Article Text

Abstract
The genital mycoplasma species, Ureaplasma parvum and Ureaplasma urealyticum are the most common organisms isolated from infected amniotic fluid and placentas, and they contribute to adverse pregnancy outcomes including preterm birth and neonatal morbidities. In our institution, almost half of the preterm infants of less than 32 weeks gestation are Ureaplasma-positive in one or more compartment (respiratory, blood and/or cerebrospinal fluid), indicating that these organisms are the most common pathogens affecting this population. This review will focus on the compelling epidemiological and experimental evidence linking perinatal Ureaplasma species exposure to important morbidities of prematurity, such as bronchopulmonary dysplasia, intraventricular haemorrhage and necrotising enterocolitis.
- Neonatology
- Ureaplasma Parvum
- Ureaplasma Urealyticum
- Bronchopulmonary Dysplasia
- Intraventricular Hemorrhage
Statistics from Altmetric.com
- Neonatology
- Ureaplasma Parvum
- Ureaplasma Urealyticum
- Bronchopulmonary Dysplasia
- Intraventricular Hemorrhage
Introduction
Ureaplasma parvum (serovars 1, 3, 6 and 14) and Ureaplasma urealyticum (serovars 2, 4, 5 and 7–13) lack cell walls, hydrolyse urea to generate ATP, have limited biosynthetic functions, adhere to human mucosal surfaces of the genitourinary tract in adults and respiratory tract in newborns and are among the smallest free-living, self-replicating cells.1 These organisms can be detected in vaginal flora in 40%–80% of healthy women and their presence has been causally linked to infertility, early pregnancy loss, stillbirth, preterm birth and neonatal morbidities.2 Vertical transmission from mothers to their infants occurs in utero or during delivery. Although these organisms have been considered of low virulence, in vitro and in vivo experimental models have provided additional evidence supporting a role for Ureaplasma species (spp.) in these disorders. This review will focus on the compelling epidemiological and experimental evidence linking perinatal Ureaplasma spp. exposure to important morbidities of prematurity, such as bronchopulmonary dysplasia (BPD), intraventricular haemorrhage (IVH) and necrotising enterocolitis (NEC) (table 1). These associations suggest that strategies targeting this infection during pregnancy and after preterm birth may improve obstetric and neonatal outcomes.
Short-term and long-term complications associated with perinatally acquired Ureaplasma species
Association of ureaplasma species and BPD
The rate of respiratory tract colonisation with Ureaplasma spp. in very low birth weight infants (<1501 g) ranges from 20% to 45%. In a recent prospective cohort from the University of Maryland Medical Center, we observed that Ureaplasma spp. respiratory colonisation was inversely related to gestational age (OR, 0.821; CI 0.720 to 0.934). Sixty-five per cent of infants <26 weeks gestation were culture or PCR-positive one or more times during the first month of life compared with 31% infants ≥26 weeks gestational age (figure 1A).19 Respiratory colonisation is higher in infants delivered by spontaneous vaginal delivery following preterm onset of labour or preterm premature rupture of membranes and is increased with duration of membrane rupture.20 The lowest colonisation rates are in infants delivered for maternal indications and small-for-dates infants. At all gestational ages, U parvum serovars are the most common (figure 1B). In a prospective preterm cohort, serovars 3 and 6 alone and in combination accounted for 96% U parvum respiratory isolates.19 U urealyticum isolates were commonly a mixture of multiple serovars with serovar 11 alone or combined with other serovars (59%) as the most common serovar.
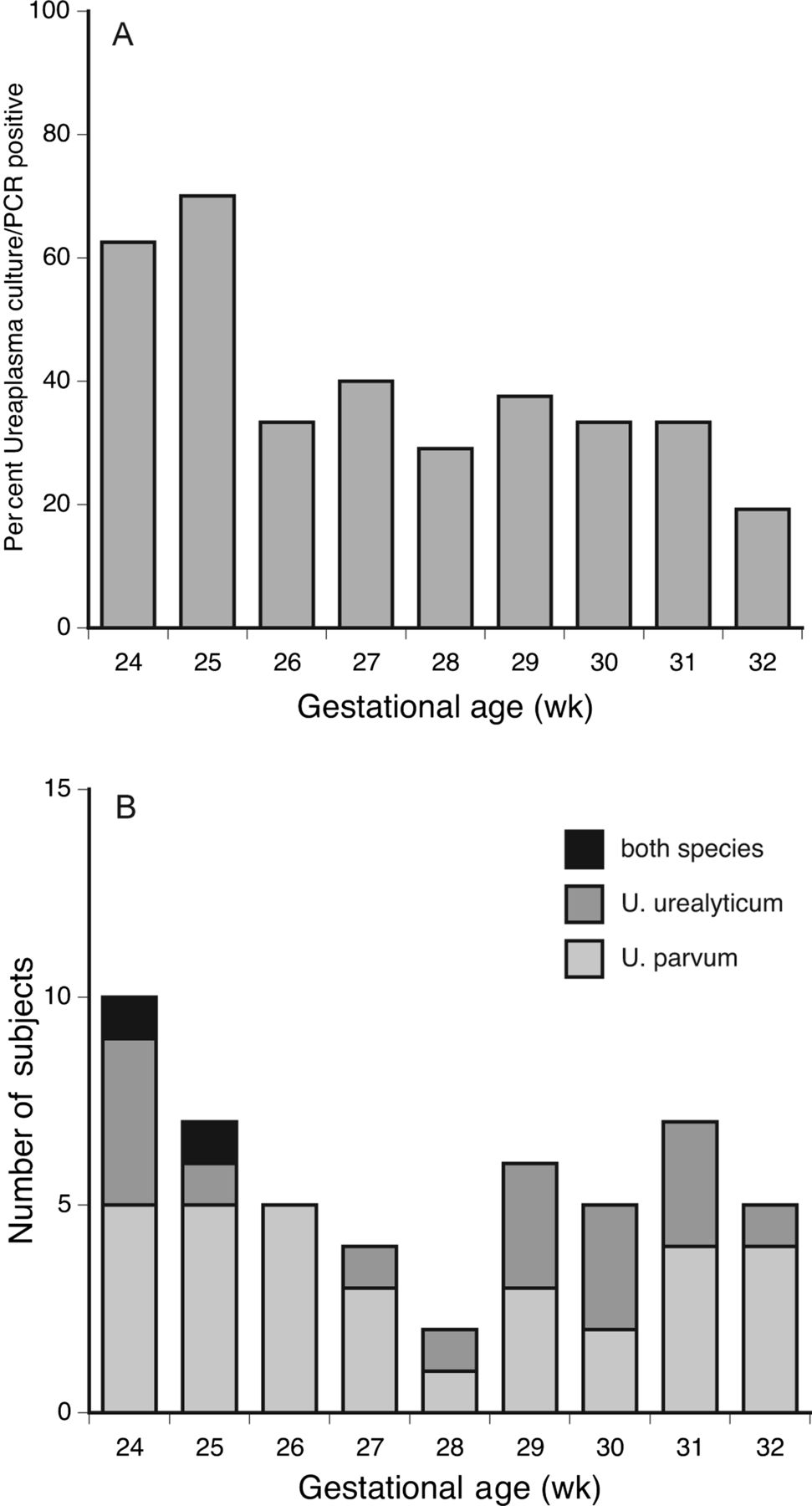
The frequency of respiratory colonisation during the first month of life with Ureaplasma species by gestational age (A) and distribution of species at each gestational age (B). Reproduced with permission.19
Although the contribution of Ureaplasma respiratory tract colonisation to the development of BPD has been debated since it was first reported in 1988, two meta-analyses published in 199521 and 20055 observed a significant association between Ureaplasma spp. respiratory tract colonisation and BPD defined as oxygen dependence at 28 days or at 36 weeks postmenstrual age. Ureaplasma spp. respiratory tract colonisation is associated with a peripheral blood leukocytosis16 and early radiographic emphysematous changes of BPD.3 ,20 ,22 These findings may be explained, in part, by an in utero onset of the inflammatory response and lung injury. Indeed, neonatal Ureaplasma spp. respiratory colonisation was associated with BPD in infants exposed to antenatal histological chorioamnionitis.23
Postnatal exposures may augment lung injury. Recently, we observed that in infants who had been mechanically ventilated for any duration and had a positive tracheal aspirate with or without a paired positive nasopharyngeal sample had a 7.9-fold increased risk (OR=7.86, CI 1.31 to 47) to develop moderate–severe BPD than mechanically ventilated infants with a positive nasopharyngeal sample alone.19 This suggests that lower tract infection, but not nasopharyngeal colonisation, augments lung injury in mechanically ventilated infants. However, Inatomi et al24 observed that risk for moderate–severe BPD was increased 4-fold in infants <29 weeks gestation with Ureaplasma-positive gastric aspirates and mechanical ventilation for ≥2 weeks duration. These studies suggest that use of non-invasive modes of respiratory support may be particularly beneficial in Ureaplasma-positive infants.
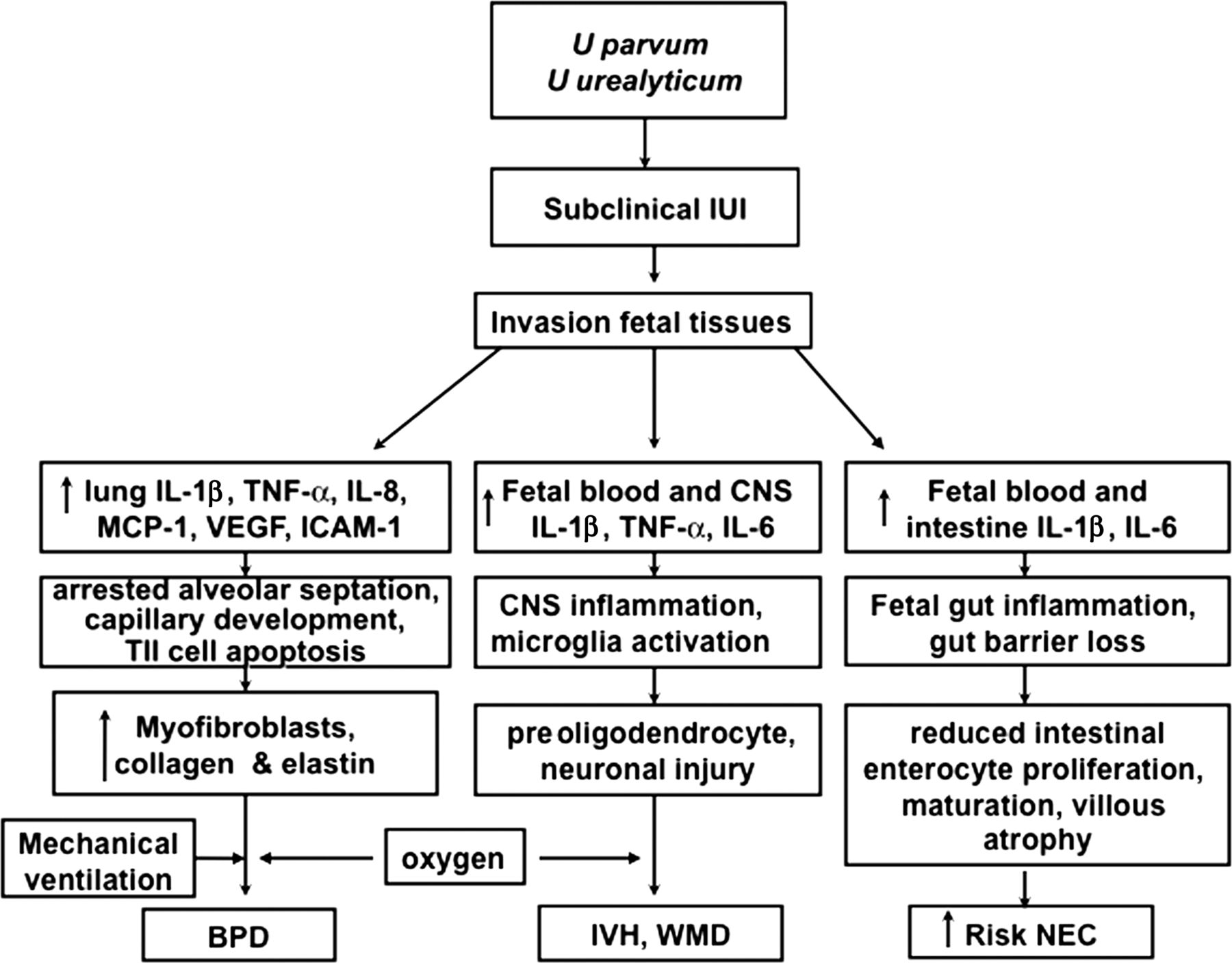
Epidemiological studies of human preterm infants and experimental intrauterine infection models in mice, sheep and non-human primates have contributed insights into the pathogenesis of Ureaplasma-mediated lung injury. Infants dying with Ureaplasma pneumonia share histological characteristics including moderate-to-severe fibrosis; increased myofibroblasts; disordered elastin accumulation; and increased number of tumour necrosis factor-α (TNF-α) and transforming growth factor β1 (TGFβ1) immunoreactive cells.2 Similar findings were observed in the 125-day immature baboon model antenatally infected with U parvum and exposed postnatally to ventilation and oxygen.25 In intrauterine U parvum infection in rhesus macaques, the duration of intrauterine ureaplasma exposure determined the severity of fetal lung injury, influx of inflammatory cells and epithelial necrosis.26 Lung fibrosis and thickened alveolar walls were evident for exposures greater than 10 days. In the ovine intrauterine infection model, fetal lung expression of TGFβ signalling components and elastin deposition were differentially affected by acute exposure to either U parvum serovar 3 or lipopolysaccharide (LPS) alone or combined exposure to U parvum and LPS.27 These data confirm that antenatal ureaplasma exposure contributes to lung inflammation, altered lung development and lung fibrosis that are characteristic of the BPD phenotype. Moreover, these data suggest that the ureaplasmas contribute to an augmented, dysregulated inflammatory response to postnatal stimuli, such as volutrauma and hyperoxia (See figure 2).
{kind=link}
{kind=link}
Overview of potential inflammatory pathways involved in ureaplasma-mediated morbidities bronchopulmonary dysplasia, intraventricular haemorrhage and necrotising enterocolitis. Modified from Viscardi.2
Association of Ureaplasma spp. and NEC
In addition to being isolated from respiratory secretions, the ureaplasmas have been detected in gastric aspirates and rectal cultures. Serial assessments of the gastro-oesophageal microbiota flora composition in 12 infants <32 weeks gestation during the first month of life using 16S rDNA analysis revealed that U parvum and U urealyticum were the predominant species during the first week of life, but were undetectable in all infants by the fourth week.28 Direct exposure of the fetal intestinal tract to microbes and amniotic fluid containing inflammatory mediators may stimulate an inflammatory response and alter intestinal barrier development leading to increased intestinal permeability and potential bacterial translocation. In the sheep intrauterine infection model, fetal intestinal exposure to amniotic U parvum serovar 3 isolate for up to 14 days prior to preterm delivery at 124 days gestation (term 150 days) caused intestinal inflammation, reduced enterocyte proliferation and villous atrophy.8 These effects were ameliorated by concomitant treatment with recombinant interleukin-1 receptor antagonist, suggesting that IL-1 signalling mediates these effects of fetal ureaplasma infection.
Recently, we demonstrated that respiratory infection with Ureaplasma spp. in preterm infants <33 weeks gestation increased the risk for NEC 2-fold.7The incidence of NEC was 3.3-fold higher in Ureaplasma-positive (14.6%) than Ureaplasma-negative (4.4%) infants ≤28 weeks (OR 3.67, 95% CI 1.36 to 9.93, p=0.01). Cord blood IL-6 and IL-1β were also significantly higher in Ureaplasma-positive NEC infants compared with Ureaplasma-negative NEC infants.7The presence of higher cytokine levels in NEC infants is similar to findings in prior studies that reported higher serum levels of cytokines and chemokines in patients with NEC than in unaffected preterm infants.29 Thus, as suggested by the sheep intrauterine infection model,8 IL-1 signalling is likely involved in ureaplasma-mediated intestinal injury.
Ureaplasmal invasive disease
Ureaplasma spp. have also been detected in blood, cerebrospinal fluid (CSF) and brain tissue, suggesting the potential for invasive disease. In two prospective US cohorts9 ,30 and one Brazilian cohort,15 Ureaplasma spp. were detected in 12.6%–23.6% cord blood, venous blood and/or CSF. Invasive disease was associated with antenatal infection/inflammation (eg, clinical and histological chorioamnionitis, elevated cord IL-6 and IL-1β concentrations). In our study of invasive ureaplasma infection, the risk of severe IVH (≥Grade III IVH) was 2.5-fold higher in serum ureaplasma PCR-positive than PCR-negative infants, but ureaplasma detection in CSF was not associated with cranial ultrasound abnormalities.9 Association with adverse outcomes were not noted in the other two studies.
The ureaplasmas have been detected in CSF of preterm and term infants evaluated for sepsis/meningitis or hydrocephalus.11 Although ureaplasmas have been detected in 0.2%–9% CSF from preterm infants in prospective series, most infections are asymptomatic and CSF parameters are often normal.2 However, in one small series, six of eight infants with ureaplasma-positive CSF had severe IVH complicated by posthaemorrhagic hydrocephalus or death.31
Ureaplasma-mediated brain injury is likely due to cytokine activation of the central nervous system immune response. There was a 5-fold increased risk for severe IVH in the presence of combined ureaplasma-positive serum and elevated serum IL-1β, suggesting a potential link between invasive ureaplasma, cytokinemia and neonatal brain injury (see figure 2).2 Experimental intrauterine infection models provide further evidence in support of this contention. In murine intrauterine U parvum infection model, microglia activation, delayed myelination and disturbed neuronal development were observed in fetal and neonatal brains.32 In antenatal U parvum-exposed immature rhesus macaques, 20% of CSF and fetal brains were culture positive, but immunohistological analyses were not performed.26 Further studies in these models are warranted to better understand the mechanism of ureaplasma-mediated brain injury and to evaluate potential therapeutic interventions.
Long-term outcomes of perinatal ureaplasma exposure
The effect of perinatally acquired Ureaplasma spp. infection on long-term outcomes of preterm infants has not been adequately studied. However, Ureaplasma spp. respiratory tract colonisation has been proposed as a causative factor in reactive airway disease in young children. Isolation of ureaplasmas from the upper respiratory tract in infants and children less than 3 years of age has been associated with wheezing.2 Maternal Ureaplasma spp. vaginal colonisation during pregnancy was associated with a 2-fold increased risk for infants wheezing defined as one or more hospitalisations for asthma in the first 3 years of life.2 At 2 years of age, infants born <33 weeks gestation who were exposed to intrauterine ureaplasma infection had higher rate of cerebral palsy and lower psychomotor development index scores on the Bayley Scales of Infant Development at 2 years adjusted age compared with non-exposed infants.12 Studies of potential therapeutic interventions for perinatal ureaplasma exposure will need to include long-term pulmonary and neurodevelopmental assessments.
Ureaplasma–host interactions
Ureaplasma spp. virulence factors
Although the Ureaplasma serovars are considered commensals in the adult genitourinary tract, potential virulence factors have been identified.33 Although IgA protease and phospholipase A1, A2 and C that were identified previously by functional and enzymatic assays of Ureaplasma serovars, have been proposed as virulence factors,34 ,35 no genes in any of the 14 ureaplasma serovar genomes (American Type Culture Collection)36 and previously sequenced clinical U parvum serovar 3 genome37 were similar to known sequences for these proteins. Recent attempts to detect phospholipase C activity in U parvum serovar 3 and U urealyticum serovar 8 were unsuccessful.36 Ammonium hydroxide formed by the reaction of water in tissues with ammonia generated by urea hydrolysis may contribute to mucosal injury and inflammation,38 but this mechanism has not been demonstrated experimentally.
The multiple-banded antigen (MBA) is a surface lipoprotein that is the predominant pathogen-associated molecular patterns detected by the host immune system and has been proposed as the major ureaplasma virulence factor. The MBA consists of an N-terminal conserved domain containing a signal peptide, lipoprotein attachment site and one transmembrane domain and a C-terminal variable domain consisting of tandem repeating units. Phase variants (loss of MBA expression) have been generated in vitro with selective pressure by serial transfer in media containing polyclonal antibodies,39–41 but have not been demonstrated in vivo. In contrast, size variation of the ureaplasmal MBA has been demonstrated in vitro42 and in vivo.38 ,41 ,43 It may be the major mechanism through which the organisms evade host defences, thus preventing eradication. In the sheep intrauterine infection model, MBA protein/mba gene size variants were detected in infected amniotic fluid and fetal lung with chronic infection (69 days), but few or no size variants were detected 3–7 days postinoculation, suggesting interaction with the host immune system is required to stimulate MBA size variation.38 MBA size variation did not correlate with chorioamnionitis severity in the sheep model, suggesting that difference is the host immune response may be important in ureaplasma pathogenicity.
Recently, we reported that most Ureaplasma spp. clinical respiratory isolates from preterm infants and laboratory reference strains have the capacity to form biofilms in vitro, but biofilm formation did not impact susceptibility of respiratory isolates to azithromycin or erythromycin.4,4 Biofilm formation in vivo may protect the organisms from host defences and antibiotics.
Host immune response
Ureaplasma infection-induced stimulation of inflammatory cytokines may be the causative link between intrauterine infection and organ injury. The role of inflammatory mediators in BPD and NEC pathogenesis has been well-described. Ureaplasma spp. stimulate release of TNF-α, IL-1β, IL-8, monocyte chemoattractant-1, TGFβ1 and other mediators by various cell types in vitro and Ureaplasma spp. colonisation is associated with increased concentrations of these cytokines in tracheal aspirates during the first week of life in infants who develop BPD.33 Fetal inflammatory responses including increased cord IL-1β and IL-6 in ureaplasma-positive infants are associated with multiple morbidities including NEC and IVH.7 ,9 Upregulation of these cytokine networks leads to inflammatory cell recruitment and activation, local tissue injury and alterations in normal developmental pathways during critical periods of development.33
Diagnostic methods
Culture methods
Since Ureaplasma species hydrolyse urea and use it for a substrate for ATP generation, the organisms require media containing urea such as 10B broth and A8 agar.1 The broth colour will change from yellow to pink, indicating pH change due to urease activity in the absence of turbidity. The ureaplasma colonies are visible with a stereomicroscope within 2–3 days on A8 agar and are identified by their characteristic brown appearance in the presence of the CaCl2 indicator. Since these organisms are susceptible to desiccation and are sensitive to temperature changes, specimens should be directly inoculated into 10B broth, Copan's Universal transport media or routine Bacteriology Transport media for transport on ice to the laboratory. In experienced laboratories, the detection limit for culture methods is 100–1000 viable organisms.
PCR
PCR is more sensitive than culture for detection (<100 genome copies) of nonviable as well as viable ureaplasmas. The most commonly used gel-based traditional and real-time PCR protocols target the common mba, urease or 16s RNA genes.1 ,19 Since it was recently recognised that horizontal gene transfer of mba genes among strains within an isolate can occur, the mba gene is not recommended as a target for serovar differentiation.36 However, it is not necessary to identify the specific species/serovar for clinical purposes.
Therapeutic considerations
Pregnancy interventions
Although antibiotic therapy is standard of care for preterm premature rupture of membranes management, usual antibiotic regimens fail to eradicate ureaplasmas or diminish the inflammatory response in the amniotic cavity. Recently, Grigsby et al45 demonstrated in an experimental U parvum intra-amniotic infection in rhesus macaques that azithromycin alone or in combination with anti-inflammatory agents, dexamethasone and indocin, prevent fetal lung injury and prolong pregnancy, but do not reduce acute chorioamnionitis. Whether this approach will be beneficial to prevent other ureaplasma-mediated neonatal injuries is unknown.
BPD prevention
It is currently unknown whether eradicating Ureaplasma spp. from the preterm respiratory tract with appropriate antibiotic therapy will prevent ureaplasma infection-mediated lung injury. Despite in vitro susceptibility of Ureaplasma spp. to erythromycin46 and favourable pharmacokinetic (PK) activity,47 trials of erythromycin therapy in ureaplasma-colonised preterm infants have failed to demonstrated efficacy to prevent BPD48 ,49 or to eradicate respiratory tract colonisation.50 More recent studies have focused on the potential benefit of the new 14-member macrolides and the 15-member azalides because of their anti-inflammatory properties and favourable Ureaplasma in vitro susceptibilities. The efficacy of azithromycin and related macrolide, clarithromycin, to prevent BPD has been assessed in single-centre studies of at-risk preterm infants,51 ,52 but the safety and optimal dosing regimens for these antibiotics have not been determined in appropriate PK and pharmacodynamic studies.
Although these drugs have been safely used in the paediatric population, a recent retrospective study of a large Tennessee Medicaid cohort detected a small absolute increased risk of cardiovascular death (HR, 2.88; 95% CI 1.79 to 4.63) in adult patients who took a 5-day course of azithromycin compared with individuals who took no antibiotics.53 In an independent analysis of the data, the US Food and Drug Administration found that the overall finding of excess risk of cardiovascular death in the azithromycin treated patients was valid and that the excess risk of cardiovascular death, especially of sudden death, is consistent with arrhythmias from drug-related QT interval prolongation. Since prolonged QT interval is rare in newborns, the implications of this study for azithromycin use in the paediatric population are unclear. However, it underscores the importance of careful evaluation of safety and PKs/pharmacodynamics of azithromycin in Phase I and II studies prior to large-scale Phase III trials or introduction into clinical practice.
We have completed a Phase I open-label, PK study characterising the single-dose PK, safety, tolerability and biological effects of 10 and 20 mg/kg IV azithromycin in mechanically ventilated 24–28 weeks gestation preterm neonates who are at high risk for Ureaplasma spp. respiratory tract colonisation and BPD.54 ,55 A two-compartment structural model with the clearance and volume of peripheral compartment (V2) allometrically scaled on body weight best described the population PK of azithromycin in preterm neonates. The single 10 and 20 mg/kg dose regimens were safe, but did not suppress pulmonary inflammatory responses. The 10 mg/kg single dose was insufficient for ureaplasma clearance, but there were no treatment failures in the 20 mg/kg group. PK simulations indicate that even multiple dose administration of 10 mg/kg azithromycin would be inadequate to maintain azithromycin plasma concentrations above the ureaplasma MIC50, while multiple doses of 20 mg/kg might provide a favourable AUC24/MIC90 ratio.
References
Footnotes
-
Funding This work was supported by the National Institutes of Health grant numbers HL07113, HL087166 and HD056424.
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed.