 adjustments/min appeared safe and effective. Results, however, may not be applicable to critically ill infants on invasive respiratory support. Whether it ultimately results in better patient outcomes and/or staff satisfaction requires further study.
Acknowledgments
We would like to thank the parents of our patients to take part in this study with their infants, the staff of the neonatal intensive care units in Mainz and Tuebingen to support this study and the Löwenstein Medical for supporting this study.
References
Footnotes
CES and AK contributed equally.
Contributors CES coordinated and supervised patient recruitment and data collection at the study centres, evaluated the analyses and drafted the initial and the revised manuscript; AK conducted patient recruitment and data collection, evaluated the analyses and reviewed the revised manuscript; NSB conducted patient recruitment and data collection and critically reviewed the manuscript; AF was involved in study design, supervised patient recruitment and data collection, evaluated the analyses and critically reviewed the manuscript; JK carried out the statistical analyses and critically reviewed and revised the manuscript; EM and CFP supervised the study design and critically reviewed the manuscript; AS designed and developed the closed-loop automatic control (CLAC) algorithm, analysed the biosignal data and critically reviewed the manuscript; MSU led the study team, received the research grant, conceptualised and designed the study, supervised the biosignal and statistical analyses and revised the draft of the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding This study was supported by a research grant from Löwenstein Medical (Bad Ems; Germany), which also provided two ventilators. The granting company had no impact on the study design, data acquisition and analysis and writing of the manuscript.
Competing interests The University of Tuebingen holds a patent on the CLAC algorithm for automated oxygen control and have a licencing agreement with Löwenstein Medical in relation to this algorithm. AF and CFP are supported by a grant of the German Ministry of Research and Education for conducting the FiO2 Controller study on medium-term effects of CLAC of FiO2. CES, AF and CFP also received a research grant from Fritz Stephan GmbH. CFP received speaker honoraria from Masimo Inc.
Patient consent for publication Not required.
Ethics approval Ethik-Kommission an der Medizinischen Fakultät der Eberhard-Karls-Universität und am Universitätsklinikum Tübingen 470/2016BO1 and Ethikkommission der Landesärztekammer Rheinland Pfalz 837.126.17 .
Provenance and peer review Not commissioned; internally peer reviewed.
Data availability statement Data are available on reasonable request.