Article Text

Abstract
Objective To compare a low versus a higher threshold for intervention in preterm infants with posthaemorrhagic ventricular dilatation.
Design Multicentre randomised controlled trial (ISRCTN43171322).
Setting 14 neonatal intensive care units in six countries.
Patients 126 preterm infants ≤34 weeks gestation with ventricular dilatation after grade III–IV haemorrhage were randomised to low threshold (LT) (ventricular index (VI) >p97 and anterior horn width (AHW) >6 mm) or higher threshold (HT) (VI>p97+4 mm and AHW >10 mm).
Intervention Cerebrospinal fluid tapping by lumbar punctures (LPs) (max 3), followed by taps from a ventricular reservoir, to reduce VI, and eventually a ventriculoperitoneal (VP) shunt if stabilisation of the VI below the p97+4 mm did not occur.
Composite main outcome measure VP shunt or death.
Results 19 of 64 (30%) LT infants and 23 of 62 (37%) HT infants were shunted or died (P=0.45). A VP shunt was inserted in 12/64 (19%) in the LT and 14/62 (23%) infants in the HT group. 7/12 (58%) LT infants and 1/14 (7%) HT infants required shunt revision (P<0.01). 62 of 64 (97%) LT infants and 36 of 62 (58%) HT infants had LPs (P<0.001). Reservoirs were inserted in 40 of 64 (62%) LT infants and 27 of 62 (43%) HT infants (P<0.05).
Conclusions There was no significant difference in the primary composite outcome of VP shunt placement or death in infants with posthaemorrhagic ventricular dilatation who were treated at a lower versus a higher threshold for intervention. Infants treated at the lower threshold received more invasive procedures. Assessment of neurodevelopmental outcomes will provide further important information in assessing the risks and benefits of the two treatment approaches.
- imaging
- neonatology
- preterm
- post haemorrhagic ventricular dilatation
- intraventricular haemorrhage
Statistics from Altmetric.com
What is already known on this topic?
Posthaemorrhagic ventricular dilatation (PHVD) most likely to occur in infants with a grade III or IV haemorrhage.
A ventriculoperitoneal (VP) shunt rate has been reported to be 35%–60% in infants who need intervention for PHVD.
What this study adds?
Intervention using lumbar punctures and/or taps from a ventricular reservoir just after the ventricular index crossed the p97+4 mm line results in the lowest VP shunt rate reported so far and was associated with fewer invasive procedures than earlier intervention.
Risk of infection following taps from a ventricular reservoir in this multicentre study was not increased compared with our single-centre study.
Introduction
Although the incidence of germinal matrix-intraventricular haemorrhage (GMH-IVH) in very low birthweight infants decreased in the 90s, there has been no further decrease over the last decade. Infants with grade III and IV haemorrhage,1 especially those who develop posthaemorrhagic ventricular dilatation (PHVD), are at increased risk of developing neurological sequelae. PHVD occurs in about 30%–50% of infants with a severe GMH-IVH and there is an ongoing discussion about the best time to intervene.2–4 Due to the high water content of the immature white matter and the large extracerebral space in extremely preterm infants, symptoms and signs of raised intracranial pressure develop several weeks following the onset of PHVD. This allows a considerable increase in ventricular size without affecting fontanelle pressure or head circumference.5
In infants with progressive PHVD, deterioration of electroencephalography (EEG) background activity, increased latency of evoked potentials, increasing Doppler Resistance Index and decreasing cerebral oxygenation have been reported,6–11 all showing improvement within a week following neurosurgical intervention.
Cranial ultrasound (cUS) is used to follow the progress of PHVD and the ‘ventricular index’ (VI) is most often used.12 Most intervention studies have taken the 97th centile (p97)+4 mm as a starting point for randomisation.13–15 Other useful measures are the anterior horn width (AHW) and thalamo-occipital distance (TOD).16 17
In previous retrospective studies, very early intervention, prior to development of clinical symptoms and prior to severe dilatation of the lateral ventricles, was associated with a reduced need for a ventriculoperitoneal (VP) shunt and better neurodevelopmental outcome.2 3 18
Our aim was to test the hypothesis that very early intervention, before crossing the p97+4 mm line, reduces death and/or the need for VP shunt when compared with later intervention.
Patients and methods
Study infants
Enrolled infants were born between July 2006 and July 2016 and admitted to eight neonatal intensive care units in the Netherlands, five centres in Europe and one in the USA. Inclusion criteria: (1) preterm infants (gestational age (GA)≤34 weeks) with a grade III or IV haemorrhage diagnosed with cUS; (2) <28 days after birth; (3) progressive dilatation of both lateral ventricles with ventricular width >p97 and AHW >6 mm. Exclusion criteria: (1) chromosomal disorders; (2) congenital malformations; (3) cystic periventricular leukomalacia; (4) infection of the central nervous system prior to randomisation.
Cranial ultrasound
Serial cUS was performed at least twice a week following the diagnosis of a grade III/IV haemorrhage to diagnose PHVD and follow progression. Ventricular measurements, VI/AHW and TOD were performed on all ultrasound scans and plotted on the Levene and Davies graphs.12 16 Measurements were recorded following informed consent, at randomisation, before each lumber puncture (LP), 1, 2 and 3 weeks after the first LP, before ventricular reservoir (VR) insertion and weekly till stabilisation, discharge or VP shunt placement.
Treatment
Low threshold
Treatment was started after the VI had crossed p97 but before crossing the p97+4 mm line, the AHW was >6 mm but <10 mm and/or the TOD was >25 mm (figure 1). Intervention started with LPs (max 3), and if necessary, followed by insertion and taps from a VR, aiming for VI<p97 over the next 7–10 days. Ten mL/kg were removed once or twice a day, the volume adjusted according to cUS. When taps from a VR were still needed 28 days after insertion to keep the VI well below the p97+4 mm, one or two ‘challenges’ were performed with discontinuation of taps. Reservoir taps were resumed in case of expanding ventricles, clinical symptoms and/or excessive head growth. Taps were continued until infant’s weight reached 2000–2500 g and according to unit protocol, the protein had decreased to <1.5 g/L and erythrocytes <100/mm3, at which stage the infant became eligible for a VP shunt.
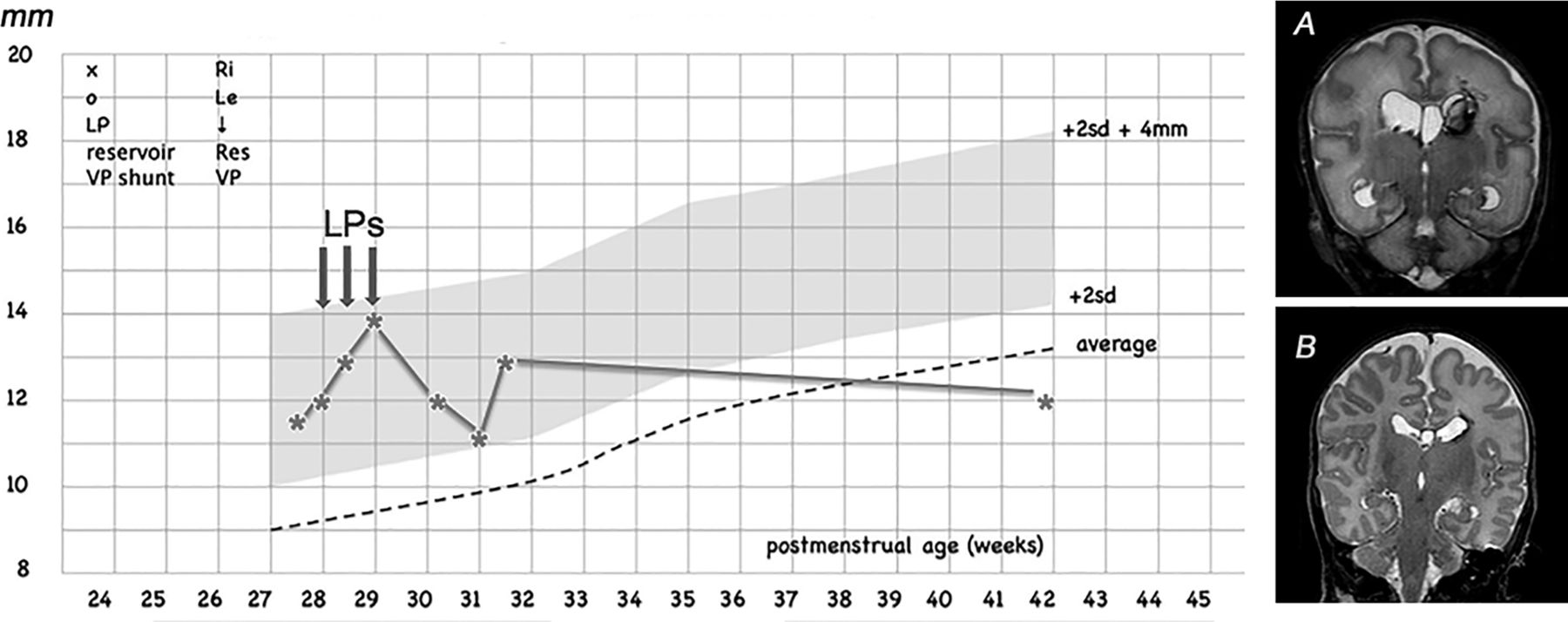
Example of early intervention, gestational age 26 weeks/birth weight 925 g; three lumbar punctures (LPs) were performed when the ventricular index had crossed the p97 (2SD) and was heading towards the p97+4 mm line. No further intervention was required. The first MRI (A, coronal T2-weighted sequence) was performed after the three LPs at 30 weeks postmenstrual age and the second MRI (B) at term equivalent age, showing remnants of the intraventricular haemorrhage and nearly normal size and shape of the lateral ventricles. VP, ventriculoperitoneal.
High threshold
Treatment was started once the VI had crossed the p97+4 mm line and the AHW was >10 mm. Further treatment was comparable to the early treatment arm (figure 2).
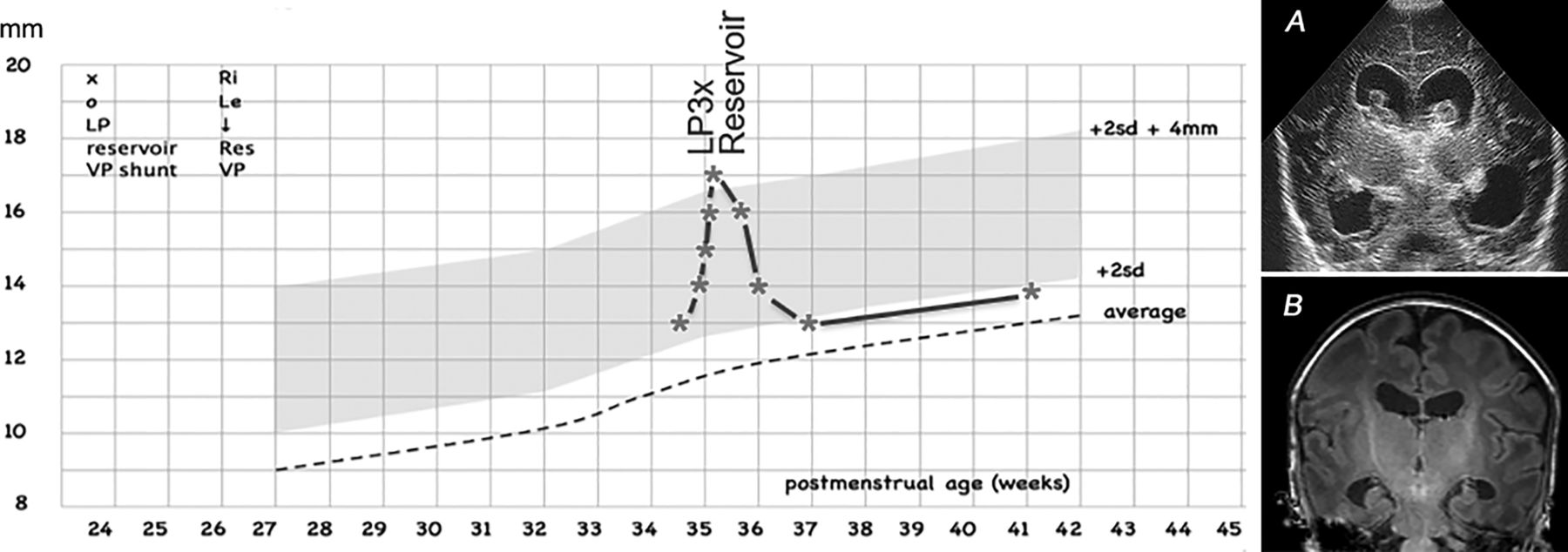
Example of later intervention, gestational age 33+6 weeks/birth weight 1790 g; three lumbar punctures (LPs) were performed once the ventricular index had crossed the p97+4 mm line and a ventricular reservoir was subsequently inserted. The ventricular index came down to below the p97 line with daily taps from the -ventricular reservoir, which could be stopped after 19 days. No further intervention was required. The coronal ultrasound (A) performed before the first LP shows intraventricular clots and ballooning shape of the lateral ventricles. The coronal MRI (T1-weighted image) at term equivalent age (B) shows mild ventricular dilatation. VP, ventriculoperitoneal.
Shunt surgery
Adequate weight, cerebrospinal fluid (CSF) protein and erythrocytes being achieved, reservoir punctures were discontinued and VI/AHW, head circumference measurements and clinical symptoms reviewed daily. If the local team observed continued ventricular expansion and accelerated head enlargement, a VP shunt was indicated, with symptoms increasing the urgency. An external review was performed later for infants who underwent shunt surgery. PG and LSdV reviewed the VI and AHW graphs, the head circumference graphs and the cUS images for infants shunted but not born in their own centres to confirm that shunt criteria were met. They were blind to the treatment allocation. These external reviews agreed with the local shunt decision in all cases.
Outcomes
Primary outcome was a composite of VP shunt placement and/or death. Diagnosis of VR dysfunction, infection and revision or need for a second reservoir were recorded as well as VP shunt dysfunction, infection and need for revision. Neurodevelopmental outcome at 2 years corrected age will be reported separately.
Randomisation and statistical analysis
Computer-generated randomisation was used online to allocate infants to treatment groups in a 1:1 ratio. Randomisation was stratified by centre and in blocks of 5. Analysis was by intention to treat.
Based on previous trials, inclusion criteria predicted that 60% of the infants would die or need a VP shunt. Our initial power calculation (using a 5% level of significance) indicated that 50 infants in each group would give 87% power of detecting a reduction from 60% in primary outcome to 30%. During the trial, the incidence of an adverse outcome was found to be much lower (around 45%) than the expected adverse outcome of 60%. Therefore, a new power calculation was done, indicating a sample size of 63 patients per study arm, to demonstrate a decrease in the adverse outcome with 45%–22% with a power of 80%.
Written informed consent was obtained from both parents of each infant.
Results
Recruitment started in the Netherlands in July 2006 and ended in July 2016. Due to slow enrolment, additional centres were invited to participate, Bristol 2007, St Louis 2009, Lund 2010, Cadiz, Barcelona and Lisbon 2013. A total of 126 infants were recruited. Most infants were recruited in Bristol (29), Utrecht (23), Nijmegen (23), Zwolle (12), Cadiz (12), while between 2 and 6 infants were enrolled in the other nine centres.
The two treatment groups were comparable for sex, gestational age and birth weight as well as having a grade III or IV haemorrhage and day of randomisation (table 1).
Clinical and intervention characteristics and primary outcomes
Low threshold group
All but two infants (97%) had their first LP on the day of randomisation. Two infants had no LPs, one was too unstable and the other due to violation of the protocol. Median number of LPs was 3 (range 0–6), and the number exceeded 3 in 12 (19%) infants, due to unavailability of the neurosurgeon or a theatre slot. A VR was inserted in 40 infants (62%), median of 6 days after the first LP. Reservoir dysfunction occurred in five infants (8%), due to dehiscence in one, obstruction in three, and malposition in one, requiring a second VR in four. In the other infant, 0.5 mg/kg of recombinant tissue plasminogen (rTPA) (Actilyse, Boehringer IngelheimInt, Ingelheim, Germany) was injected into the reservoir, which resolved the dysfunction. An infection occurred twice, once with Enterococcus faecalis, requiring removal of the VR and in the other infant Staphylococcus capitis was cultured with CSF sterilisation with intraventricular antibiotics. However, subsequently multiloculated pocket formation occurred, requiring endoscopic fenestration twice and subsequent VP shunt. Seven infants died (11%), two without any intervention (one due to Escherichia coli sepsis on the day of randomisation and the other 3 days after randomisation due to acute respiratory failure), two following LPs (one sepsis, one necrotising enterocolitis (NEC)) and three following insertion of a VR (one bronchopulmonary dysplasia, two NEC). Twelve required a VP shunt (19%), including one following unsuccessful fenestration of the third ventricle twice. Seven had a grade III and five had a grade IV haemorrhage. Shunt revision (<1 month after insertion) was needed in seven infants (58%) because of an infection in one (Streptococcus viridans) and dysfunction in the other six.
Higher threshold group
Thirty-six of the 62 (58%) infants had LPs, performed at a median of 5 days after randomisation. Median number of LPs was three (range 0–4), and the number was more than three in eight infants (22%), due to unavailability of the neurosurgeon or a theatre slot. VR was inserted in 27 infants (43%), median of 10 days after the first LP. VR dysfunction occurred in six infants (9%), due to obstruction in three, malposition in one and lack of communication between the two ventricles requiring placement of a second reservoir in two. An infection with Staphylococcus. aureus and Klebsiella pneumoniae occurred in two other infants, both were treated with antibiotics without removal of the VR. Nine infants died (14%), four without any intervention (two sepsis, one NEC, one acute respiratory failure), three following LPs (one sepsis, one BPD, one meningitis following discharge home) and two following insertion of a VR (one candida sepsis, one NEC). Fourteen infants required a VP shunt (23%), seven following a grade III and seven following a grade IV haemorrhage. One infant needed a revision following an infection, one had a disconnection but the VP shunt was not revised and in one infant a second fenestration was performed.
Comparison of primary outcome between early and later intervention
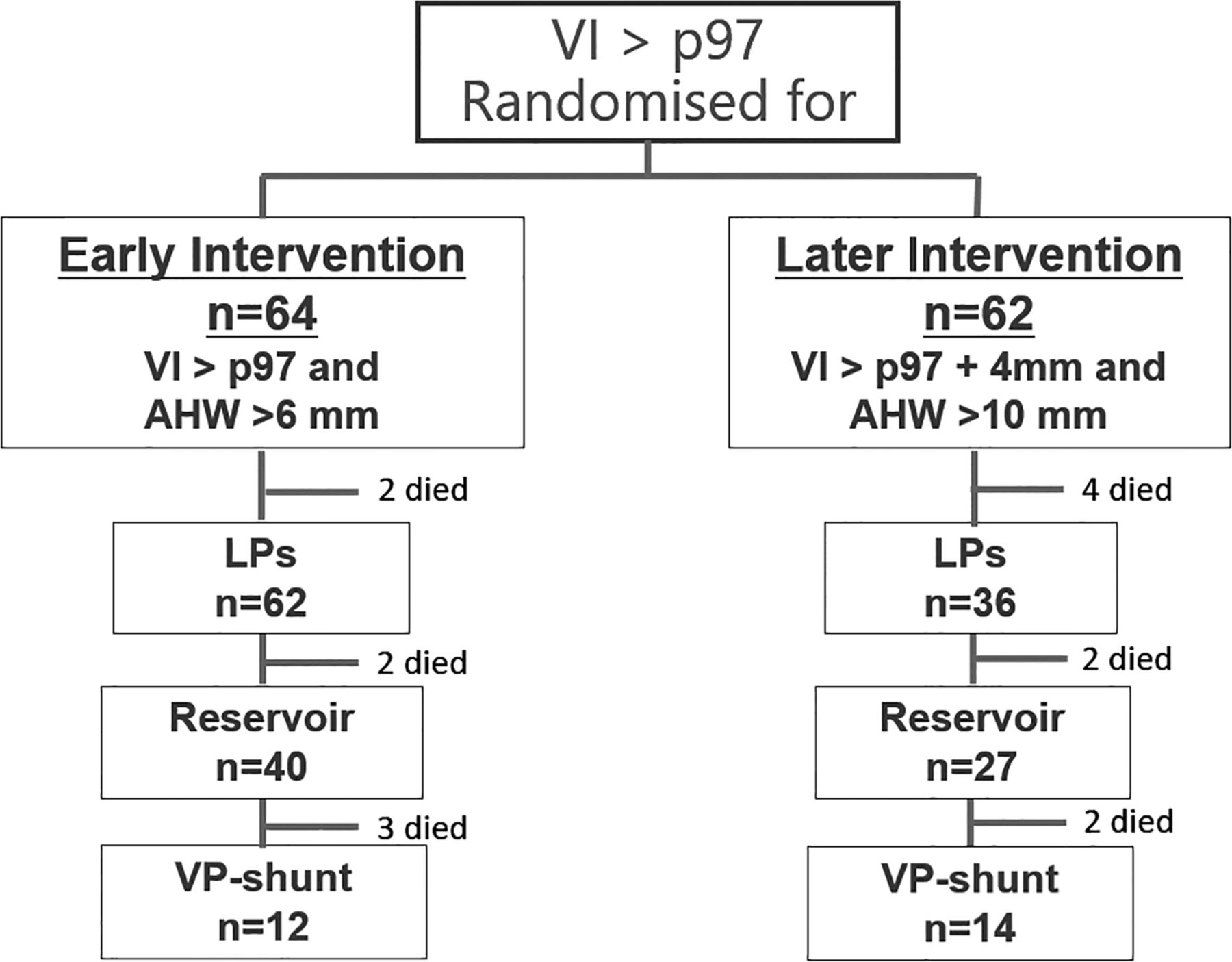
Outcomes at discharge are shown in table 1 and figure 3. Of 64 infants assigned to the LT group, 7 (11%) died and 12 (19%) underwent VP shunt surgery (death or shunt 30%). Of 62 infants assigned to HT group, 9 died (14%) and 14 (23%) required VP shunt placement (dead or VP shunt 37%). This difference was not significant (P=0.45). Revision of the VP shunt was required in 7/12 (58%) of the LT group vs 2/14 (14%) in the HT group (P<0.01). This could not be explained by a difference in protein levels or erythrocytes in the CSF prior to VP shunt placement.
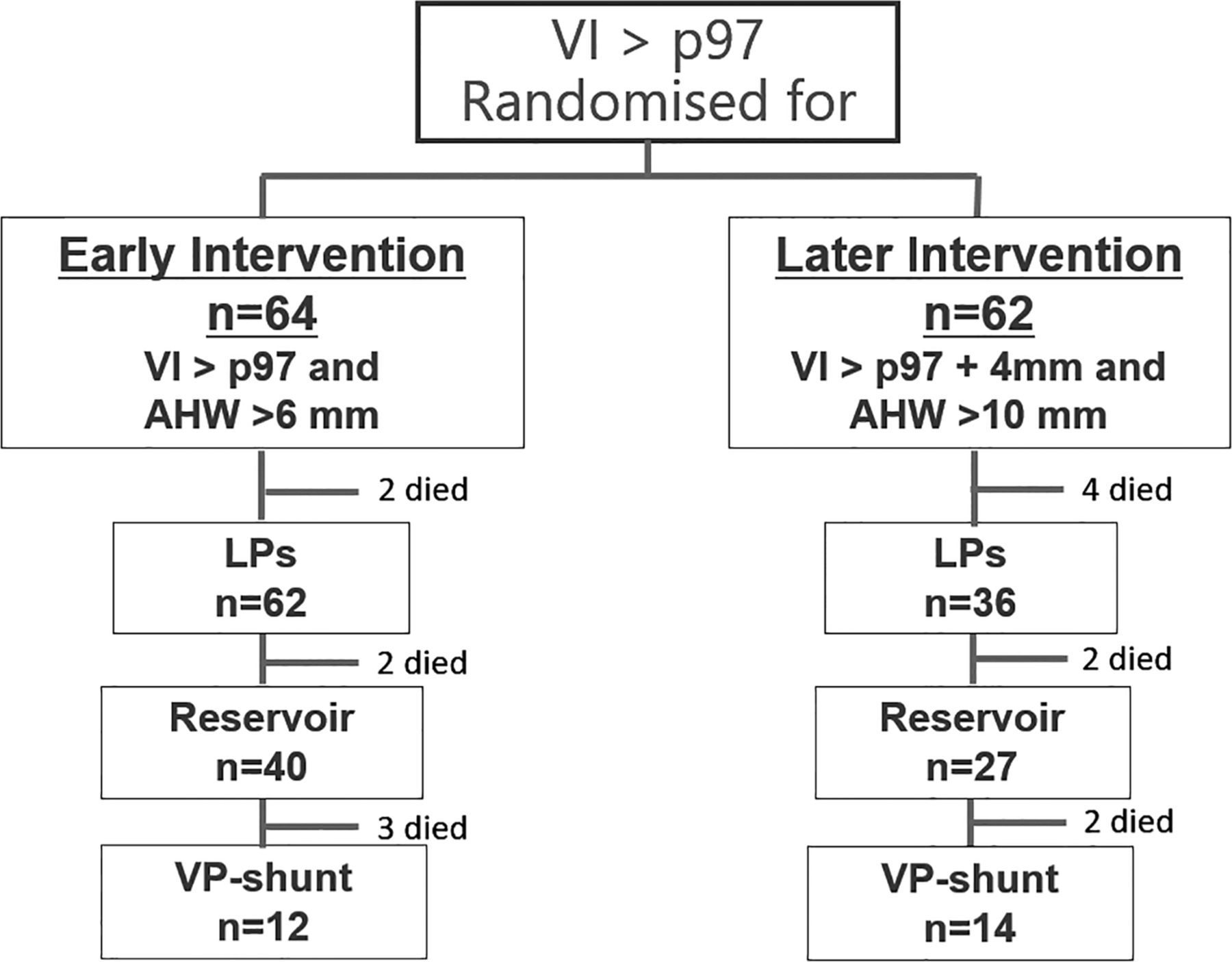
Flow chart of patient allocation and subsequent treatment of posthaemorrhagic ventricular dilatation. AHW, anterior horn width; LP, lumbar puncture; VI, ventricular index; VP, ventriculoperitoneal.
Randomisation was performed on median day 9 in both study arms, followed by significantly more LPs in the LT group (P<0.001). The first intervention after randomisation was performed median day 1.0 in the LT compared with median day 6 in the HT group (P<0.001). Subsequent insertion of a VR was also more often performed in the LT group (62% early group; 43% HT group; P<0.05). Insertion was performed at median day 6 following randomisation in the LT group, compared with day 10 in the HT group (P<0.001). VR dysfunction occurred in 5/40 (12.5%) of the LT group vs 6/27 (22%) in the HT group. Median maximum VI measurements (mm over p97) were 2.7 mm in the LT group compared with 4.0 mm in the HT group (P<0.001). Median maximum measurements of the AHW (mm over 6 mm) were 3.0 mm in the LT and 5.0 mm in the HT group (P<0.001) (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Median maximum ventricular measurements, including ventricular index in mm above the +2 SD line on the Y-axis on the left (panel A) and anterior horn width (AHW) in mm above the 6 mm line on the Y-axis on the right (panel B), for the infants in the low (LT) and the high threshold (HT) group depicted on the X-axis. Median maximum ventricular index measurements (mm >2SD) were 2.8 mm in the early group compared with 4.2 mm in the later intervention group (P<0.001). Median maximum measurements of the anterior horn width (mm >6 mm) were 3.0 mm in the early and 5.0 mm in the later intervention group (P<0.001).
Violation of the protocol
In the LT group, the first LP was performed too early in two infants, when the VI was still on p97 but without upward progression. In another two infants, the VI was never reduced <p97 and several measurements were over p97+4 mm (see online supplementary figure).
Supplementary file 1
![[SP1.jpg]](https://fn.bmj.com/content/fetalneonatal/104/1/F70/DC1/embed/inline-supplementary-material-1.jpg?download=true){kind=link}
In the HT group, the first LP was performed before the VI had crossed the p97+4 mm line in three infants. No LP was performed >p97+4 mm in two infants as they were too unstable and both subsequently died. Randomisation too early occurred, when the VI was on, but had not yet crossed, the p97 line and without progression of the PHVD. In two infants, the VI was never reduced <p97 and several measurements remained >p97+4 mm.
Ventricular reservoirs
No neurosurgeon was available on site in two Dutch centres and in one of the two hospitals in Bristol. Infants were referred following randomisation, and when the need for neurosurgery was expected. Reservoir placement was performed in the operating theatre in 10/14 centres. Taps from the reservoir were performed by the neonatal staff in 12 and by neurosurgical staff in the other 2 centres. There were more reservoir-related complications in infants treated during the first half than in the second half of the study period (10/19 and 5/33, respectively (P=0.01)). There was no significant difference in GA or birth weight for infants with and without complications.
Discussion
We were unable to show a further reduction in the need for a VP shunt in the LT group, but the need for VP shunt placement in both study groups is, to the best of our knowledge, the lowest reported so far. In the HT group, the number of infants who had LPs and VRs was significantly lower than in the LT group. Whether this increase in additional interventions in the LT group will be associated with improved preservation of brain volumes and improved neurodevelopmental outcome still needs to be determined. Intervention can be considered early in both groups, when compared with timing of intervention in previous studies. In the first randomised controlled trial (RCT) performed, the VentriculoMegaly trial, there was no upper limit on VI at entry and only LPs or ventricular taps were performed. These methods were only used to prevent further dilatation, but not to bring the VI down to within the normal range.13 There was no significant difference between the number of infants VP shunted between the two groups (53% and 54%). The next RCT, using acetazolamide and furosemide, also had no upper limit on VI at entry. Seven per cent had a VR inserted in the arm receiving drugs and 14% in the standard arm.14 The number of infants VP shunted was significantly higher in the treatment group (51%) compared with the standard treatment group (38%) and the composite outcome (death and/or shunt) was significantly worse in the treatment arm as well. The DRIFT (drainage, irrigation and fibrinolytic therapy) trial also had no upper limit on VI at entry. Thirty-eight per cent in the DRIFT arm had VR insertion and 75% in the standard group. Once again, there was no significant difference between the number of infants VP shunted between the two groups (38% and 39%). A recent prospective cohort study from the Hydrocephalus Clinical Research Network reported that 56% of those treated when the frontal-occipital horn ratio exceeded 0.55 with clinical symptoms were VP shunted.19 In a recent observational cohort study, as many as 92% of preterm infants required a shunt when treatment was started following onset of clinical symptoms.20
Enrolment in the present study was much slower than expected, as fewer infants developed a severe GMH-IVH. Compliance with trial management was generally good, but interpretation of the protocol was inappropriate in about 10% of the cases but following intention to treat, these infants were included in the analysis.
The rate of infection for the different intervention methods was low. CNS infection did not occur following LPs and in only 6% of the infants following VR insertion, similar to a previous single-centre study.21 A second VR was required in about 15% of the infants, mostly due to dysfunction. Both types of complications may further increase the risk of an adverse outcome. Infection is known to have an adverse effect on outcome, even when there is no evidence that the CNS is involved.22 Complications were less common during the second half of the study period, suggestive of a learning curve. Recently, more attention has been given to the risk of anaesthesia in young children and this may be especially important in extremely preterm infants.23 24 The proportion of VR and VP shunts with dysfunction needing revision was higher in the LT group than the HT group. Even though, in most centres, insertion of a VP shunt was only performed when the infant had reached a weight of 2–2.5 kg and the protein and red cell count were low, the need for revision was high (25%), which was due to disconnection or dysfunction in most cases. Each need for revision, involved a period of increased intracranial pressure and the need for anaesthesia. Every revision is associated with a small reduction in IQ points.25
In the DRIFT trial, there was no significant reduction in the need for a VP shunt, but a subsequent improvement in neurodevelopmental outcome at 2 years corrected age was noted in the DRIFT arm.26 In the current trial, we will determine whether the increased number of (neurosurgical) interventions needed in the early study arm influences neurodevelopmental outcome.
Conclusions
Control of PHVD, using LPs and taps from a VR before or just after the VI crossed the p97+4 mm line was associated with the lowest need for VP shunt reported so far. No significant reduction in VP shunt insertion and no difference in mortality was found following very early as compared with later intervention for PHVD but intervention at p97+4 mm involved fewer LPs and reservoir insertions.
References
Footnotes
Contributors All authors and partners of the ELVIS study group. Enrolled patients in one of the 14 participating centres. Entered clinical data in the Electronic database. Had substantial contributions to the conception or design of the work, or the acquisition, analysis or interpretation of data. Drafting the work or revising it critically for important intellectual content. Final approval of the version published. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Competing interests None declared.
Patient consent Parental/guardian consent obtained.
Ethics approval The study (ISRCTN43171322) was approved by the Medical Ethics Board Erasmus Medical Center Rotterdam.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Eight of 126 infants are also included in another paper. This is an observational study about posthaemorrhagic ventricular dilation, which is a present in press for Neurology. These data can be accessed when needed from the first author.
Collaborators The ELVIS study group: Han K; Division of Neuroscience, Department of Neurosurgery, University Medical Centre, The Netherlands, Steggerda S; Department of Neonatology, Leiden University Medical Center, Leiden, The Netherlands, Benders MJNL; Department of Neonatology and Brain Center Rudolf Magnus, Wilhelmina Children’s Hospital, University Medical Center Utrecht, Utrecht, The Netherlands, Dudink J; Department of Neonatology and Brain Center Rudolf Magnus, Wilhelmina Children’s Hospital, University Medical Center Utrecht, Utrecht, The Netherlands; ter Horst HJ; Department Neonatology, UMCG, Groningen, The Netherlands, Dijkman KP; Department Neonatology, Máxima Medical Center, Veldhoven, The Netherlands, Ley D; Department Pediatrics, Institute of Clinical Sciences, Lund, Sweden, Fellman V; Department Pediatrics, Institute of Clinical Sciences, Lund, Sweden, de Haan TR; Department Neonatology, Emma Children’s Hospital, Academic Medical Center, University of Amsterdam, The Netherlands, Agut Quijano T; Department Neonatology, Hospital Sant Joan de Deu, Barcelona, Spain, Barcik U; Department Neonatology, Hospital Sant Joan de Deu, Barcelona, Spain, Mathur A; Division of Newborn Medicine, Edward Mallinckrodt Department of Pediatrics, Washington University School of Medicine, St Louis, USA, Graca AM; Department Neonatology, Hospital de Santa Maria, Lisbon, Portugal.
Linked Articles
- Fantoms