Article Text

Abstract
Objective Failure of closure of the patent ductus arteriosus (PDA) may be associated with harm. Early cardiac ultrasound-targeted treatment of a large PDA may result in a reduction in adverse outcomes and need for later PDA closure with no increase in adverse effects.
Study design Multicentre, double-blind, placebo-controlled randomised trial.
Setting Three neonatal intensive care units in Australia.
Patients and interventions Eligible infants born <29 weeks were screened for a large PDA and received indomethacin or placebo before age 12 h.
Main outcome Death or abnormal cranial ultrasound.
Results The trial ceased enrolment early due to lack of availability of indomethacin. 164 eligible infants were screened before 12 h; of the 92 infants with a large PDA, 44 were randomised to indomethacin and 48 to placebo. There was no difference in the main outcome between groups. Infants receiving early indomethacin had significantly less early pulmonary haemorrhage (PH) (2% vs 21%), a trend towards less periventricular/intraventricular haemorrhage (PIVH) (4.5% vs 12.5%) and were less likely to receive later open-label treatment for a PDA (20% vs 40%). The 72 non-randomised infants with a small PDA were at low risk of pulmonary haemorrhage and had an 80% spontaneous PDA closure rate.
Conclusions Early cardiac ultrasound-targeted treatment of a large PDA is feasible and safe, resulted in a reduction in early pulmonary haemorrhage and later medical treatment but had no effect on the primary outcome of death or abnormal cranial ultrasound.
Registered Trial Australian New Zealand Clinical Trials Registry (ACTRN12608000295347).
Statistics from Altmetric.com
What is already known on this topic
-
Trials of treatment of the patent ductus arteriosus in unselected populations have failed to show benefits.
-
Early prophylactic indomethacin reduces periventricular/intraventricular haemorrhage but does not improve neurodevelopmental outcome.
What this study adds
-
It is feasible to identify infants with a large patent ductus arteriosus (PDA) early after birth with ultrasound and target treatment to this group.
-
Indomethacin treatment of a large PDA before 12 h of age reduced pulmonary haemorrhage and subsequent symptomatic treatment without causing harm.
-
Early cardiac ultrasound-targeted treatment had no effect on the primary outcome of death or abnormal cranial ultrasound in this underpowered study.
Introduction
Early or prophylactic treatment of a patent ductus arteriosus (PDA) has demonstrated a reduction in the rate of periventricular/intraventricular haemorrhage (PIVH) and pulmonary haemorrhage (PH) and reduced need for subsequent medical or surgical closure.1–4 Despite these clear short-term benefits, this has not translated into improved outcomes for surviving infants3 and the practice has not been widely adopted. Clinicians appear unwilling to accept exposure of infants to a treatment where some will have great benefit5 but where there is also potential for harm including renal impairment,6 gastrointestinal tract injury,7 fluid retention, risk of bronchopulmonary dysplasia (BPD) and transient cerebral vascular restriction.8
Ductal constriction in the very preterm in the early postnatal hours is characterised by great variance and those babies with poor constriction are at higher risk of PIVH, PH and later need for PDA treatment.9–11 If early prophylactic treatment could be targeted at only those with poor PDA constriction, then the benefits may be maximised and potential harms minimised. We hypothesised that early ultrasound-targeted PDA treatment in babies born before 29 weeks would result in a reduction in mortality and abnormal cranial ultrasound findings as well as subsequent need for medical or surgical PDA closure with no increase in short-term adverse effects.
Methods
A multicentre, double-blind, placebo-controlled randomised trial was conducted in infants born before 29 weeks between January 2007 and December 2010. Infants were recruited from three Australian tertiary neonatal intensive care units.
Eligible infants were born at or transferred to one of the participating hospitals and able to have an initial screening cardiac and cranial ultrasound before 12 h of age. Infants were excluded if they had a Grade 2–4 PIVH, PH, if they were clinically unstable and not expected to survive, if they had a significant congenital anomaly, if there was structural heart disease or if they had specific contraindications to indomethacin treatment such as thrombocytopaenia (<50 000/mm3), raised creatinine (>120 µmol/L) or severe growth restriction (<3rd centile) with abnormal umbilical Doppler arterial flows. Infants with ductal right to left shunting for more than 33% of the cardiac cycle, indicative of pulmonary hypertension,12 were not randomised immediately. Randomisation occurred if this had resolved by 12 h. Sample size was calculated using the primary outcome of combined death or abnormal cranial ultrasound at discharge which had an a priori incidence of 21% in our population. To detect an absolute reduction in this rate to 10% (power of 0.8 and significance of 0.05) would require 170 in each arm. In December 2010, after we had screened 164 infants and randomised 92 of these, intravenous indomethacin was withdrawn from the Australian market. The trial was closed in March 2011 as the drug remained unavailable. A data and safety monitoring committee oversaw the trial; the first of three planned interim analysis recommended continuing the trial with no evidence of safety issues in prespecified outcomes.
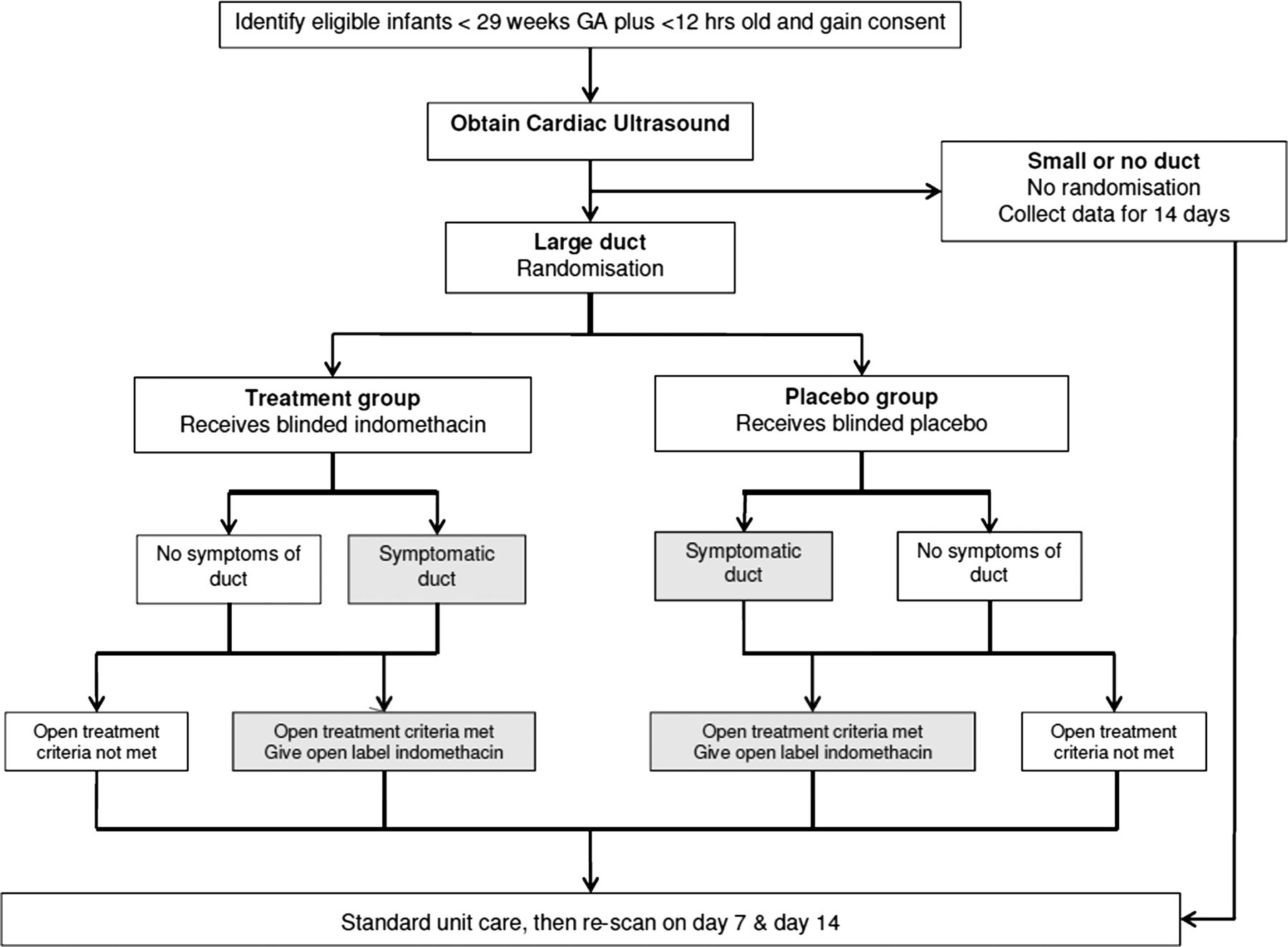
The study procedures are summarised in figure 1. Eligible infants received a clinician performed cardiac ultrasound between 3 and 12 h of birth to establish structural normality, measure the PDA diameter and assess the direction of ductal shunt. Infants with Grade 2–4 PIVH on this initial cranial ultrasound were excluded. The PDA diameter was measured as previously described.13 The PDA was classified as either large or small based on the relevant 50th centile postnatal age cut points from a population-based study of 417 infants from the participating units documenting the PDA within the first 12 h of life by gestational and postnatal age.14 The PDA diameters used were >1.8 mm at postnatal age 3–5 h, >1.6 mm at postnatal age 6–8 h and >1.3 mm at postnatal age 9–12 h.14 Infants classified as having a large PDA were block randomised by gestational age (GA) groups (23–24, 25–26 and 27–28 weeks) and centre by each centre's pharmacy using a random number–generated table. Syringes containing either the study drug (Indocid PDA, Merck, Sharpe and Dome at a concentration of 1 mg/2 mL) or a saline placebo were prepared by pharmacy. Infants received a loading dose of 0.2 mg/kg followed by 0.1 mg/kg for two further doses at 24-h intervals administered by 30-min infusion or the equivalent volume of normal saline. Clinicians, investigators and nursing staff remained blinded.

DETECT (Ductal Echocardiographic Targeting and Early Closure Trial) study flow diagram.
Further cardiac ultrasounds in the first 72 h to assess ductal size were only permitted if strict criteria for open-label treatment were met. Open-label treatment after the first 72 h was discouraged but remained at the discretion of the treating clinician if treatment criteria were met. Open-label treatment criteria in the first 72 h (during trial drug treatment) were:
-
PH defined as blood stained respiratory secretions WITH a significant change in respiratory requirements and chest x-ray (CXR) changes in the presence of echocardiographic evidence of significant left to right ductal shunting.
-
Severe persistent (>30 min) hypotension (mean blood pressure<GA in weeks) thought to be due to PDA and unresponsive to pressor therapy with echocardiographic evidence of significant left to right ductal shunting.
Open-label treatment criteria after 72 h required all of the following criteria to be met:
-
Echocardiographic evidence of a haemodynamically significant PDA (>1.5 mm diameter measured using colour Doppler).
-
Presence of a systolic murmur typical of a PDA.
-
Evidence of and documentation of a clinical effect such as worsening ventilatory settings (more than 10% change in FiO2 or need for mechanical ventilation from continuous positive airway pressure (CPAP)), cardiomegaly and pulmonary oedema on chest X-ray, or resistant hypotension (persisting mean blood pressure<GA for >4 h despite vasopressor treatment).
Surgical treatment was allowed, if there was persisting ventilator dependence or congestive cardiac failure with echocardiographic evidence of a haemodynamically significant duct and failure of two open-label medical courses. Study drug was ceased if there were complications thought to be due to indomethacin. A further cardiac ultrasound to assess PDA was obtained on Day 7 and Day 14. The study intervention ended at Day 14 after which infants could be treated as per the discretion of the treating clinician; however, reasons for open-label treatment were still documented. Late cranial ultrasounds (closest to 6 weeks postnatal age) were recorded.
The primary outcome was combined death and/or abnormal cranial ultrasound (PIVH Papile Grade ≥2 or cystic periventricular leukomalacia (PVL)) at nursery discharge. Secondary outcomes included mortality, PIVH, PVL, total doses of indomethacin, side effects of indomethacin; renal impairment (elevated creatinine >150 µmol/L, oliguria <1.0 mL/kg/h for >12 h during treatment), gastrointestinal bleeding, spontaneous intestinal perforation, necrotising enterocolitis (NEC)—greater than stage 1 of Bell's classification, time to full oral feeds (150 mL/kg/day), PH (frank blood stained respiratory secretions, a sudden clinical increase in respiratory support and CXR changes), retinopathy of prematurity, sepsis (positive blood culture and antibiotics>5 days), duration of mechanical ventilation, CPAP, oxygen therapy and hospitalisation, BPD (physiological requirement for oxygen at 36 weeks’ GA) and diuretics or postnatal steroid for BPD. Developmental outcome at 12 and 36 months is planned.
Data were analysed on an intention to treat basis using IBM SPSS Statistics software (IBM Corporation, Chicago). Continuous variables were compared using Student t test or Mann–Whitney U. Categorical variables were analysed using χ2 or Fishers exact. Statistical significance of the primary outcomes was taken at p value <0.05.
Results
During the trial period, 393 infants were born before 29 weeks’ GA in the participating hospitals. Of these, there were 103 parental refusals, 8 clinician refusals and 85 infants were excluded for the reasons listed in figure 2; 164 infants underwent cardiac ultrasound screening of which 94 (57%) were classified as having a large PDA and 70 a small or closed PDA. There was an insignificant trend towards more large PDAs at lower GA (16/23 at 23–24 weeks, 32/64 at 25–26 weeks and 46/77 at 27–28 weeks). Of the infants with large PDA, 44 were randomised to indomethacin and 48 to placebo, evenly spread across the GA strata (figure 2). All infants received the allocated therapy, but 2 in the indomethacin group and 4 in the placebo group did not receive all 3 doses due to death or contraindications developing. Two infants with large PDA were excluded from randomisation due to evidence of raised pulmonary pressures. Outcomes were determined in all other infants screened.

{kind=link}
{kind=link}
CONSORT (Consolidated Standards of Reporting Trials) diagram of the DETECT study. CHD, congenital heart disease; PPHN, persistent pulmonary hypertension; IUGR, intrauterine growth restriction.
Baseline characteristics
There were no significant differences in baseline characteristics of infants with a large PDA by treatment allocation (table 1). The mean age at receipt of the study drug was 9 h.
Baseline characteristics of infants with a large patent ductus arteriosus (PDA) randomised to indomethacin or placebo
Primary outcome
The primary outcome of combined death and/or abnormal cranial ultrasound (PIVH Papile Grade ≥2 or cystic PVL) at nursery discharge was not different between the two groups—8/44 (18%) in the indomethacin group versus 9/48 (19%) in placebo (table 2). The individual components of the combined outcome showed no significant differences. There was no effect of GA when analysed according to our prespecified strata (table 2). Some infants had more than one outcome.
Outcomes of infants with a large patent ductus arteriosus (PDA) randomised to indomethacin or placebo
Secondary outcomes
The secondary outcomes for infants with a large PDA randomised to indomethacin or placebo are shown in table 3.
Secondary outcomes of infants with a large patent ductus arteriosus (PDA) randomised to indomethacin or placebo
The reduction in PH prior to 72 h was significant with a number needed to treat of 5.4 to prevent one PH. The rate of PH during the entire study period was not different (9% vs 23%, indomethacin vs control, p=0.07). Fewer infants who received targeted indomethacin received open-label treatment. Open-label treatment was given to nine infants in the indomethacin arm (3/8 at 23–24 weeks, 6/15 at 25–26 weeks and 0/21 at 27–28 weeks) and to 19 infants in the placebo arm (7/8 at 23–24 weeks, 8/16 at 25–26 weeks and 4/24 at 27–28 weeks). Open-label therapy was given after 72 h in 21/28 babies overall. Only two infants in the cohort received surgical ligation, both in the placebo group. There was no difference in other measured outcomes. When the significant secondary outcomes were stratified by GA, it was clear that 28 weeks’ GA babies had less adverse effects, but the numbers were too small to properly assess significance (table 4).
Relevant secondary outcomes by GA stratification
Discussion
Our trial demonstrates the feasibility of early cardiac ultrasound-targeted management of the PDA. We selected a high risk group of infants based on PDA size in the first 12 h after birth and administered early indomethacin or placebo. Early targeted treatment had no effect on the primary outcome of death or abnormal cranial ultrasound, although early closure of the trial before full enrolment due to lack of availability of the trial drug decreased power to detect a difference. Despite the premature trial closure, we found a significant reduction in early PH after targeted indomethacin treatment, consistent with the findings of others.4 The high rate of PH seen in our study (11.7% overall) is consistent with other studies including the Trial of Indomethacin Prophylaxis in Preterms (TIPP) trial and the latest Cochrane review.1 ,3 Early indomethacin also reduced the need for later medical treatment, which may be less effective.15 Our approach resulted in no adverse gastro-intestinal or renal effects. Other outcomes including receiving oxygen at 36 weeks postmenstrual age and retinopathy of prematurity were also not different.
Whether and when to treat a PDA remains controversial.16 Strategies range from aggressive management17 to a more conservative approach, with some suggesting that the PDA is an innocent bystander to adverse outcomes.18 A conservative approach to PDA treatment limits exposure to the side effects of non-steroidal anti-inflammatory drugs (NSAID)19 but may put an infant at risk of the complications of a large systemic to pulmonary shunt including PH, chronic lung disease, potential disturbances of cerebral blood flow and rarely cardiac failure.11 ,20 Many of these risks occur early, in the first 24 h.20
The use of prophylactic indomethacin reduces the incidence of a symptomatic PDA and severe PIVH;1 however, in the TIPP trial3 prophylactic indomethacin did not lead to improved neurodevelopmental outcome. A possible explanation for this paradoxical finding is that the effect of early indomethacin treatment depends on ductal presence and size. In infants with a large PDA it aids closure and reduces adverse effects. In contrast, infants exposed to NSAID without a significant PDA may suffer adverse effects, possibly mediated by a reduction in cerebral blood flow21 or fluid retention1 ,22 with changes in lung compliance and development of chronic lung disease, itself a marker for neurodevelopmental impairment.
Longitudinal natural history studies of PDA in preterm infants have demonstrated a wide range of constriction in the first few hours of life. Eighty-nine per cent of infants with a large PDA defined by colour Doppler diameter at 6 h of age received closure treatment.11 ,13 In contrast, the background rate of treatment in an unselected population was 40%. There is no evidence that delaying therapy with NSAIDs until a PDA is clinically symptomatic (generally Day 3–7) improves long-term outcome and some concerns that treatment after a period of exposure to relative organ hypoperfusion from a ductal steal potentiates the adverse effects of NSAIDs on the gut (perforation) and the kidney (renal failure). The prophylactic indomethacin trials demonstrated that earlier treatment with NSAID results in improved efficacy but no increased risk of harm.1 ,3 ,15
As this trial intended to treat infants in the same time frame as the indomethacin prophylaxis trials we used a similar dosage regimen. The average time of first dose in both groups was 9 h, reflecting the complexities of obtaining early consent. Open-label treatment of the PDA resulted in significant contamination of randomisation arms in previous trials. In our trial despite having strict criteria for open-label treatment, 20% of indomethacin treated infants and 40% of placebo received open-label treatment demonstrating that many clinicians still feel that ductal treatment is an important aspect of care.
The utility of early clinician performed ultrasound23 to define either a large or small PDA was also assessed by this trial. We found that infants who had a large, untreated PDA (our placebo group) had a higher chance of adverse outcome including PH and increased later treatment with indomethacin. In contrast, infants judged to have a small PDA on ultrasound in the first 12 h had an 80% chance of spontaneous closure, making this a clinically useful screen.24
The primary limitation of this trial was the lack of power to demonstrate the primary outcome following early closure. The significant number of infants where there was parental or clinician refusal to enrol in the trial reflected some of the uncertainties that remain in this area. This may have resulted in a biased group being enrolled, although the baseline characteristics of the randomised infants are similar to our nursery population. Due to the large numbers required to assess a primary outcome of neurodevelopment at 2 years, we chose an intermediate combined outcome of death/abnormal cranial ultrasound. It is our intent to follow our cohort through to the age of 3 years and report neurodevelopmental outcome.
We conclude that early cardiac ultrasound-targeted treatment of a large PDA is feasible and safe. There is some evidence of protection from PH and a demonstrated reduction in the need for subsequent later medical treatment. The benefits of ultrasound-targeted therapy were not associated with harm. A larger randomised control trial of this strategy will be needed to demonstrate potential efficacy in the prevention of important short-term outcomes including death and cerebral injury. Such a trial should be powered on neurodevelopmental follow-up as a primary outcome.
References
Footnotes
-
Contributors MK conceived and designed the trial, was PI at his site, enrolled patients, entered data, analysed the data, prepared and reviewed the manuscript before publication. AG helped design the trial, was PI at his site enrolled patients, entered data, analysed the data and reviewed the manuscript for publication. MJ consented and enrolled patients, entered and cleaned data from all sites and reviewed the manuscript before publication. NE conceived and designed the trial, was PI at his site, enrolled patients, entered data, analysed the data and reviewed the manuscript for publication.
-
Funding This study was in part funded by Heart Research Australia.
-
Competing interests None.
-
Patient consent Obtained from the parents.
-
Ethics approval Human Research Ethics Committee of each of the participating hospitals.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Fantoms