Article Text

Abstract
Objective To describe the trend and risk factors for severe intraventricular haemorrhage (IVH) among infants <32 weeks gestation.
Design Population-based cohort study.
Setting Australia and New Zealand.
Patients All preterm infants <32 weeks gestation in the Australian and New Zealand Neonatal Network (ANZNN) from 1995 to 2012.
Interventions Comparison of IVH incidence between 6-year epochs.
Main outcome measures Overall IVH and severe IVH incidence.
Results A total of 60 068 infants were included, and overall survival to discharge increased from 89% to 93% over the three epochs. As the percentage of infants with IVH decreased from 23.6% to 21.3% and 21.4% (p<0.001) from epoch 1 to 3, respectively, fewer survivors had severe IVH (4.0%, 3.3% and 2.8%, respectively, p<0.001). Over time, there were fewer antenatal complications, higher antenatal steroid usage and more caesarean-section births. Fewer infants were intubated at birth, had low 5 min Apgar score, had sepsis or pneumothorax needing drainage. Adjusted for perinatal confounders, there was significant reduction in odds of severe IVH from epoch 1 to 3 (adjusted OR (AOR) 0.8, 95% CI 0.7 to 0.9). Factors associated with development of severe IVH include no antenatal steroids (AOR 1.7, 95% CI 1.5 to 1.9), male (AOR 1.3, 95% CI 1.2 to 1.4), 5 min Apgar score <7 (AOR 2.0, 95% CI 1.9 to 2.2), intubated at birth (AOR 2.0, 95% CI 1.8 to 2.2), extremely low gestational age (AOR 4.0, 95% CI 3.7 to 4.4), outborn (AOR 1.6, 95% CI 1.5 to 1.8) and vaginal delivery (AOR 1.4, 95% CI 1.3 to 1.6).
Conclusions Along with increased survival among infants born <32 weeks gestation, the incidence of severe IVH has decreased over the 18 years, especially in the most recent period. This coincided with reduction in rates of risk factors for severe IVH development.
- epidemiology
- neonatology
Statistics from Altmetric.com
What is known on this topic?
Reports on intraventricular haemorrhage (IVH) rates have described a decreasing trend in infants born <32 weeks gestation, from 40%–50% in 1980s to 15%–20% in early 2000s.
The incidence of severe IVH has reportedly been stagnant over the past two decades.
What this study adds?
Along with improved survival among infants born <32 weeks gestation, rates of survival without severe IVH have increased over the study period.
In addition to known risk factors for severe IVH, caesarean-section births and outborn were associated with increased risk.
Introduction
Intraventricular haemorrhage (IVH) is a common intracranial complication of extreme prematurity and is reportedly present in up to one-third of all infants born <28 weeks gestation.1 2 IVH occurs within the fragile germinal matrix, which is a source of neuronal cells for the developing premature brain. The presence of severe IVH (grade 3 or 4) has been strongly associated with adverse long-term neurodevelopmental outcomes.3 The implications of low-grade IVH (grade 1 or 2) have been unclear with differing conclusions from several reports.4 5
Reports on IVH trends have revealed an overall decreasing incidence in preterm infants <32 weeks gestation, from around 40%–50% in the 1980s to 15%–20% in the early 2000s.6–8 This improvement correlated with decreases in severe IVH from 10%–15% to 4%–8%.1 9 10 However, the initial reduction in the severe IVH incidence has been reportedly stagnant over the past two decades.11 In this study, we aim to investigate the trends of IVH and severe IVH among infants <32 weeks gestation over 18 years (1995–2012) in Australia and New Zealand. We hypothesise that with improvement in the survival of very preterm infants, there has been an increase in survival without severe IVH in tertiary-level neonatal intensive care units (NICUs) in this setting.
Methods
Data source
This is a retrospective cohort study using data from the Australian and New Zealand Neonatal Network (ANZNN) of all preterm infants born at <32 weeks gestation admitted to a collaborating NICU from 1 January 1995 to 31 December 2012. ANZNN is a collaborative network of all 29 tertiary-level NICUs in Australia and New Zealand. The network monitors the care of high-risk newborns by pooling data of all infants admitted to tertiary-level NICUs during the neonatal period (≤28 days) for any of the following indications: gestational age of <32 weeks, birth weight <1500 g, need for assisted ventilation for ≥4 hours, major surgery and therapeutic hypothermia. Care of extremely preterm infants has been regionalised since the early 1990s, where preterm infants who are offered intensive care will be cared for in a tertiary-level NICU. The ANZNN contains 99% of all live births<29 weeks in both countries. Each NICU has an audit officer who collects and checks the data before submission into a central database, located at the University of New South Wales, Australia. Accuracy of the data collection is validated by data crosschecking by ANZNN data managers.
Variables and definitions
Variables were defined according to the ANZNN data dictionary (https://www.anznn.net/dataresources/datadictionaries). Gestational age is defined as the best obstetric estimate of completed weeks based on obstetric history, clinical examination and prenatal ultrasound. Assisted conception is classified as the use of fertility treatments including hormonal therapy, artificial insemination or in vitro fertilisation. An infant is small for gestational age (SGA), if the birth weight is <3rd centile according to published Australian norms.12 Outborn infants refer to those who were delivered in a non-tertiary-level NICU.
The primary and secondary outcome of interest are the incidence of severe IVH and the combined outcome of severe IVH and/or death over time. The classification of IVH is as defined by Papile et al.13 The maximum IVH grade is recorded from ultrasounds performed within the first 10 days of life. Grade 1 and 2 IVH were classified as low grade, whereas grade 3 and 4 as severe IVH. Mortality and major morbidity are limited to events occurring before initial NICU discharge. Major morbidities included the presence of bronchopulmonary dysplasia (BPD),14 severe IVH, cerebral cysts, medically or surgically treated necrotising enterocolitis (NEC) and grade 3 or 4 retinopathy of prematurity (ROP).15 Sepsis is defined as a clinical picture consistent with early onset and/or late-onset sepsis, and either a positive bacterial or fungal culture of blood and/or cerebrospinal fluid, or a positive urine culture by sterile collection only.
Statistical analysis
Analysis was performed for the whole population and also stratified by three 6-year epochs (epoch 1: 1995–2000, epoch 2: 2001–2006, epoch 3: 2007–2012). We compared the outcomes using Χ² test for proportions and t-test for means, as appropriate. Infants who did not receive head ultrasound scans were excluded from IVH-specific analysis. Variables associated with IVH were analysed by epoch and the association was determined by multivariable logistic regression models to estimate the adjusted OR (AOR) of the outcomes–severe IVH and the combined severe IVH and/or death.
The following clinical variables were included in the multivariable analysis on the development of severe IVH: receipt of antenatal steroids, male gender, 5 min Apgar score <7, intubation at birth, gestational age ≤27 weeks, outborn status, pregnancy-induced hypertension (PIH) and method of delivery. Multivariable analysis for the combined outcome of severe IVH and/or death included: receipt of antenatal steroids, male gender, 5 min Apgar score <7, intubation at birth, gestational age ≤27 weeks, outborn status, PIH, SGA and method of delivery. OR and AOR were expressed with 95% CI. A level of significance of α <0.05 using a two-tailed comparison was used. Statistical analyses were performed using IBM SPSS Statistics V.22.0 (IBM, Armonk, New York, USA).
Results
Maternal and infant characteristics
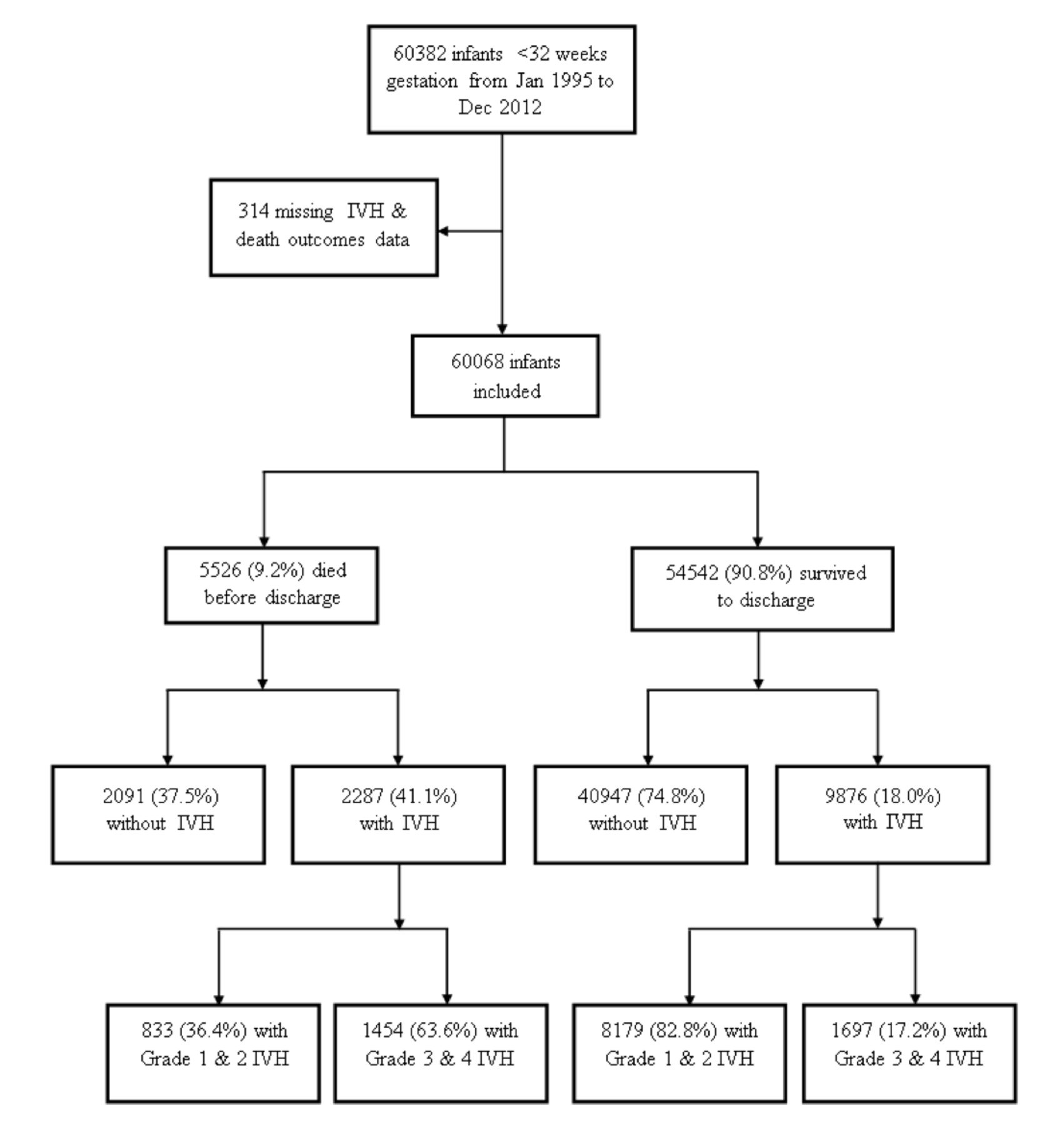
A total of 60 068 infants born <32 weeks gestation was included (figure 1). Of these, 18 316 infants were born in epoch 1, 20 146 in epoch 2 and 21 606 in epoch 3. The proportion of Asian and Indigenous (Aboriginal, Torres Strait Islander descent, Pacific Islander or Maori) mothers in this cohort increased from epoch 1 to epoch 3: 5.3% to 9.0% and 10.6% to 12.6%, respectively (table 1). The mean maternal age also increased, from 28 to 30 years. The rate of births via assisted conception declined slightly (12.0% in epoch 1 to 11.3% in epoch 3), while the proportion of multiple gestation infants remained stable (27.2%–27.8%).
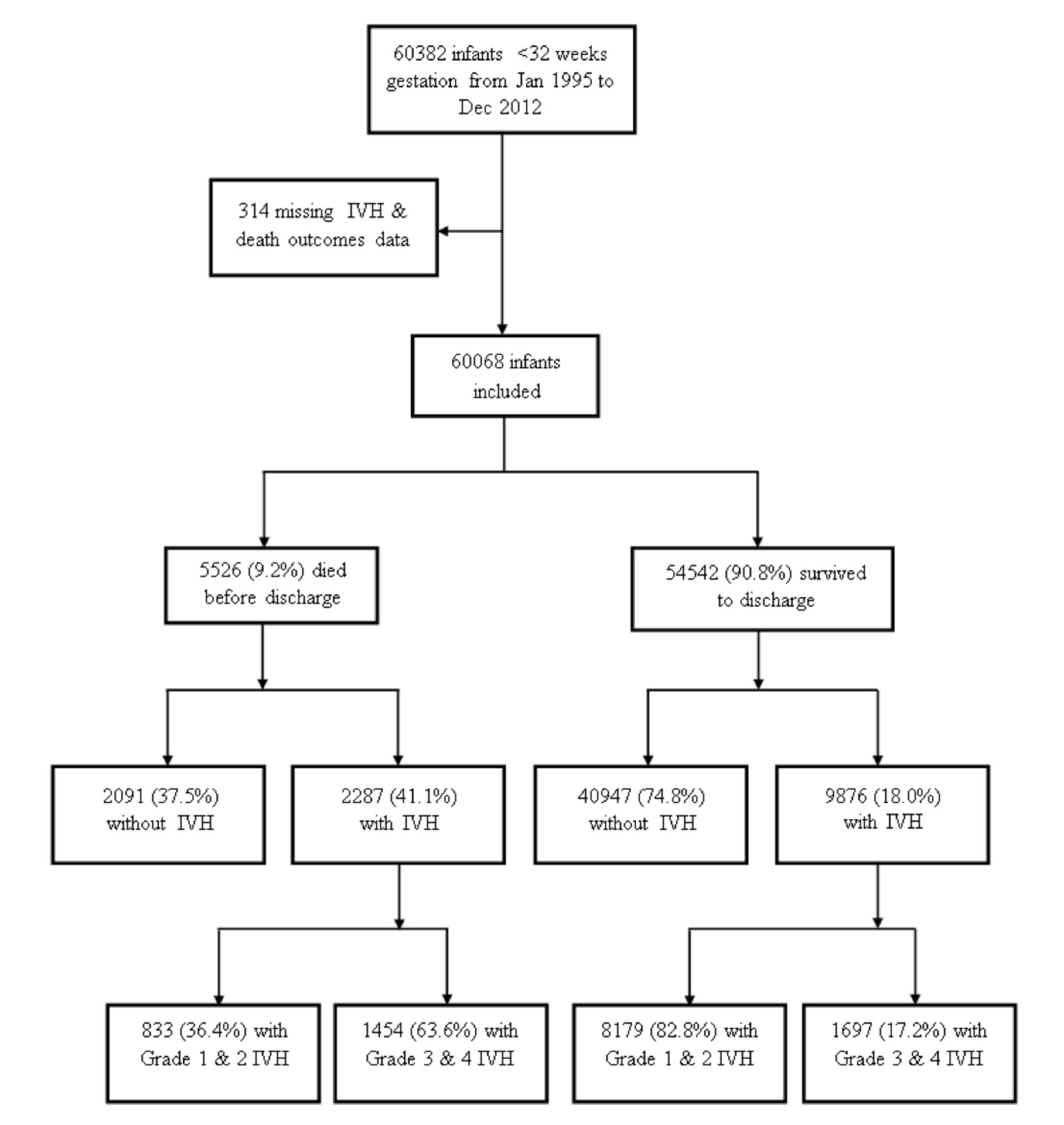
Distribution of different grades of IVH in very preterm infants <32 weeks gestation born in Australia and New Zealand from January 1995 to December 2012. IVH, intraventricular haemorrhage.
Clinical characteristics and outcomes as stratified by study epoch
From epoch 1 to 3, there was a decrease in the incidence of antenatal complications such as PIH (20.4%–15.0%) and antepartum haemorrhage (APH) (24.2%–21.5%) but an increase in prolonged rupture of membranes (PROM) (21.1%–23.7%). There was an increased trend for caesarean sections, specifically caesarean section without labour (32.5%–38.7%) (online supplemental figure 1). The mean gestational age for infants in this study was 28.4 weeks, slightly more than half were male (54.4%) and 28.3% were of multiple gestation births. Antenatal steroid usage increased from 82.6% to 89.4% from epoch 1 to epoch 3. Intubation rates at resuscitation decreased significantly from 51.3% to 40.1%, while rates of surfactant usage generally increased from 55.4% to 56.3%. The incidence of outborns also trended upwards, from 11.4% to 13.6% from epoch 1 to 3. Stratified by gestational age, outborn births have increased for infants of almost all gestational ages, ranging from 9.6% to 15.6% (online supplemental figure 2).
Supplemental material
The overall survival in this population was 91% over the study period, with a notable increase from 89.3% to 92.2% over the three epochs. The incidence of pneumothorax (4.7%–3.9%) and sepsis (28.2%–10.9%) has declined over the three epochs. The proportion of infants with one or more major morbidity was 24.3%.
IVH trends and comparisons
There were 12 163 (20.2%) infants with IVH—9012 (15%) with low-grade IVH and 3151 (5.2%) with severe IVH (online supplemental table 1). The proportion of infants with IVH of any grade were 23.6%, 21.3% and 21.4% from epoch 1 to 3, respectively. Infants with severe IVH decreased from 6.6%, 5.7% to 5.0%. Survival without severe IVH increased from 84.8% to 91.0% (figure 2). Among infants born ≤27 weeks gestation, those with any IVH decreased from 37.6% to 36.0% and 34.9% over the three epochs, respectively and severe IVH decreased from 14.0% to 13.0% and 11.6%. By comparison, IVH of any grade among infants born ≥28 weeks gestation decreased from 16.7% to 14.3% and 14.8% over the three epochs and severe IVH decreased from 2.9% to 2.1% and 1.8%, respectively. Of the 4867 (8.1%) infants who did not receive head ultrasounds, 1148 died before receiving a scan (23.6%) and 3580 (73.6%) infants were >28 weeks gestation at birth.
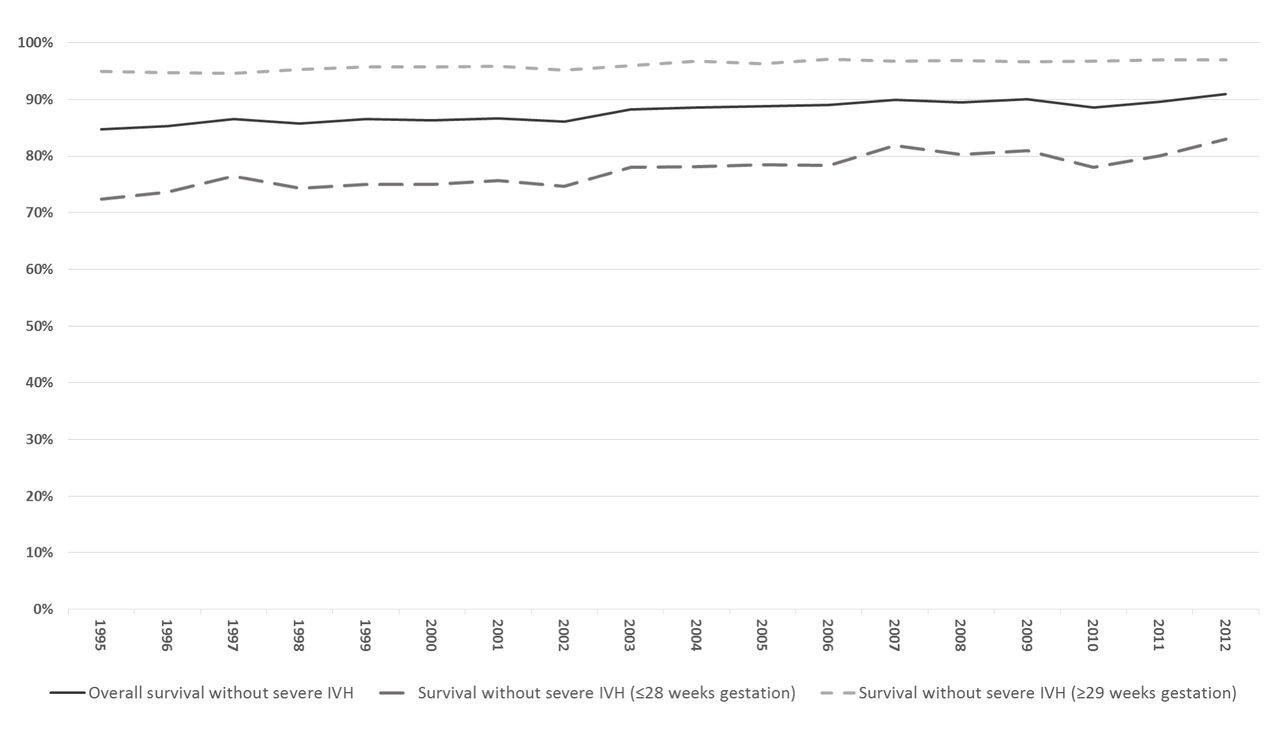
Trends of survival and survival without severe intraventricular haemorrhage (IVH) among survivors over the study period. Number of survivors by year: 1995—2476; 1996—2638; 1997—2578; 1998—2765; 1999—2896; 2000—3000; 2001—2949; 2002—2963; 2003—3004; 2004—2984; 2005—3123; 2006—3247; 2007—3285; 2008—3460; 2009—3356; 2010—3070; 2011—3304; 2012—3444.
Stratified by gestational age, the incidence of any IVH and severe IVH have generally declined from epoch 1 to 3 with the exceptions of those born at gestations ≤24 weeks (figure 3). The incidence of severe IVH increased from epoch 1 to 3 for infants ≤23 weeks. This is coincident with an increase in survival (online supplemental table 2) and a decrease in severe IVH and/or death for this gestational age group.

{kind=link}
{kind=link}
{kind=link}
Proportions of intraventricular haemorrhage (IVH) severity and/or mortality as stratified by epoch and gestational age. Proportion of infants with (A) varying IVH severity, (B) death and/or severe IVH, as stratified by epoch and gestational age.
Compared with infants without IVH, infants with IVH were more likely to be extremely low gestational age ≤27 weeks, male, born via vaginal delivery, outborn, have 5 min Apgar score <7 and require surfactant after birth (table 2). Infants with IVH were less likely to be part of a multiple gestation pregnancy, born to mother with PIH, to have received antenatal steroids and be SGA. Those with IVH were also twice as likely to have one or more major morbidity, and were more than four times less likely to survive. The incidence and risk of death and death and/or severe IVH were significantly higher for outborn infants compared with inborns (online supplemental figure 3). Compared with inborns, the odds of death and/or severe IVH for outborns from epoch 1 to 3 were 1.6 (95% CI 1.5 to 1.8), 1.7 (95% CI 1.5 to 1.9) and 1.6 (95% CI 1.4 to 1.8), respectively.
Comparison of clinical parameters between infants with and without IVH
Controlling for known confounders, infants with severe IVH were less likely to have received antenatal steroids (AOR 1.7, 95% CI 1.5 to 1.9), born to a mother with no PIH (AOR 1.3, 95% CI 1.1 to 1.4), be male (AOR 1.3, 95% CI 1.2 to 1.4), of low gestation ≤27 weeks (AOR 4.0, 95% CI 3.7 to 4.4), have 5 min Apgar score <7 (AOR 2.0, 95% CI 1.9 to 2.2), intubated at birth (AOR 2.0, 95% CI 1.8 to 2.2), be outborn (AOR 1.6, 95% CI 1.5 to 1.8), born via vaginal delivery (AOR 1.6, 95% CI 1.5 to 1.8) and born in the earlier epochs (online supplemental table 3). Similar risks factors, including SGA status at birth, were noted for infants with severe IVH and/or mortality (online supplemental table 4).
Discussion
In this population-based cohort study of infants <32 weeks gestation, 20.2% of infants had IVH and 5.2% had severe IVH. The improving adjusted risk for severe IVH and severe IVH and/or death was most significant in the recent epoch with reduction by 20% and 30%, respectively compared with epoch 1. Several multicentre US studies have reported decreasing and stagnating rates of severe IVH from 15%–19% in the early 1990s to 12%–13% from 2000 to 2012.11 16 A more recent cohort study from the California Perinatal Quality Care Collaborative reported significant decrease in severe IVH across California from 9.7% in 2005 to 5.9% in 2015.17 Several European studies have reported IVH trends similar to ours. The French EPIPAGE in 1997 reported the incidence of severe IVH to be about 6%.18 A recent report from 194 EuroNeoNet NICUs (2006–2012) described varying rates of severe IVH rates of 5%–14.5% from different European regions with a decreasing trend noted in Western European countries.19
Improvement in several factors associated with IVH development may have contributed to the decreasing incidence in our cohort. Over the study period, the coverage of antenatal steroids was generally high, up to 89% in these high-risk infants. We also found a significant decrease in intubation rates, which reflects the increasing primary usage of nasal continuous positive airway pressure in our setting.20 The increasing surfactant usage rates over the same period also suggests an increasing usage of early and less invasive means of surfactant provision in our setting.21 The decrease in rates of pneumothorax and sepsis over time may also have contributed to the decrease. We also noted decreases in the rates of antenatal complications such as PIH, APH and preterm labour in our cohort. The lower adjusted risk of severe IVH among infants born to mothers with PIH in our study have been demonstrated in several cohort studies.22–24 The mechanism behind this protective effect remains unclear, but it has been postulated to be related to angiogenic factors present in PIH, the effect of antihypertensives used and the obstetric management of this condition. Further studies are needed to investigate this association further and the potential biological pathways associated with it.
Risk factors associated with severe IVH in our population were extremely low gestational age, outborn, male, no antenatal steroids, vaginal births, intubation at birth and 5 min Apgar score <7. The protective effect of antenatal steroids has been well documented.25 Poor conditions at birth and the requirement for significant support at birth have been associated with development of IVH.17 26 Such infants may be more likely to be affected by physiological changes during resuscitation.27 Regionalisation of NICU care in Australia and New Zealand have led to prioritisation of in utero transfers for threatened preterm deliveries <32 weeks to tertiary hospital. Birth in non-tertiary neonatal centres and transport of these infant postbirth have been associated with significant risk of severe IVH and poor outcomes.28–31 The rates of death and IVH and/or death were consistently higher in those outborn across the three epochs in our study. Even after controlling for factors such as antenatal steroids, outborn infants were at 1.7 times increased risk for severe IVH. It is possible that less neonatal-experienced staff, excessive handling, difficulty with ventilation and temperature instability could lead to the increased risk. However, without further information on the clinical condition and initial management of these infants, we could not assess the exact mechanisms further.
There is conflicting evidence on the effect of the route of delivery on the risk of IVH in preterm infants.32–36 Compression of the fetal head during vaginal delivery is thought to increase central venous pressure in the preterm infant, leading to the development of IVH.37 38 Observational studies have predominantly shown no difference in the risk of IVH based on the route of delivery. In our study, there were more vaginal births in the group with IVH (54.7% vs 34.4%). The adjusted risk of severe IVH and severe IVH and/or death were also significantly lower in those born via caesarean section, especially in those without labour. Further studies detailing the indications and care surrounding caesarean section and the subsequent development of IVH are needed.
One of the potential limitations of this study is the interobserver reliability issues as a result of differing techniques and grading of ultrasound scans, especially involving lower IVH grades. A previous US National Institute of Child Health and Human Development (NICHD) study reported 48%–68% agreement for reporting of low-grade IVH.39 A study from ANZNN investigated the variation in interpretation of head ultrasounds of preterm infants,40 and showed a high-level agreement between the reviewers and the submitted reports (κ statistics=0.75–0.91). Even so, grade 1 IVH was generally over-reported and grade 4 under-reported.
Our current study did not evaluate the effects of other recognised risk factors for IVH including the presence and timing of interventions for hypotension and variations in ventilation strategies or changes in carbon dioxide. A total of 3719 (6.2%) surviving infants did not receive a head ultrasound scan and were excluded from the IVH-specific analysis. Of these, 3580 were >28 weeks gestation and were of low risk for severe IVH. However, this is a potential source of bias and may have underestimated the IVH rate.
Conclusion
Along with improvements in survival among infants born <32 weeks gestation, the incidence of severe IVH has decreased over the 18 years, especially in the most recent time period. This has coincided with reduction in rates of maternal, perinatal and neonatal risk factors for the development of severe IVH.
References
Footnotes
Contributors KTY, RT, KL were involved in the conception and design of the work; acquisition, analysis and interpretation of the data for the manuscript and initial drafting of the manuscript. They had full access to all data in the study. KTY had the final responsibility for submission for publication. SC was involved in the acquisition, analysis and interpretation of the data for the work. SB, RH, WT-M were involved in the interpretation of the data for the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Ethics approval The South Eastern Sydney Local Health District Human Research Ethics Committee approved this study (HREC ref: 14/208).
Provenance and peer review Not commissioned; externally peer reviewed.
Collaborators Advisory Council Members of ANZNN (*denotes ANZNN Executive) Australia: Peter Marshall (Flinders Medical Centre, SA), Peter Schmidt (Gold Coast University Hospital, QLD), Paul Craven, Koert de Waal* (John Hunter Children’s Hospital, NSW), Karen Simmer, Andy Gill*, Jane Pillow* (King Edward Memorial and Princess Margaret Hospitals, WA), Jacqueline Stack (Liverpool Hospital, NSW), Pita Birch (Mater Mother’s Hospital, QLD), Dan Casalaz, Jim Holberton* (Mercy Hospital for Women, VIC), Alice Stewart (Monash Medical Centre, VIC), Lucy Cooke* (Neonatal Retrieval Emergency Service Southern Queensland, QLD), Lyn Downe (Nepean Hospital, NSW), Michael Stewart (Paediatric Infant Perinatal Emergency Retrieval, VIC), Andrew Berry (NSW Newborn & paediatric Emergency Transport Service), Rod Hunt (Royal Children’s Hospital, VIC), Charles Kilburn (Royal Darwin Hospital, NT), Tony De Paoli (Royal Hobart Hospital, TAS), Kei Lui* (Royal Hospital for Women, NSW), Mary Paradisis (Royal North Shore Hospital, NSW), Ingrid Rieger, (Royal Prince Alfred Hospital, NSW), Pieter Koorts (Royal Women’s Hospital, QLD), Carl Kuschel, Lex Doyle, (Royal Women’s Hospital, VIC), Andrew Numa (Sydney Children’s Hospital, NSW), Hazel Carlisle (The Canberra Hospital, ACT), Nadia Badawi, Christine Jorgensen* (The Children’s Hospital at Westmead, NSW), Guan Koh (The Townsville Hospital, QLD), Jonathan Davis (Western Australia Neonatal Transport Service), Melissa Luig (Westmead Hospital, NSW), Chad Andersen (Women’s & Children’s Hospital, SA). New Zealand: Adrienne Lynn (Christchurch Women’s Hospital), Brian Darlow (Christchurch School of Medicine), Liza Edmonds (Dunedin Hospital), Lindsay Mildenhall (Middlemore Hospital), Mariam Buksh, Malcolm Battin* (Auckland City Hospital), David Bourchier (Waikato Hospital), Vaughan Richardson, Fiona Dineen* (Wellington Women’s Hospital). ANZNN Executive not members of hospitals contributing data: Georgina Chambers* (National Perinatal Statistics and Epidemiology Unit, University of New South Wales); Victor Samuel Rajadurai* (KK Women’s and Children’s Hospital, Singapore); Barbara Bajuk* (NSW Pregnancy and Newborn Services Network), Jutta van den Boom* (Waitemata DHB).
Patient consent for publication Not required.