Article Text

Abstract
Objective To evaluate the usefulness of a single C-Reactive Protein (CRP) measurement at 18 h of age to identify neonates where antibiotics started for possible early onset sepsis (EOS) could safely be discontinued.
Design/Methods In a prospective cohort of 647 preterm (<35 weeks) and 555 late preterm (35–36 weeks) or term newborns with maternal and/or neonatal risk factors for EOS, CRP levels were measured between 15 and 21 h of age.
Results There were 16, 107 and 1079 neonates with proven EOS, possible EOS and no EOS, respectively. Among the 645 neonates with a CRP<10 mg/L, 1 had proven EOS, 43 had possible EOS and 601 (93.2%) were not infected. All with possible or proven EOS were either less than 35 weeks’ gestation, symptomatic at the time of CRP assessment or remained on antibiotics because of maternal bacteraemia: they would therefore not be considered for discharge. There were 557 neonates with a 18-h CRP≥10 mg/L. Of these, 15 had proven EOS, 64 had possible EOS, and 478 (85.8%) were not infected. Sensitivity and specificity of 18-h CRP for proven or possible EOS were 64% (95% CI 56 to 73) and 56% (95% CI 53 to 59), respectively. The negative predictive value was 93% (95% CI 91 to 95), and the positive predictive value was 14% (95% CI 11 to 17).
Conclusions The duration of antibiotic treatment in neonates born beyond 34 weeks’ gestation and asymptomatic at the time of CRP assessment could be potentially reduced with a diagnostic algorithm that includes a point-of-care 18-h CRP measurement. An elevated 18-h CRP in isolation should not be used as a reason to prolong antibiotics.
- Newborn
- C-reactive Protein
- Early-onset Neonatal Sepsis
- Preterm Infant
- Antibiotics
Statistics from Altmetric.com
Introduction
Early Onset Sepsis (EOS) is a frequent condition (1–20 infants per 1000 live births) responsible for an important fraction of neonatal morbidity and mortality.1 ,2 When EOS is suspected at birth on the basis of symptoms or risk factors, empiric antibiotics are initiated before the causative agent is identified. These are usually continued for 48–72 h, at which time 97–98% of cultures ultimately yielding a pathogen are positive.3 ,4 Antibiotics may be continued longer if the infant was ever symptomatic as intrapartum antibiotics can result in falsely negative blood cultures. It is estimated 4–10% of all newborns have at least one evaluation for suspected EOS, and more than 5% of all newborns receive systematic antibiotics within the first week after birth.5 This approach results in treatment of as many as 30 uninfected infants for every one who is eventually determined to be infected, and the combination of evaluation and treatment of these uninfected infants accounts for approximately 25% of all neonatal intensive care unit (NICU) days.5–7 There are also parental emotional consequences to this approach, including anxiety and mother-infant separation, which may interfere with establishment of breast feeding. Unnecessary use of antibiotics may ultimately increase the incidence of multiresistant micro-organisms, and favour the subsequent development of allergy and asthma.8 Furthermore, decreases in the biodiversity of the microbiome induced by antibiotics have been linked to obesity, inflammatory bowel disease, and Clostridium difficile infection.9
There have been many attempts to develop reliable diagnostic tools to rule out EOS.10–12 Many studies have reported results of the use of C-reactive protein (CRP) measurement for this purpose.13–19 CRP is produced by the liver in response to inflammatory cytokines. The normal level in newborn infants is 2–5 mg/L with there being consensus that 10 mg/L is the upper limit of normal.18 In EOS, CRP levels at the time of initial evaluation have a low sensitivity (less than 40%) and low negative predictive value. This low sensitivity of very early CRP is because EOS usually originates during labour or at delivery, and it then takes 6–12 h for CRP to rise.19 CRP does not cross the placenta, so maternal CRP does not contribute.19 Although the sensitivity of a normal CRP at less than 12 h of age is not sufficiently high to justify withholding antibiotics, two CRP levels <10 mg/L at the time of evaluation and 24 h later (as advocated in the UK National Institute for Health Care Excellence (NICE) guidelines) indicate that EOS is extremely unlikely.16–18 ,20 We investigated whether a single CRP measurement at 18 h of age could identify a group of infants where antibiotics could safely be discontinued, potentially hastening discharge.
Patients and methods
The study was conducted over 3 years (2006–2009) at the neonatal intensive care unit of the referral tertiary centre for Northern and Central Alberta (Royal Alexandra Hospital) and the special care nursery of the two largest community hospitals in the Edmonton Region. Babies were eligible for the study if a written informed consent was obtained, and at least one of the following inclusion criteria was met: (1) gestational age (GA) below 37 weeks with either spontaneous preterm labour or preterm and prelabor rupture of the membranes; (2) GA≥35 weeks with positive maternal Group B Streptococcus (GBS) screening and inadequate perpartum antibiotic prophylaxis; (3) any GA with prolonged rupture of the membranes (more than 18 h) or clinical chorioamnionitis. Exclusion criteria included major fetal anomaly previously detected on ultrasound examination, non-bacterial congenital infection, or maternal refusal or inability to provide consent. All newborns were enrolled before 18 h of age. The study was approved by the Health Research Ethics Board of the University of Alberta, Edmonton.
Infants had proven EOS if the blood culture drawn as part of the initial sepsis work-up was positive for a bacterial pathogen. Blood cultures positive for normal skin flora were considered to be contaminants. Infants had possible EOS if (1) they were born to mothers who received intrapartum antibiotics and (2) antibiotics were started on the day of birth and continued for greater than 72 h despite negative culture. All other infants were considered to be not infected.
CRP levels were determined on a blood sample (0.8 mL) drawn between 15 and 21 h of age. This timing was chosen hoping that results could be used in a future algorithm that would expedite discharge by 24 h of age. The analysis was carried out on Vitros 950/250 instrumentation (Ortho Diagnostics, Johnson and Johnson). The point-of-care method is an immunorate format based on an enzymatic heterogeneous sandwich immunoassay. The threshold was set to 10 mg/L.18 Prior to and during the study, CRP measurements for routine neonatal care were not used at the three institutions. All healthcare providers were kept unaware of the CRP results during the entire study period.
Data were summarised by frequency and percent or mean and SD. Groups were compared using χ2 and adjusted χ2 tests for maternal and infant variables, respectively.21 Adjusted t tests compare group means for infant variables. Diagnostic test characteristics were reported with 95% CIs.
Results
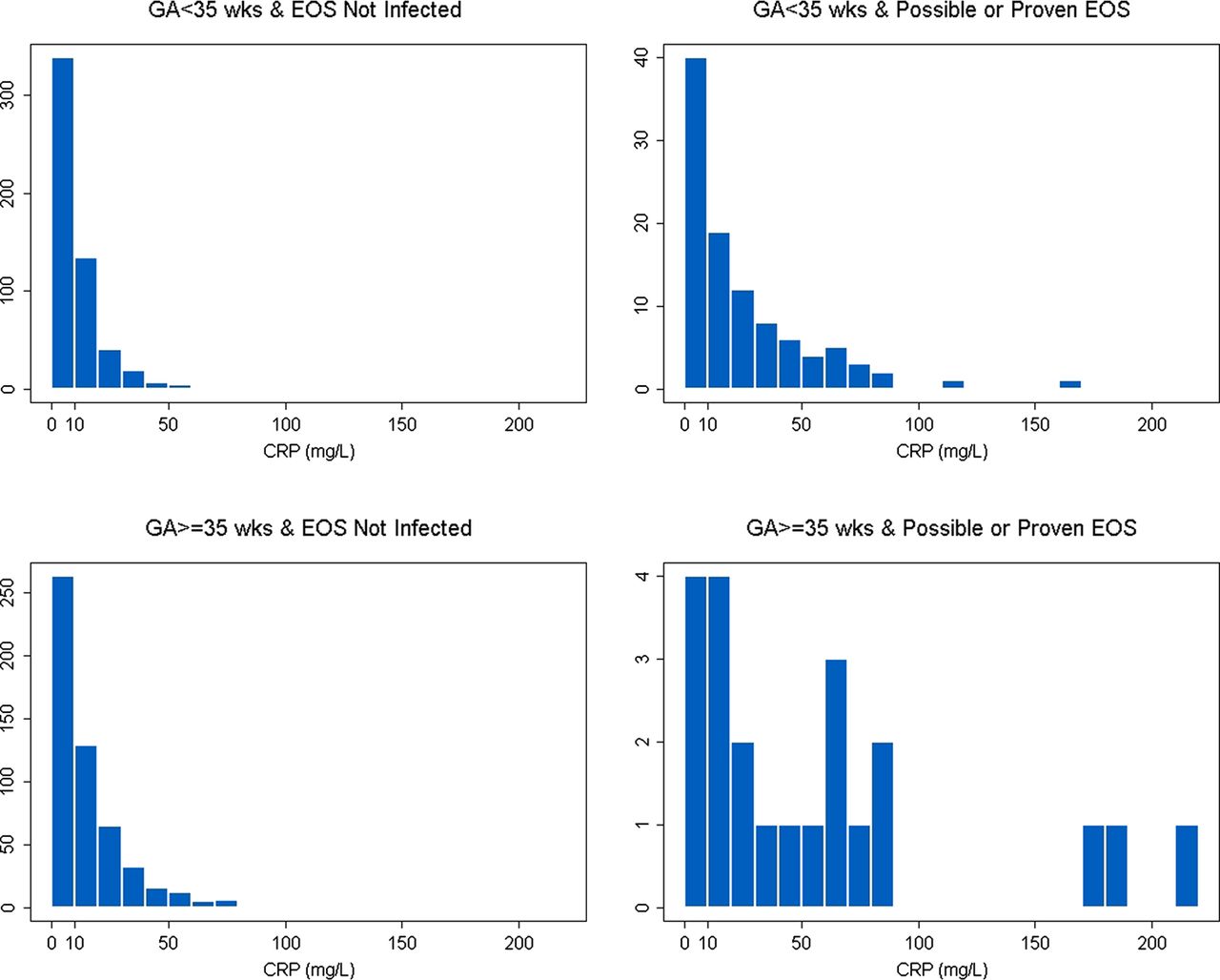
Table 1 shows the characteristics of the 1107 mothers and their 1202 neonates (647 preterm <35 weeks and 555 late preterm (35–36 weeks) or term). There were 16, 107 and 1079 neonates with proven EOS, possible EOS and no EOS, respectively. Table 2 shows the pathogens isolated from neonates with proven EOS: Escherichia coli accounted for 11 of the 16 cases. Figure 1 shows the 18-h CRP distribution according to GA and EOS diagnosis.
Maternal and neonatal characteristics
Identification of pathogens for infants with septicemia*
{kind=link}
18-h C-reactive protein (CRP) distribution according to gestational age (GA) (<35 and ≥35 weeks) and early onset sepsis (EOS) diagnosis (ruled out and possible or proven).
Among the 645 neonates with a CRP<10 mg/L, 601 were not infected. Of the remaining 44 neonates, one had proven EOS and 43 had possible EOS: all were either less than 35 weeks’ GA or symptomatic at the time of the CRP assessment, with the exception of one asymptomatic infant who was continued on antibiotics as the mother was bacteraemic (table 3). Therefore, they would not be considered for early discharge. With the exception of this subject, all infants (n=189) older than 34 weeks' gestation, asymptomatic within 18 h of age, and with CRP<10 mg/L, were not infected.
18-h CRP distribution according to GA (<35 and ≥35 weeks), EOS diagnosis (proven, possible, or not infected) and the composite variable ‘symptomatic or not’
There were 557 neonates with a 18-h CRP≥10 mg/L. Of these, 15 had proven EOS, 64 had possible EOS, and 478 were not infected.
Sensitivity and specificity of 18-h CRP for proven or possible EOS were 64% (95% CI 56% to 73%) and 56% (95% CI 53% to 59%), respectively. The negative predictive value was 93% (95% CI 91% to 95%), and the positive predictive value was 14% (95% CI 11% to 17%).
Discussion
The current study shows that a CRP measured at approximately 18 h of life has a sensitivity of only 64% for detecting combined possible and proven EOS. One reason for this low sensitivity may be misclassification of uninfected neonates born in the face of intrapartum antibiotics as having possible EOS. A further explanation is that it may take longer than 18 h for the CRP to rise in an infected preterm neonate.22
All neonates born beyond 34 week's gestation, asymptomatic at 18 h of age, and with a CRP<10 mg/L met our definition of ‘not infected,’ with the exception of one infant classified as possible EOS as antibiotics were continued because the mother was bacteraemic. If these findings were validated in a subsequent study, it is possible that they could constitute criteria for discontinuing antibiotics earlier (24 instead of 48–72 h) and possibly considering discharge at 18–24 h of age.
The positive predictive value of elevated CRP for possible or proven EOS has consistently been shown to be low (only 14% in the current study), mainly because there are multiple conditions associated with an inflammatory reaction in the perinatal period, including a complicated labour and delivery, meconium aspiration syndrome, animal-derived surfactant administration, intraventricular haemorrhage and tissue injury.18 ,22 It is vital that clinicians recognise that an elevated 18-h CRP in isolation should never be used as a reason to prolong antibiotic therapy.
There is increasing interest in use of Il-6, IL-8 mannose-binding lectin, and procalcitonin levels alone or in combination with molecular, proteomic and genomic diagnostics to rule out EOS.23 One advantage of CRP over other biomarkers is that point-of-care testing is commercially available. Ideally, a test would be performed at birth with results available within 1 h, so that antibiotics could be avoided. Until such a test is described, use of CRP<10 mg/L at 18 h for early discharge of asymptomatic late preterm or term neonates appears to be a potentially useful strategy.
Acknowledgments
Dr Rosychuk is salary supported by Alberta Innovates—Health Solutions (Edmonton) as a Health Scholar. We thank Barbara Kamstra, Athaide Melba, Donna Morstad, Heather Rylance and Shirley Beauchamp, research nurses at the three institutions, who obtained consent and successfully enrolled 1107 mothers in the study.
References
Footnotes
-
Contributors All authors contributed to this manuscript's conception and design, analysis and interpretation of the data, drafting the article or revising it for important intellectual content and finally approving the final version to be published.
-
Funding An Innovation Grant from the Royal Alexandra Hospital Foundation (Edmonton, Alberta).
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Health Research Ethics Board of the University of Alberta, Edmonton.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Fantoms