Article Text

Abstract
Objectives To evaluate the effects of indomethacin or ibuprofen compared with placebo on closure, morbidity and mortality in preterm infants <37 weeks' gestation with echocardiographically and/or clinically important patent ductus arteriosus (PDA) at >24 h of life.
Data sources MEDLINE, EMBASE, Cochrane Central Register of Controlled Trials, CINAHL, Cochrane Library, clinicaltrials.gov, controlled-trials.com, American Pediatric and European Paediatric Research Societies and Effective Care of the Newborn Infant.
Review methods Systematic review with network meta-analysis of randomised studies comparing intravenous indomethacin, ibuprofen or placebo for PDA in preterm infants at >24 h of life.
Results Ten trials compared intravenous indomethacin versus intravenous ibuprofen, nine intravenous indomethacin versus placebo and one intravenous ibuprofen versus placebo. Both intravenous indomethacin (pooled RR 2.39 (95% CI 2.05 to 2.78)) and intravenous ibuprofen (RR 2.40 (95% CI 2.03 to 2.84)) closed a PDA more effectively than placebo. Intravenous ibuprofen was associated with approximately 30% greater risk of chronic lung disease than intravenous indomethacin (RR 1.28 (95% CI 1.03 to 1.60)) or placebo (RR 1.29 (95% CI 0.99 to 1.70)). Differences in risk or benefit were not significant between any combination of intravenous indomethacin, intravenous ibuprofen or placebo groups for intraventricular haemorrhage, necrotising enterocolitis and death. Reporting on neurological outcomes was insufficient for pooling.
Conclusions Intravenous indomethacin or ibuprofen administered to preterm infants for PDA at >24 h of life promoted ductal closure, but other short-term benefits were not seen. Treatment with intravenous ibuprofen may increase the risk of chronic lung disease. Good-quality evidence of treatment effect on morbidity, mortality and improved neurodevelopment is urgently needed.
Statistics from Altmetric.com
Observational studies have suggested an association between echocardiographically and/or clinically important patent ductus arteriosus (PDA) in preterm infants and increased risk of chronic lung disease (CLD), necrotising enterocolitis (NEC), intraventricular haemorrhage (IVH), poor neurodevelopmental outcome and mortality; however, a clear role in causation remains elusive.1 2 In contrast, there is strong evidence of adverse effects arising from the use of intravenous indomethacin to close a PDA within the first 1–3 weeks of life. Examples include brain white matter injury, NEC, intestinal perforation, renal impairment and white cell/platelet dysfunction.2,–,6 Intravenous ibuprofen, developed as a potential alternative to indomethacin, tends to have less vasoconstrictive effect on cerebral, mesenteric and renal arterial beds with improved blood flow.7
What is already known on this topic
▶ Exposure to PDA in preterm infants may increase morbidity and mortality; however, the link between PDA and disease causation has not been clearly demonstrated.
▶ Intravenous indomethacin administered before 24 h of life regardless of PDA status is the only treatment regime to demonstrate any benefit of protection against severe IVH.
▶ Ibuprofen is an alternative to indomethacin with equal efficacy in PDA closure and the potential benefit of less renal and gastrointestinal ischaemia.
What this study adds
Administration of intravenous ibuprofen compared with placebo for clinically important PDA beyond 24 h of life:
▶ is twice as likely to close the PDA compared with placebo;
▶ was not associated with any benefit or harm on the short-term outcomes of NEC, any IVH and death before hospital discharge;
▶ may be associated with an increase in the risk of CLD.
Recent surveys of preterm infant PDA management in the USA and Australia indicated a wide practice variation; from prophylactic indomethacin or ibuprofen to late pharmacological intervention with indomethacin and/or surgical ligation for persistent PDA.8 9 Cochrane systematic reviews have indicated that intravenous indomethacin administered to preterm infants at <24 h of life and regardless of PDA status is the only regime associated with a reduction in short-term risk of severe IVH. Such an approach exposes more infants to adverse effects of indomethacin in the absence of any evidence of benefit on longer-term neurological outcomes.10
Ibuprofen has been investigated as an alternative to indomethacin with benefits of equal efficacy in PDA closure, less transient renal ischaemia and potential reduction in NEC balanced by lack of efficacy in IVH reduction and reports of pulmonary hypertension and haemorrhage with early use.7 11 Intravenous ibuprofen compared with placebo in the treatment of PDA at <24 h of life does not reduce IVH and, in case reports, may be associated with pulmonary hypertension and haemorrhage.7
In preterm infants >24 h of life, the evidence from Cochrane is limited to a direct comparison between the two medications, intravenous ibuprofen and intravenous indomethacin.11 Their review findings indicate that intravenous ibuprofen has equal efficacy in PDA closure, with less transient oliguria.11 This, of course, only represents the comparison of the relative effectiveness of indomethacin versus ibuprofen on PDA closure, related morbidities and mortality; it does not indicate the baseline risks of untreated PDA or potential treatment adverse effects. Previous meta-analyses of intravenous indomethacin versus placebo for echocardiographically and/or clinically important PDA in preterm infants at >24 h of life exist; however, these are in need of updating in light of new trials.12 13 Importantly, there are no direct meta-analyses of intravenous ibuprofen versus placebo in this setting.11
Methods
Search strategy
We searched MEDLINE (1966 to August 2008), EMBASE (1982 to August 2008), CINAHL (up to August 2008), The Cochrane Central Register of Controlled Trials, The Cochrane Library (issue 3, 2008), clinicaltrials.gov and controlled-trials.com. We hand searched abstracts of the national and international American Pediatric Society/Pediatric Academic Societies and The European Paediatric Research Societies and the Effective Care of the Newborn Infant. The authors were contacted for further information regarding unpublished trials and reports found in published databases. Search terms included MeSH: infant, newborn AND ductus arteriosus, patent AND, indomethacin OR ibuprofen OR cyclooxygenase inhibitors AND randomised controlled trial (RCT). No search limits were applied.
Selection
We included all randomised and quasi-randomised trials comparing intravenous indomethacin with placebo, intravenous indomethacin with intravenous ibuprofen and intravenous ibuprofen with placebo in preterm (<37 weeks) or low–birth weight infants (<2500 g) with an echocardiographically and/or clinically important PDA at >24 h postnatal age. Thus, studies providing evidence of echocardiographic (ductal size, left to right shunt, atrial enlargement) or clinical (systolic murmur, hyperactive precordium or bounding pulses) criteria for the diagnosis of PDA or both were included.
The primary outcome for all the studies was PDA closure, and the secondary outcomes were (1) death before hospital discharge; (2) NEC in the neonatal period; (3) IVH, including all grades and/or grade 3 to grade 4; (4) CLD at 28 days and/or 36 weeks, corrected and/or at any age reported and (5) neurodevelopment as measured by Bayley Scales of Infant Development.14 Studies of intravenous indomethacin or intravenous ibuprofen prophylaxis (defined as treatment given at <24 h postnatal age) and regimes including oral forms of indomethacin or ibuprofen were excluded.
Validity assessment
We assessed the methodological quality of all the trials for randomisation, allocation concealment, blinding to intervention and accounting of loss to follow-up using the Jadad Scale with a score of 5 indicating highest quality (table 1)15.
Summary of characteristics and methodological quality of the included studies
Data abstraction
Two authors assessed the methodological quality of the trials and extracted the data. Complete articles were used where possible. Disagreements were resolved with the assistance of a third reviewer.
Quantitative data synthesis
Data were pooled separately according to treatment comparison and outcomes using fixed and random effects models. The effects of intravenous ibuprofen versus intravenous indomethacin and intravenous indomethacin versus placebo were directly compared by pooled risk ratio (RR) using the inverse variance method. The 95% CIs were calculated. Planned sensitivity analyses included trials with (1) quality scores of <3 and ≥3, (2) blinding of operators and participants to study medication versus no blinding, (3) mean age of treatment <72 versus ≥72 h and (4) use of clinical versus echocardiographic criteria for primary case identification. Heterogeneity among studies was assessed using I2 and, where this was significant, was further investigated using sensitivity analyses of post hoc variables mean gestational age at birth <28 versus ≥28 weeks, mean birth weight <1000 versus ≥1000 g and three doses versus one to three doses. Funnel plots were examined for presence of asymmetry indicative of publication bias with further Egger regression testing where appropriate.
This study had two components. First, traditional direct meta-analyses of intravenous indomethacin versus intravenous ibuprofen and intravenous indomethacin versus placebo were performed. Second, these direct meta-analyses were combined using network meta-analysis. Network meta-analysis is a relatively new technique that can be used to indirectly compare the risk or benefit associated with randomly allocated treatments that have not been directly tested against each other. Trials need to have been conducted in populations with similar age and disease profile sharing a common treatment or placebo arm.15 16 We chose to use network meta-analysis to estimate the baseline risk or benefit associated with the administration of intravenous ibuprofen compared with placebo.
Figure 1 represents an example of the graph yielded by the three-way network meta-analysis procedure for the outcome of PDA. The natural logarithms of the RR (logRR) of the two direct meta-analyses, intravenous indomethacin versus intravenous ibuprofen and intravenous indomethacin versus placebo, were derived using χ2 analysis or Fisher exact test (as appropriate) and then fitted into a meta-regression model. A restricted estimation of maximum likelihood function was used in the meta-regression. Indirect estimates of the pooled relative risks (RR) between intravenous ibuprofen versus placebo for the outcomes of PDA closure, death, NEC, IVH and CLD were then estimated. In this manner, we were able to compare the relative benefit or risk of the direct meta-analysis of intravenous indomethacin versus placebo and the indirect network meta-analysis of intravenous ibuprofen versus placebo for the stated outcomes. The incidence of each of these outcomes for the comparators ibuprofen, indomethacin and placebo were pooled and used to calculate the number of preterm infants needed to treat or harm.17 This information allowed us to estimate the sample sizes required to demonstrate a statistically significant result for each outcome in future randomised trials.

Simplified diagram of indirect network meta-analysis.
Analyses were performed using the STATA V.10.0 and Revman V.5.0.18 19 A p≤0.05 was used for statistical significance for all tests except heterogeneity in which 0.10 was used. Sample sizes for future trials were estimated from the event rates for each outcome using a power of 0.8 and α=0.05, with continuity correction where appropriate.
Results
The search yielded a total of 565 citations; the title and abstract of each were screened, and 474 papers were excluded. The remaining 91 papers were examined as potentially relevant RCTs. Twenty-two of these met the inclusion criteria: 3 were later excluded, and 19 RCTs were included across the three meta-analyses (fig 2).

Search results and selection of papers (QUOROM statement flow diagram).
Study characteristics
Table 1 provides details of the characteristics of the 19 trials identified for all three comparisons. Only one trial compared intravenous ibuprofen with placebo; this comparison was thus estimated using indirect network meta-analysis, as described above.
Methodological quality of studies
The methodological quality of the included studies is summarised in table 1. Data for two trials were reported in abstract form only.20 21 Three trials were translated from foreign language papers with English abstracts.22,–,24 Randomisation was adequately described in eight trials; and allocation concealment, in five.22,–,31 Six trials adequately described blinding. Fourteen trials analysed the results according to intention to treat for all outcomes.20,–,27 32,–,37
Findings of the included studies
Primary outcome
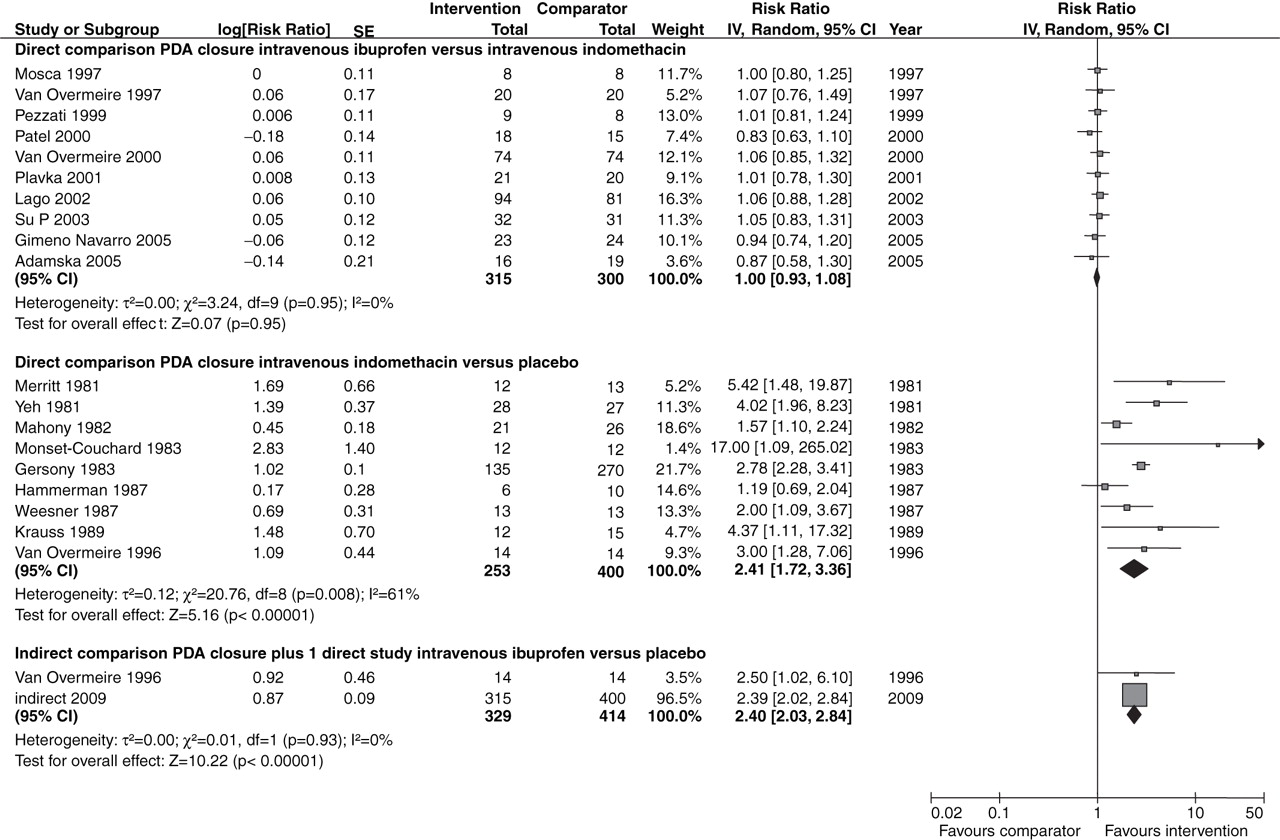
Intravenous indomethacin and intravenous ibuprofen demonstrated equal effectiveness in preterm infants with echocardiographically and/or clinically important PDA at >24 h of life, with both drugs twice as likely to close the PDA compared with placebo. The robustness of this result is supported by a similar finding of no statistically significant difference in PDA closure rates for the direct meta-analysis intravenous ibuprofen versus intravenous indomethacin.
As indicated by the I2 values in fig 3, there was a high level of heterogeneity in effect size between the studies included in the direct meta-analysis between indomethacin and placebo for PDA closure. The sensitivity analyses for all the three treatment combinations including studies with the prespecified variables including mean age at treatment and post hoc variables mean birth weight and mean gestational age (supplementary tables 9a and b) did not change the direction or the statistical significance of the effect estimate for PDA closure with the exception of mean gestational age <28 weeks for the comparison intravenous indomethacin versus placebo in which indomethacin was no longer statistically significantly effective. Despite mild funnel plot asymmetry on visual examination for the comparison of intravenous indomethacin versus placebo, Egger regression asymmetry testing (p=0.5) indicates that publication bias is unlikely; however, the small number of studies may reduce the accuracy of this assessment.
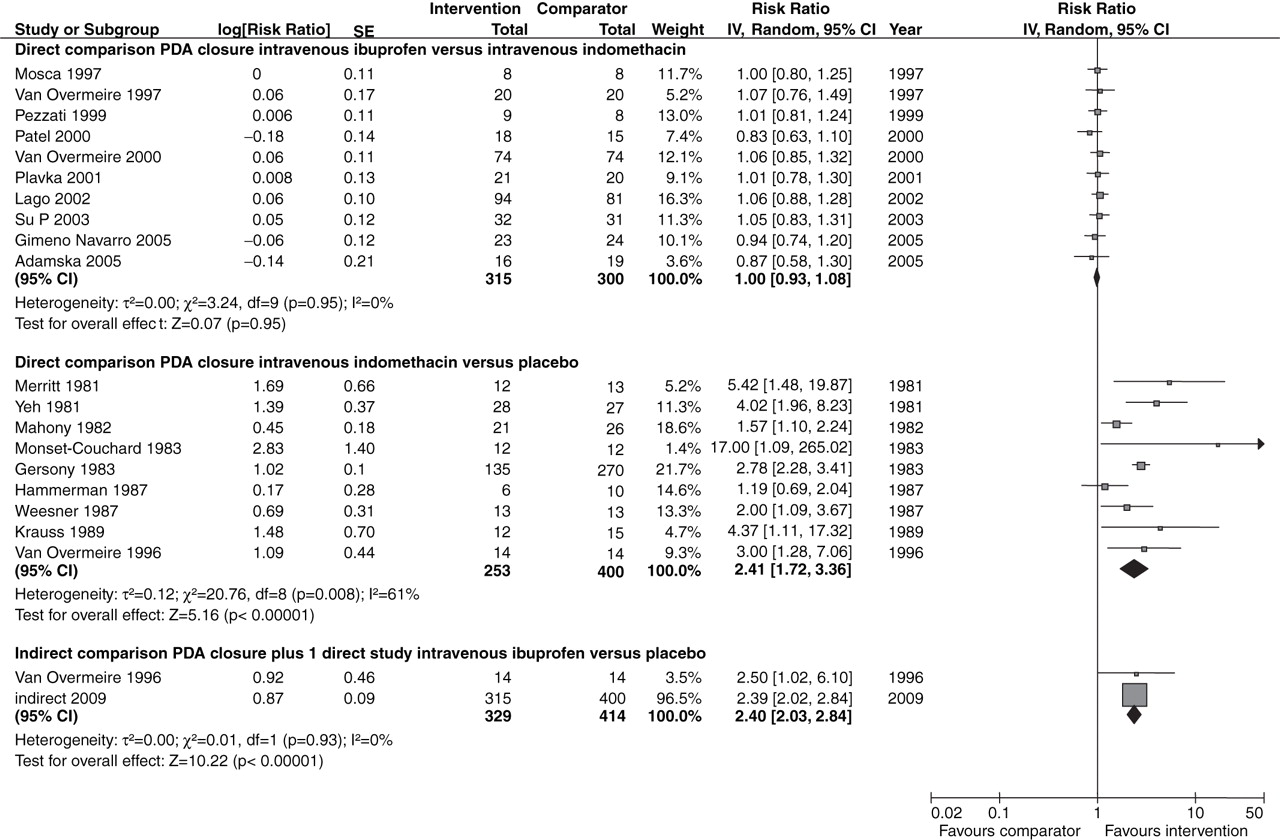
Forest plot of three-way comparison intravenous indomethacin versus intravenous ibuprofen versus placebo, outcome 1: primary outcome: PDA closure (echocardiographically detected and/or clinically important).
Secondary outcomes
The direct meta-analysis of intravenous ibuprofen versus intravenous indomethacin indicated a statistically significant increase in the risk of CLD at any age reported (fig 4) associated with the administration of intravenous ibuprofen for closure of echocardiographically and/or clinically important PDA in preterm infants at >24 h of life.
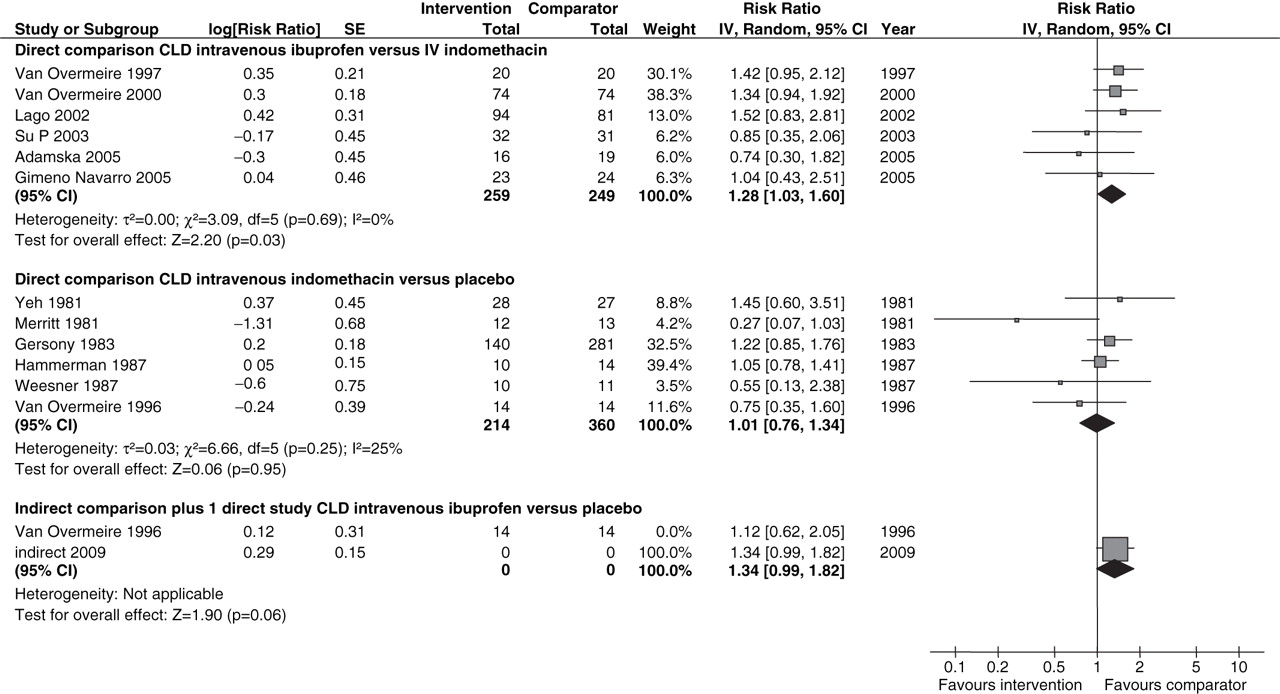
Three-way comparison intravenous indomethacin versus intravenous ibuprofen versus placebo, secondary outcome 1: CLD at any age reported.
The indirect meta-analysis between ibuprofen and placebo indicated an increase in the risk of CLD of borderline statistical significance. The administration of intravenous indomethacin was not associated with a reduction in the risk of CLD in the direct meta-analysis between intravenous indomethacin versus placebo. There was mild between-study heterogeneity in effect sizes for the outcome of CLD in the direct meta-analysis between indomethacin and placebo, which may have resulted from the use of different definitions of CLD or variations in baseline risk of respiratory morbidity between studies. Risk of CLD for intravenous ibuprofen versus intravenous indomethacin remained statistically significantly increased for all sensitivity analyses with the exception of mean age at treatment <72 h.
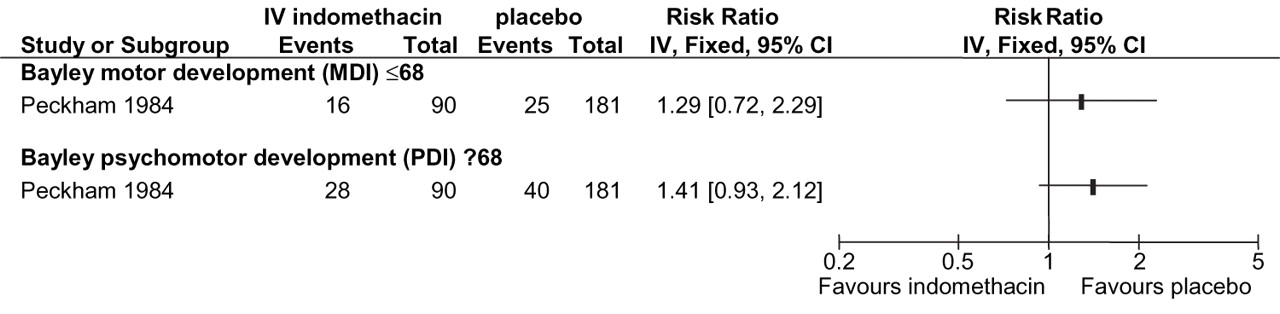
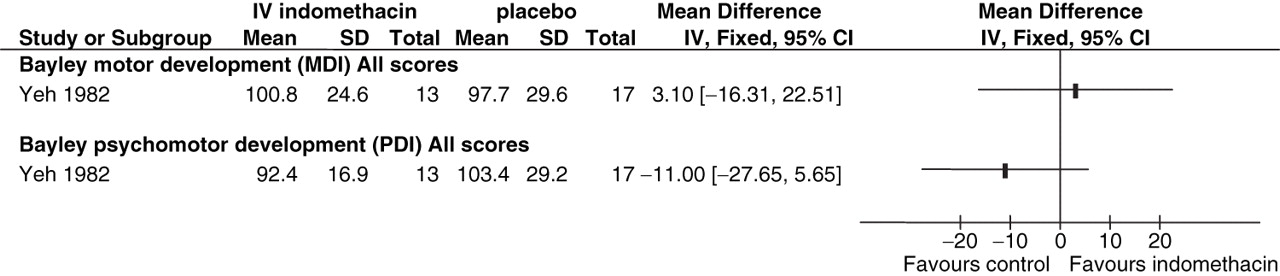
Only two studies reported further on neurodevelopmental outcomes at follow-up. Both studies used the Bayley Neurodevelopmental Scales at 1-year corrected age and compared intravenous indomethacin with placebo; however, because data were presented as mean scores in Yeh and incomplete categorical scores in Peckham, the estimates could not be pooled and were analysed separately.38,–,40 The mean difference between scores or risk of poorer neurological outcomes indicated by a score of ≤68 was not statistically significant between intravenous indomethacin and placebo (figs 5 and 6).

Intravenous indomethacin versus placebo, secondary outcome 5: neurodevelopment at 12 months' corrected age. The mean difference in the Bayley Mental Developmental Index/Psychomotor Developmental Index score.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Intravenous indomethacin versus placebo, secondary outcome 5: neurodevelopment at 12 months' corrected age. Poor neurological outcome indicated by the Bayley Mental Developmental Index/Psychomotor Developmental Index ≤68.
The risks of NEC, IVH and death (supplementary tables 6, 7 and 8) were not significantly different between comparisons of intravenous ibuprofen versus placebo, intravenous ibuprofen versus intravenous indomethacin and intravenous indomethacin versus placebo. There were inadequate studies for IVH and NEC to perform sensitivity analyses.
Funnel plot asymmetry confirmed by a statistically significant p=0.04 on the Egger test was evident in the direct meta-analysis between ibuprofen and indomethacin for death. This indicated a relative absence of smaller studies showing higher estimates of the risk of death associated with intravenous ibuprofen, which may have arisen due to a tendency for smaller, less precise studies with negative outcomes to remain unpublished. Some funnel plot asymmetry was also noted in the comparison between indomethacin and placebo for the outcomes of CLD and death; however, the Egger test (p=0.5) for both outcomes indicates that publication bias is unlikely. Again, the small number of studies included in each comparison may reduce the accuracy of these assessments.
Analysis of the risk-to-benefit ratios for all the outcomes (table 2) indicates that treating 100 preterm infants at >24 h of life with intravenous ibuprofen or intravenous indomethacin rather than placebo may close an additional 33 PDA cases from which the only associated benefit may be the prevention of one case of NEC. PDA closure with intravenous ibuprofen rather than placebo may be associated with 14 extra cases of CLD per 100 infants, 3 extra cases of IVH and 1 death. The results were similar for intravenous indomethacin versus placebo, substituting an extra two cases each of CLD and IVH.
Summary of effect estimates, incidence rates, numbers needed to harm or treat and sample sizes
Discussion
Intravenous ibuprofen administration at >24 h of life in preterm infants was equally effective with intravenous indomethacin in closing an echocardiographically and/or clinically important PDA; however, there was increased risk of CLD at any age reported for intravenous ibuprofen compared with that for indomethacin or placebo. This contrasts with the findings of the most recent Cochrane review, where the differences in the outcome of CLD between ibuprofen and indomethacin did not reach statistical significance at 28 days, 36 weeks' corrected age or at any age reported. Unlike the Cochrane review, which combined studies of oral ibuprofen or indomethacin with intravenous, this review was restricted to trials of intravenous forms, and it is likely that the increased risk of CLD for ibuprofen seen in this review is associated with administration of intravenous rather than oral ibuprofen for PDA closure. There remains the possibility of a protective effect for intravenous indomethacin rather than an increased risk for intravenous ibuprofen in this meta-analysis, which may account for the comparatively lower risk of CLD for intravenous ibuprofen compared with that for placebo. Considering the small difference in incidence rates of CLD between intravenous indomethacin and placebo in comparison with that between intravenous ibuprofen and placebo (table 2), in addition to the wide differences in sample sizes required to achieve adequate power to detect a difference in a randomised trial between the two comparisons, any protective effect for intravenous indomethacin on CLD is likely to be small. The remaining outcomes of NEC, IVH and death show even smaller differences in the incidence rates between indomethacin, ibuprofen or placebo, which is further reflected in the large sample sizes. Lack of benefit for all the measured outcomes in this meta-analysis may be due to the lack of overall treatment effect of PDA closure with the use of intravenous indomethacin or intravenous ibuprofen or as a result of bias due to the use of non-randomised intravenous indomethacin treatment in the placebo group on which the incidence rates are based. Lack of precision indicated by wide CI surrounding the pooled relative risk for all comparisons for the outcomes of NEC, IVH and death is more than likely because of the small size and number of available studies included in the meta-analyses and may have contributed to the null findings.
A few notes of caution should be added to the findings of our review. There may be variation in baseline risk associated with (1) the inclusion of a range of birth weights, gestational ages and ages at treatment within and between the studies with inadequate reporting of outcomes for low birth weight, low gestational age and age at treatment subgroups and (2) potential differences in baseline incidence of outcomes between the direct meta-analyses of ibuprofen versus indomethacin and indomethacin versus placebo used to provide the indirect comparison between ibuprofen and placebo. The latter may be due to time-dependent changes in treatment, diagnostic criteria for determination of PDA and study outcomes and survival of lower–gestational age preterm infants. Many of the studies included in this meta-analysis were small, and this may have impacted upon the estimates of pooled RR, particularly for the outcomes of PDA closure, CLD and death. Assessment of funnel plot asymmetry for the direct comparison of intravenous ibuprofen versus intravenous indomethacin indicates a tendency for the inclusion of small studies to overestimate any protective effect of intravenous ibuprofen towards the risk of death. This may have occurred because of the tendency for small studies to demonstrate larger treatment effects, greater tendency for publication of studies showing positive treatment effects or within- and between-study variations in levels of baseline risk of the measured outcomes in the preterm population.
PDA closure with intravenous indomethacin or intravenous ibuprofen administered for echocardiographically and/or clinically important PDA in preterm infants at >24 h of life was not associated with any reduction in the risk of major morbidity and mortality. Administration of non-randomised intravenous indomethacin treatment to the placebo arm was specified in seven of nine studies in the direct meta-analysis (table 1). The resulting lack of trials comparing either intravenous indomethacin or intravenous ibuprofen against placebo implies that the baseline incidence rates of many of the outcomes included in this meta-analysis had never been established in preterm infants before the widespread use of indomethacin for PDA closure. In addition, the diagnostic criteria for outcomes such as CLD, IVH and PDA, survival of extreme preterms and respiratory management have changed substantially since intravenous indomethacin was first introduced >30 years ago. Intravenous ibuprofen, a relative newcomer, has only ever been tested against intravenous indomethacin, and the increased risk of CLD with the administration of intravenous ibuprofen compared with standard intravenous indomethacin treatment or placebo indicated in our own direct and indirect meta-analyses highlights some concerns regarding the exacerbation of early pulmonary disease in preterm infants. The precise mechanism by which these two medications with similar therapeutic action and efficacy in closing the PDA could have different pulmonary outcomes remains unknown. Perfusion studies indicate that compared with intravenous indomethacin, intravenous ibuprofen has less tendency to reduce cerebral, mesenteric and renal arterial blood flow, whereas a recent experimental study in preterm baboons indicated beneficial effects on lung water clearance and alveolar preservation using either medication.34 35 38 The effect of intravenous indomethacin and intravenous ibuprofen on pulmonary physiology in preterm neonates has been less well studied.
Future RCTs comparing intravenous ibuprofen or intravenous indomethacin administered for echocardiographically and/or clinically important PDA at >24 h of life to placebo should be (1) of good quality, (2) include complete data on lower–birth weight subgroups, length of exposure to PDA and period of outcome measurement and, (3) examine longer-term respiratory and neurological outcomes. The large sample sizes indicated for most of outcomes in this analysis are difficult to achieve in a neonatal population; therefore, a multicentre study is recommended with a minimum sample size required to detect a difference in CLD at 36 weeks' corrected age between intravenous ibuprofen and placebo of at least 130 preterm infants per treatment group. Avoidance of treatment in the placebo arm may reduce the sample size required to detect a difference in benefit and harm between intravenous ibuprofen and placebo or intravenous indomethacin and placebo for all outcomes examined in this analysis.
Acknowledgments
The authors would like to thank the staff of the Neonatal Intensive Care Unit, John Hunter Children's Hospital, and the School of Medicine and Population Health, University of Newcastle, Newcastle, Australia.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online tables
Footnotes
-
Funding LJJ received a full-time University of Newcastle Research Scholarship Central.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.