Article Text

Abstract
Background Premature newborns often experience oxygen saturations outside policy-specified targets, which may be associated with increased morbidity. Nurse workload may affect oxygen management.
Objective To examine the relationship between number of patients assigned to neonatal intensive care unit (NICU) nurses and achievement of oxygen saturation goals in premature newborns.
Design The authors linked nurse–patient assignment data with continuous oxygen saturation data for infants <29 weeks' gestation in a single NICU between January and June 2008. The proportion of time oxygen saturation was in policy-specified target range (85–92%) and proportion of time hyperoxaemic (98–100%) were determined for multiple 6 h monitoring periods. Each period was characterised by a single nurse, respiratory support mode and fraction of inspired oxygen (Fio2) level (0.22–0.49 or ≥0.5). The nurse:patient ratio for the infant's nurse for each monitoring period was determined. Factors associated with Spo2 target achievement and hyperoxaemia were identified.
Results The authors analysed 1019 monitoring periods from 14 infants with a mean (SD) birth weight of 860 (270) g and gestational age of 26.6 (1.6) weeks. The mean (range) postmenstrual age for all monitoring periods was 31.6 (24.1–40.7) weeks. Eighty-seven nurses provided care. In a multivariate cross-classified hierarchical regression, the nurse:patient ratio, postmenstrual age, respiratory support mode and Fio2 were significantly associated with oxygen saturation outcomes. Fewer patients per nurse was significantly associated with a higher saturation target achievement among patients on high-frequency ventilation, and with reduced hyperoxaemia among patients on nasal cannula.
Conclusions Fewer patients per nurse may be associated with improved achievement of oxygen saturation goals and may be an important modifiable factor influencing oxygen-related outcomes in premature newborns. This effect may vary with mode of respiratory support.
Statistics from Altmetric.com
Introduction
Recent cohort studies suggest that targeting lower rather than higher oxygen saturation (Spo2) ranges in premature infants may reduce the incidence and severity of retinopathy of prematurity (ROP) and bronchopulmonary dysplasia (BPD), without increasing adverse outcomes.1,–,5 Two randomised controlled trials have demonstrated that Spo2 targets of 89–94% and 91–94% are beneficial and safe in very-low-birth-weight (VLBW, <1500 g) infants with established ROP or lung disease, respectively.6 7 Prospective international trials are under way to determine whether Spo2 targets in the mid-high 80s compared with the low 90s starting from birth will improve outcomes for VLBW infants.
What is already known on this topic
▶ Implementation of policies to target oxygen saturations in very-low-birth-weight infants is associated with reductions in retinopathy of prematurity and chronic lung disease.
▶ Achievement of policy-specified target is highly variable among centres, among infants within centres and within infants over time.
What this study adds
▶ The number of patients cared for by a nurse is a significant modifiable factor affecting precision of oxygen management in the NICU.
▶ Respiratory support mode modifies the effect of nurse:patient ratio on oxygen saturation target achievement.
In practice, achievement of policy-specified oxygen saturation targets is highly variable and limited by many factors. Spo2 target achievement varies among neonatal intensive care units (NICUs), among infants within NICUs and for individual infants over time.8 This variation does not appear to be due to differences in biological factors such as birth weight or admission illness severity (IS), suggesting that factors involving NICU infrastructure or personnel play an important role in achievement of Spo2 goals. Indeed, clinically important variation among nurses regarding Spo2 goals and compliance with oximeter alarm guidelines has been documented.9 10 Identifying factors such as these, and developing methods for improving the precision of oxygen management, is increasingly of interest in neonatal intensive care.
Among factors potentially influencing achievement of oxygen saturation targets, no study has examined in detail the relationship between Spo2 in VLBW infants and nurse workload. We hypothesised that achievement of oxygen saturation goals will decrease with increasing number of assigned patients per nurse. In order to test this hypothesis, we designed this study with the following objectives: (1) to examine the relationship between the number of patients simultaneously cared for by nurses (individual nurse:patient ratio), and proportion of time VLBW infants achieve Spo2 within policy-specified target range, as well as proportion of time with hyperoxaemic Spo2 (98–100%); and (2) to identify infant and nurse factors associated with Spo2 target achievement and hyperoxaemia exposure, adjusted for individual nurse:patient ratio.
Methods
This was a single-centre retrospective observational study linking existing quality improvement (QI) oximeter data with NICU nurse administrative data and bedside patient flow sheets at Connecticut Children's Medical Center. Institutional Ethics Review Board approval was obtained for this study.
Oximeter data
As part of a QI initiative, oximetry data were collected January–June 2008 from a convenience sample of newly admitted VLBW infants. Using Masimo Radical 7 SET oximeters (Masimo Corporation, Irvine, California), Spo2 values were collected every 2 s during routine bedside oximetry monitoring throughout the infant's hospitalisation. Infants who were moribund on admission or did not survive 96 h (the age at first oximeter download) were not included in the QI initiative. Oximeter data were not included for care performed away from the bedside.
Infants
VLBW infants <29-week gestation were included in this study if they had QI oximeter data available. For multiple gestations, only the infant with the greatest amount of oximeter data was included.
Nurse–patient assignment data
In order to examine nurse and patient assignment factors, we examined the achievement of target range and hyperoxaemic time for individual infants within single nurse work shifts. Information from daily nurse–patient assignment sheets was linked to the infant's QI oximeter data, including the infant's nurse during each shift and number of other patients assigned to the infant's nurse during that shift.
In the Connecticut Children's NICU, in order to facilitate nurse–patient assignments, patients are assigned at the beginning of each shift to one of three IS categories: High, Medium and Convalescent. Patients in the Medium IS category include those receiving high-frequency oscillator (HFOV) or synchronised intermittent mandatory ventilation (SIMV), continuous positive airway pressure (CPAP), nasal cannula (NC) ≥2 l/min, vasoactive medications, NPO status or care for invasive lines, chest tubes, postoperative status or unstable cardiorespiratory status. Patients meeting Medium IS criteria may be categorised as High IS if they require especially frequent assessments and interventions for labile cardiorespiratory and/or neurological status. Convalescent IS infants are those not meeting these criteria. Typically, nurses caring for High IS infants have no other assigned patients (nurse:patient ratio 1:1), while nurses caring for Medium IS infants may have one or two other patients (nurse:patient ratio 1:2–3), and nurses caring for Convalescent IS infants may have two or three other patients (nurse:patient ratio 1:3–4). However, NICU census or staff availability may result in assignment of more or fewer patients than is usual for the infant's assigned category.
Unit of analysis: monitoring periods
Monitoring periods within single nursing shifts were the primary unit of analysis. Oximetry data from immediately before and after shift changes were excluded to avoid overlap in patient care givers, resulting in a maximum monitoring period duration of 6 h. Such monitoring periods met inclusion criteria if: the infant received care from one nurse, and continuously received supplemental oxygen via a single respiratory support mode. Monitoring periods were included only if they preceded documentation of mature retinal vascularisation or laser retinal ablation, and were excluded if the assigned nurse or respiratory support could not be determined.
For each monitoring period, data collected included date, IS category, study ID of the infant's nurse and the nurse's number of assigned patients (nurse:patient ratio). Respiratory support and fraction of inspired oxygen (Fio2) (as read from the bedside oxygen blender), recorded hourly by the bedside nurse, were linked to the oximeter data. Respiratory support modes were HFOV, SIMV, CPAP and NC. In addition to the individual nurse:patient ratio for the infant's nurse, the NICU-level nurse:patient ratio (nurses working that shift/NICU census that shift) was also determined.
During the course of their hospitalisation, each study infant accumulated multiple monitoring periods. Varying numbers of monitoring periods were analysed for each infant, with monitoring periods from varying postmenstrual ages (PMA). A given nurse may have provided care during several monitoring periods for different infants at different times. Thus, monitoring periods were clustered within individual infants, and were also clustered within individual nurses.
Data analysis
The primary outcome, Spo2 target achievement, was defined as the proportion of time during a monitoring period that the infant's Spo2 was between 85 and 92%, the NICU's goal for oxygen management in infants born <29 weeks' gestation. Hyperoxaemic time was the proportion of a monitoring period where Spo2 was between 98 and 100%.11
Descriptive, univariate and multivariate analyses were performed. Regression analyses were performed with cross-classified random effects hierarchical modelling to adjust for the two-way clustering in this data set.12 Univariate comparisons of factors correlated due to clustering were accomplished with cross-classified hierarchical regression in which the factor of interest was the sole factor entered. Multivariable modelling used backward selection from among a priori selected factors.
Results
Fourteen infants met the inclusion criteria with a mean (SD) gestation of 26.6 (1.6) weeks and birth weight of 860 (270) g. Five infants (36%) were white, three (21%) black and four (29%) Hispanic. Eleven (79%) were male, and 12 (86%) received antenatal steroids. The median number of monitoring periods/baby was 60 (interquartile range, 33–117). Eighty-seven nurses provided care. The median number of monitoring periods/nurse was seven (2–16). The individual nurse:patient ratio ranged from 1:1 to 1:4 among the monitoring periods. The mean (SD) NICU-level nurse:patient ratio during the monitoring periods was 1 nurse to 2.38 (0.18) patients. Eleven monitoring periods were excluded owing to missing or ambiguous data.
Oxygen saturation outcomes were examined for 1019 monitoring periods (table 1). The median monitoring period duration was 359 min (354–360). The mean PMA for monitoring periods was 31.6 weeks (range 24.1–40.7 weeks). The mean PMAs for independent variable subgroups are provided in table 1. The overall median monitoring period Spo2 target achievement was 16.1% (8.7–27.3), hyperoxaemic time 22% (8.1–44.2), time below target (Spo2 <85%) 3.1% (1.5–6.2) and time with Spo2 93–97% 48.3% (35.2–59.2).
Characteristics of monitoring periods
In a univariate cross-classified hierarchical regression, target achievement decreased significantly, and hyperoxaemic time increased with assignment of a second patient to the infant's nurse (nurse:patient ratio 1:2) compared with monitoring periods where the monitored infant was the only assigned patient (nurse:patient ratio 1:1, figure 1). The target achievement decreased, hyperoxaemic time increased and proportion time with Spo2 <85% decreased with addition of a third or fourth patient (nurse:patient ratio 1:3+) compared with two patients. There was no significant correlation between NICU-level nurse:patient ratio and target achievement.
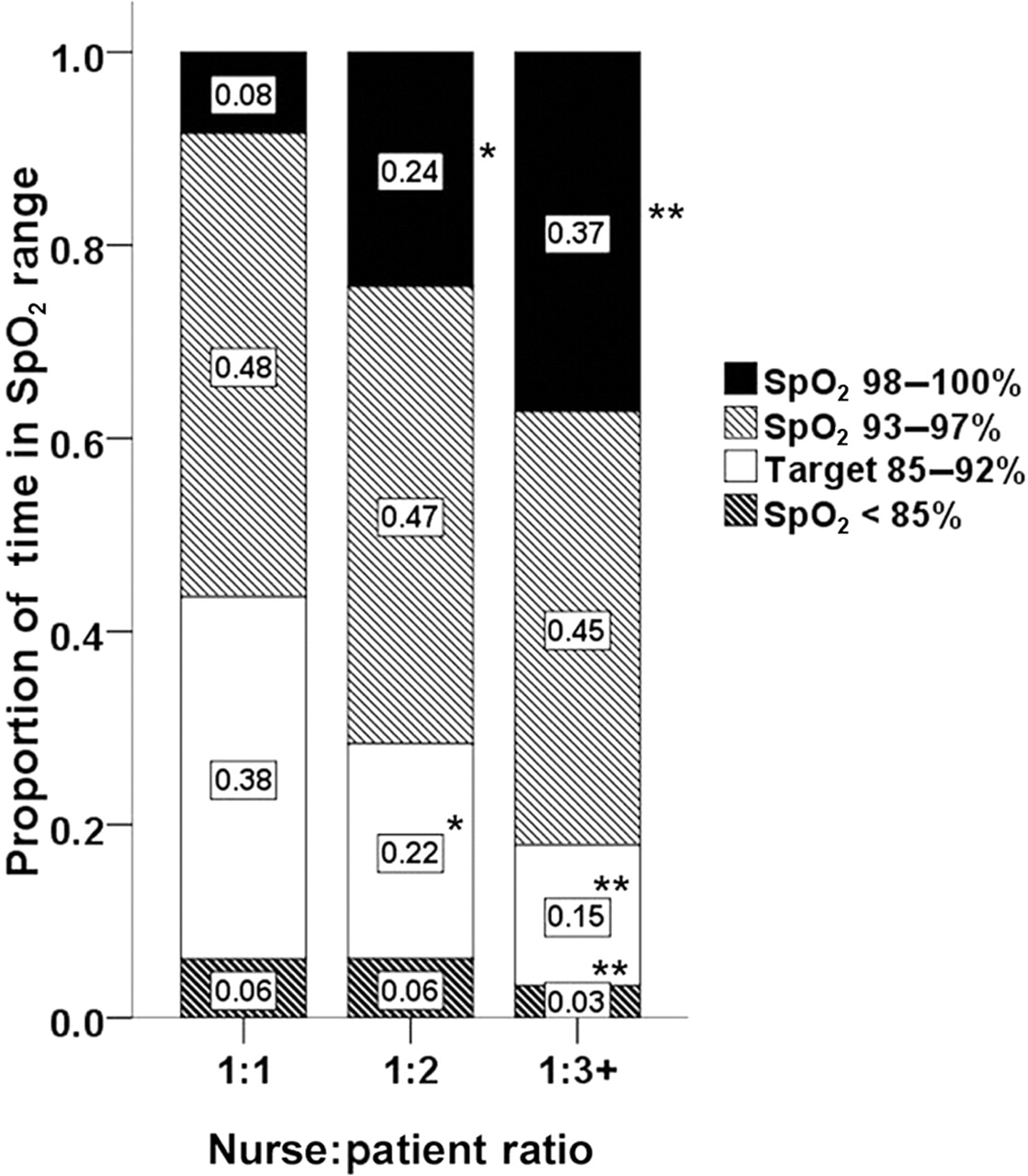
Mean proportion of time in specified oxygen saturation (Spo2) ranges, by nurse:patient ratio. *p<0.001, comparison group=1:1. **p<0.001, comparison group=1:2.
The median target achievement fell from 38.5% for High IS monitoring periods to 18.2% for Medium IS (p<0.001 compared with High IS) and 6.3% for Convalescent IS (p<0.001 compared with Medium IS). The median hyperoxaemic time increased from 1.1% for High IS monitoring periods to 19.2% (p<0.001) for Medium IS and 55.7% (p<0.001) for Convalescent IS. The median time with Spo2 <85% was not different among High IS (3.6%) and Medium IS (3.8%) but was significantly lower for Convalescent IS monitoring periods (1.7%, p<0.001). Within IS categories, there was a visual trend toward reduced target achievement and increased hyperoxaemic time with more assigned patients (figure 2).

Mean proportion of time in specified oxygen saturation (Spo2) ranges, by illness severity category and nurse:patient ratio.
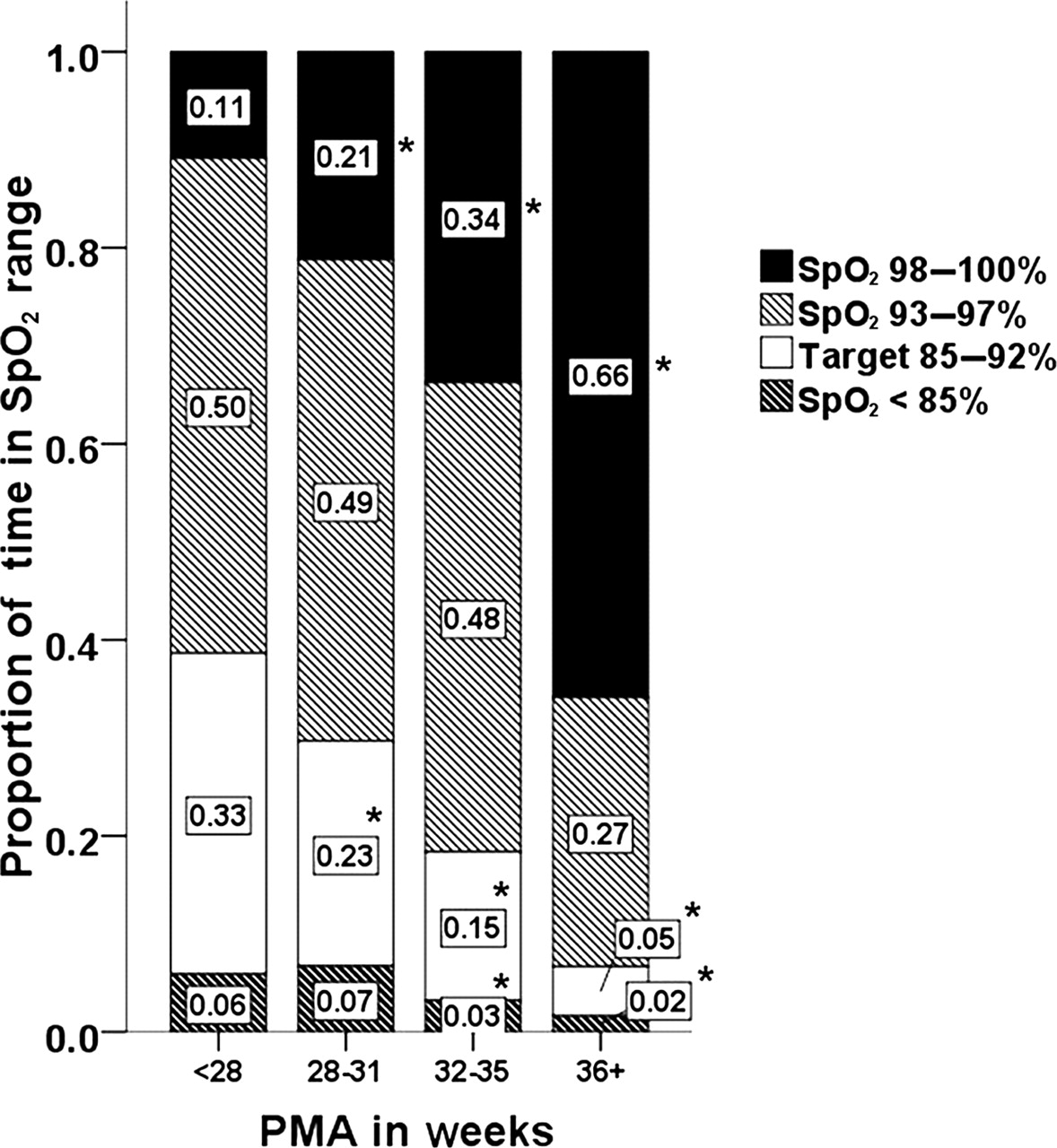
Postmenstrual age correlated significantly with both Spo2 target achievement and hyperoxaemic time (figure 3), with target achievement lower and hyperoxaemic time greater at higher PMA. The proportion of time with Spo2 <85% was significantly lower for monitoring periods after 32-week PMA.
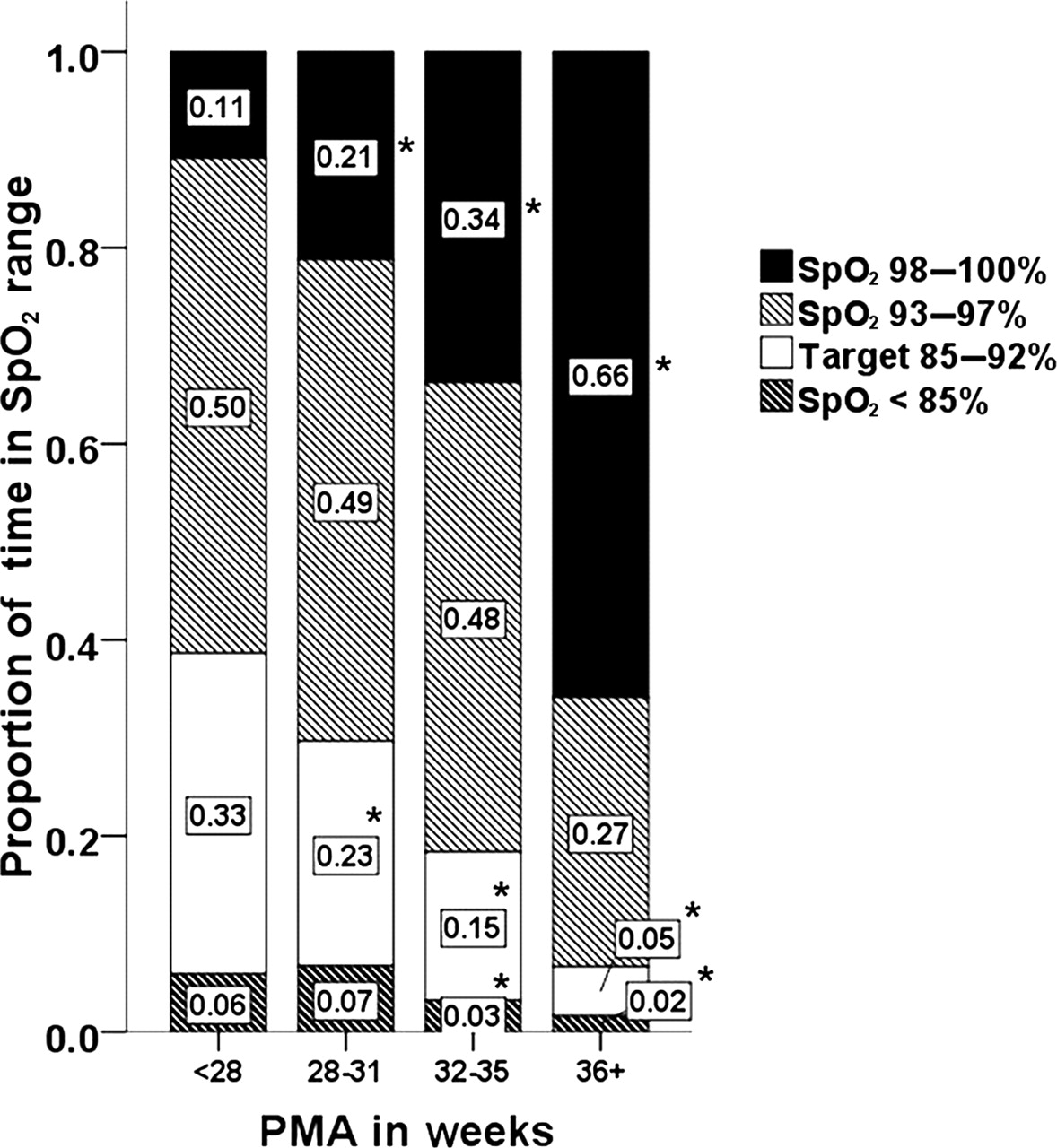
Mean proportion of time in specified oxygen saturation (Spo2) ranges, by postmenstrual age. *p<0.01, comparison group=prior postmenstrual ages (PMA) category.
The median target achievement was highest among monitoring periods on HFOV, 38.8%, and decreased with less aggressive respiratory support: 21.9% on SIMV, 20.5% on CPAP and 8.8% on NC (p<0.001 for all groups compared with HFOV). The median hyperoxaemic time increased from 1.3% on HFOV to 12.4% on SIMV, 17.6% on CPAP and 40.7% on NC (p<0.001 for all groups compared with HFOV). Within the HFOV, CPAP and NC groups, there was a visual trend toward reduced target achievement and increased hyperoxaemic time with more assigned patients (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean proportion of time in specified oxygen saturation (Spo2) ranges, by respiratory support mode and nurse:patient ratio. CPAP, continuous positive airway pressure; HFOV, high-frequency oscillator; IMV, intermittent mandatory ventilation; NC, nasal cannula.
The median target achievement was lower in monitoring periods on Fio2 ≥0.5, 0.5%, compared with 16.5% in monitoring periods on Fio2 0.22–0.49 (p<0.01). The median hyperoxaemic time was also greater in monitoring periods on higher Fio2, 97.5%, compared with 21.4% on lower Fio2 (p<0.001). Fio2 was ≥0.5 during 39 of the 1019 monitoring periods. Two distinct PMA groups were found within the Fio2 ≥0.5 subgroup: for a PMA less than 32 weeks, the median target achievement was 36.5%, and the median hyperoxaemic time was 7.6%. For a PMA of 32 weeks or greater, the median target achievement was 0.3%, and the median hyperoxaemic time was 98.7%.
Factors associated with Spo2 target achievement in multivariate cross-classified random effects hierarchical regression are listed in table 2. The reference group is monitoring periods with supplemental oxygen provided via NC. The nurse:patient ratio term tested in this model was ‘nurse caring for one patient versus more than one patient.’ The adjusted mean target achievement for the reference group at 31.6 weeks' PMA (overall mean) was 16.3%. With each incremental week's PMA, target achievement decreased 2 percentage points. Fio2 ≥0.5 was associated with a 3.9 percentage point adjusted increase in target achievement. Monitoring periods on SIMV had significantly lower adjusted target achievement, while CPAP was not significantly different from NC.
Cross-classified hierarchical models of factors significantly associated with proportion of time in target range, and proportion of time with saturation 98–100%
After adjusting for the above factors, HFOV was associated with increased target achievement; however, this effect was modified by a number of assigned patients. For monitoring periods with no other assigned patients (nurse:patient ratio 1:1), the adjusted target achievement improved by 12.8 percentage points compared with the reference group. However, for monitoring periods on HFOV with a nurse:patient ratio of 1:2+, the adjusted target achievement was significantly reduced by 8.2 percentage points compared with HFOV monitoring periods with a nurse:patient ratio of 1:1. This relationship between target achievement and number of assigned patients was not seen with other respiratory modes (figure 4).
Table 2 shows the results of multivariate regression examining factors associated with hyperoxaemic time. In contrast to the prior model, the nurse:patient ratio term tested here was ‘nurse caring for two patients versus three or more patients.’ The adjusted mean hyperoxaemic time was 26.8% at an overall mean PMA of 31.6 weeks. With each incremental week PMA, the adjusted hyperoxaemic time increased by 4.3 percentage points. Monitoring periods on NC where the nurse had three or more assigned patients (nurse:patient ratio 1:3+) were associated with a 6.2-percentage-point significant increase in hyperoxaemic time compared with NC monitoring periods where the nurse had fewer assigned patients.
After adjusting for the factors in these models, other factors were not significantly associated with target range achievement or hyperoxaemic time, including birth weight, antenatal steroid status or IS Category.
Discussion
Avoidance of hyperoxaemic Spo2 levels is associated with reduced morbidity in VLBW infants. This study found four factors significantly associated with precision of oxygen saturation management: nurse:patient ratio, postmenstrual age, respiratory support and Fio2. Confirming the study hypothesis, a smaller number of assigned patients was associated with improved Spo2 target achievement and reduction in hyperoxaemia. However, this effect varied with respiratory support mode. The nurse:patient ratio significantly influenced target achievement among patients on HFOV, and influenced the proportion of hyperoxaemic time among patients on NC.
A number of studies have shown an increased risk of mortality and morbidity associated with increased nursing workload,13 14 while other studies have found either no difference or improvements in patient outcomes.15 16 Increasing the number of assigned patients may result in less time for individual patient needs, thus increasing the risk of certain adverse outcomes. Our findings suggest that, in certain situations, fewer assigned patients promote more precise oxygen management, which may influence oxygen-related outcomes such as ROP or BPD.
In this study, target achievement decreased significantly, and hyperoxaemic saturation exposure increased with increasing PMA. A significant association between PMA and target achievement has been reported previously.8 In that study, infants with a mean gestation of 26±1.4 weeks achieved the target 50.9% of the time during the first week of life compared with 44.1% during week 4. The relationship between PMA and target Spo2 achievement partly explains the low overall target achievement of 16.1% observed in our cohort, as data were collected throughout NICU oximetry monitoring. The target achievement during the first 4 weeks of life in this study was 28%, which is within the range reported for 14 NICUs (16–60%).8 The relationship between PMA and Spo2 target achievement may reflect reduced emphasis on precise oxygen management as infants become older and less ill. It also may reflect the lack of consensus regarding duration of Spo2 targeting in premature infants.17 Recent cohort studies used varying endpoints for duration of lower Spo2 targeting, including 32 weeks' PMA, 34 weeks' PMA or the duration of supplemental oxygen.2 6 7 Current prospective trials comparing different Spo2 targets also use differing endpoints for the duration of such targeting.18,–,20 A planned prospective meta-analysis combining data from these trials may provide evidence regarding optimal duration of Spo2 targeting.
Automated feedback systems that mechanically adjust Fio2 to maintain Spo2 targets significantly increase target achievement when compared with manually adjusted Fio2, for brief periods under optimal conditions.21,–,23 Automated Fio2 control systems also reduce Fio2 adjustments by staff, which may translate into reduced nurse workload and enhanced acceptance of an Spo2 policy by NICU staff.22 23 It is noteworthy that these reports describe mechanisms that are integrated into ventilators. In this study, in which 80% of monitoring periods were not on a mechanical ventilator, achievement of Spo2 goals was significantly lower in non-ventilated infants. Automated Fio2 control systems may have greater promise for improving Spo2 targeting if such systems can be adapted for use with non-ventilator-based CPAP and NC devices.
Administration of blended Fio2 greater than 0.5 was associated with increased hyperoxaemia and increased target achievement in the multivariate analysis. This unanticipated finding may reflect the heterogeneity of the Fio2 >0.5 monitoring period group, which, in a post hoc analysis, represented either infants of low PMA with acute respiratory conditions (sepsis, postsurgery, etc) or convalescing infants on NC. A further investigation to clarify the relationships between high Fio2 and achievement of Spo2 goals in specific subgroups, perhaps using both blended and calculated effective Fio2, is warranted.
The proportion of time spent below the target range (Spo2 <85%) in this study was comparable with a recent study in which infants had Spo2 values <80% for 1.9% of the time on supplemental oxygen.24 That study reported a statistically significant increase in hypoxaemic time after a small shift downward in the Spo2 target range. Others have reported an increase in haemodynamically significant patent ductus arteriosus in extremely-low-birth-weight infants after changing policy to target lower Spo2 values, although the proportion of time below target was not measured.25 Policy changes intended to reduce hyperoxaemic time should consider the potential for increased hypoxaemic saturations.
Nurse–patient assignments and nurse:patient ratios are not random but are based in part on perceived severity of illness. Thus, IS may potentially confound the relationship between the nurse:patient ratio and achievement of oxygen saturation goals. We observed a significant association between IS (as reflected by IS category) and both target range achievement and hyperoxaemic time in univariate analysis. However, in a multivariate analysis, the IS category was not significantly associated with target achievement or hyperoxaemic time after adjusting for other factors, suggesting that IS is not significantly confounding these results. While the use of our NICU's internal IS categorisation as a proxy for IS during monitoring periods may limit the generalisability of this finding, we are not aware of any measures of neonatal IS that have been validated for following changes from shift to shift. The development of such a measure may have significant implications for nurse–patient assignment decisions in the NICU, and warrants further research.
This study documents Spo2 target achievement and hyperoxaemic saturation exposure as a function of nurse:patient ratios. By using monitoring periods obtained through repeated measurement in a wide variety of clinical circumstances as the unit of study, we were able to perform a robust analysis with a comparatively small number of patients. However, modifiable factors not included or identified in this study may also affect the precision of oxygen management, such as staff education and motivation, presence and effectiveness of an oxygen policy, oximeter alarm settings, compliance auditing and feedback practices. Optimal Spo2 target achievement in the NICU appears to require attention to these factors26 but may also require specific modifications to nurse–patient staffing algorithms. Technological advancements, such as automated Fio2 adjustment devices, may eventually lead to improved oxygen control with reductions in nurse workload.21,–,23
Important questions remain regarding targeted Spo2 and outcome in premature infants. Randomised controlled trials are under way to address the benefits and risks of high versus low saturation targets. Secondary analyses of data from these trials may shed light upon the proportion of target achievement necessary to achieve maximum benefit, proportion of target achievement feasible during routine care or duration of precise oxygen saturation management necessary to achieve optimal outcomes.
Conclusion
This study found that the nurse:patient ratio, postmenstrual age, respiratory support mode and Fio2 were significantly associated with achievement of oxygen saturation goals in VLBW infants at risk for ROP and BPD. Reducing the number of patients per nurse in certain clinical situations may result in less exposure to hyperoxaemic saturations and more time within the desired Spo2 range. Nurse:patient ratios may represent a modifiable factor influencing oxygenation-related outcomes in VLBW infants. Further research is needed to determine optimal nurse–patient assignment levels for maintaining precise oxygen management in VLBW infants, and to evaluate their effects on important outcomes such as ROP and BPD.
References
Footnotes
-
Competing interests None.
-
Ethics approval Ethics approval was provided by the Connecticut Children's Medical Center Institutional Review Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.