Article Text

Abstract
Background: Benchmarking is that process through which best practice is identified and continuous quality improvement pursued through comparison and sharing. The Vermont Oxford Neonatal Network (VON) is the largest international external reference centre for very low birth weight (VLBW) infants. This report from 2004–7 compares survival and morbidity throughout Ireland and benchmarks these results against VON.
Methods: A standardised VON database for VLBW infants was created in 14 participating centres across Ireland and Northern Ireland.
Results: Data on 716 babies were submitted in 2004, increasing to 796 babies in 2007, with centres caring for from 10 to 120 VLBW infants per year. In 2007, mortality rates in VLBW infants varied from 4% to 19%. Standardised mortality ratios indicate that the number of deaths observed was not significantly different from the number expected, based on the characteristics of infants treated. There was no difference in the incidence of severe intraventricular haemorrhage between all-Ireland and VON groups (5% vs 6%, respectively). All-Ireland rates for chronic lung disease (CLD; 15–21%) remained lower than rates seen in the VON group (24–28%). The rates of late onset nosocomial infection in the all-Ireland group (25–26%) remained double those in the VON group (12–13%).
Discussion: This is the first all-Ireland international benchmarking report in any medical specialty. Survival, severe intraventricular haemorrhage and CLD compare favourably with international standards, but rates of nosocomial infection in neonatal units are concerning. Benchmarking clinical outcomes is critical for quality improvement and informing decisions concerning neonatal intensive care service provision.
Statistics from Altmetric.com
The Institute of Medicine defines quality as “the degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge”.1 The Vermont Oxford Neonatal Network (VON), founded in 1990, is the largest existing international external reference centre to assist in benchmarking care for very low birth weight (VLBW), ie, birth weight less than 1500 g infants. It is a not-for-profit organisation whose mission is to improve the quality and safety of medical care for newborns and their families through a coordinated programme of research, education and quality improvement.2 3 Since 2003 an all-Ireland collaborative quality improvement project entitled Neonatal Intensive Care Outcomes Research and Evaluation (NICORE) Ireland has been working with VON to evaluate the effectiveness and efficiency of clinical care for newborn infants and their families throughout Ireland and Northern Ireland.
Neonatal units in Ireland are distributed geographically, with 19 public centres in the Republic of Ireland and five centres in Northern Ireland. Each centre has varying levels of activity related to the number of babies delivered and the number of premature or VLBW babies cared for in each unit. Thirteen neonatal centres in Ireland (eight centres in the Republic and five centres in Northern Ireland) currently participate in the NICORE Ireland project. Each centre collects the standardised VON VLBW outcome data, which are recorded and analysed by VON to provide an annual report on mortality and morbidity. This paper focuses on outcome data from 2004 to 2007 to compare survival and key morbidities across Ireland and benchmark results against the VON database. Its aim is to identify key areas for ongoing local and national quality improvement initiatives.
Methods
This collaborative project involves the secure submission of anonymised data from participating neonatal units to the VON. A comprehensive standardised database for all neonatal intensive care episodes for all VLBW infants in participating centres across Ireland and Northern Ireland is thus created from which is generated an annual report. The VON VLBW database includes all infants with birthweight between 401 g and 1500 g born in a participating centre or admitted to it within the first 28 days of life.4 As some patients have complex transfer histories, each participating centre maintains both a patient log and transfer log of eligible infants to identify and track individual patients who are transferred from their centre to other hospitals and to follow their disposition and discharge status.
Each year the VON and NICORE Ireland collaboration have grown, with 13 centres across Ireland contributing data on 796 VLBW infants benchmarking against 682 centres and data on 54 073 VLBW infants in VON in 2007.
What this study adds
This is the first all-Ireland international benchmarking report for neonatal care of VLBW infants.
Survival, severe intraventricular haemorrhage and CLD compare favourably with international standards, but rates of nosocomial infection in neonatal units are concerning.
Benchmarking clinical outcomes is critical for quality improvement and informing decisions concerning neonatal intensive care service provision.
In Ireland, 14 of 25 maternity centres in Ireland contributed data in 2004 and 2005, with 12 participating in 2006 and 13 in 2007 due to difficulties in gathering and submitting data from some centres in the Republic. The 12 maternity centres in the Republic not participating in the NICORE Ireland project have from 951 to 2031 births per annum, with extremely low birthweight (<1000 g) infants born in these 12 centres transferred to the participating NICORE Ireland regional centres for ongoing care. From the available national perinatal reporting system annual reports from the Economic and Social Research Institute we can ascertain that the NICORE Ireland collaboration gathered data on 82% (1333 of the 1602 VLBW infants) born in the Republic of Ireland for 2004–6.5 From the child health system data, electronic patient records and confidential enquiry into maternal and child health forms we know that the NICORE Ireland collaboration gathered data on 97% (738 of the 761 VLBW infants) born in Northern Ireland for 2004–6. Therefore, overall, the NICORE Ireland collaboration gathered data on 87.6% (2071 of 2363 VLBW infants) born in Ireland and Northern Ireland from 2004 to 2006 inclusive.
To allow for case mix, VON calculates a standardised mortality ratio (SMR) for each participating centre to create valid comparisons of survival rates. The SMR is the ratio of observed to predicted deaths at each centre, ie
SMR = observed mortality rate/predicted mortality rate
The observed mortality rate is the proportion of infants with birth weights between 501 and 1500 g who died. The predicted mortality rate is calculated using a multivariable logistic regression model developed by comparing infants from all network centres in the same time period. Infant characteristics used as variables in the regression equation to calculate predicted values include: gestational age (completed weeks) and its squared term, small for gestational age, multiple birth, 1-minute Apgar score, sex, race, location of birth (inborn or outborn), mode of delivery (vaginal or Caesarean section) and four variables to indicate the level of severity of congenital malformation. These birth defect variables indicate severity based on data collected in previous years and are ordered categories from most life threatening to least life threatening. The SMR indicates whether a centre has more or fewer deaths than would be expected based on the characteristics of infants treated at the centre. If the upper bound of the SMR is less than 1, this indicates that the centre has significantly fewer deaths than expected. If the lower bound of the SMR is greater than 1, this indicates that the centre has significantly more deaths than expected. If the lower and upper bounds of the SMR include 1; this indicates that the number of deaths expected is not significantly different from the number of deaths observed, based on the characteristics of infants treated.4
Severe intraventricular haemorrhage (IVH) is defined as either grade 3 IVH with intraventricular blood and ventricular dilation or grade 4 IVH with intraparenchymal haemorrhage identified on either cranial ultrasound or computed tomography of the brain or a magnetic resonance imaging brain scan.
Neonatal chronic lung disease (CLD) is defined as being present if the infant received any supplemental oxygen on the date of week 36 postmenstrual age.
Coagulase negative staphylococcus (CONS) infection (the most common late-onset nosocomial infection seen in neonatal units) is defined as being present when CONS is recovered from a blood culture obtained from either a central line or peripheral blood sample, and/or is recovered from cerebrospinal fluid obtained by lumbar puncture, ventricular tap or ventricular drain and when there are signs of generalised infection (such as apnoea, temperature instability, feeding intolerance, worsening respiratory distress or haemodynamic instability) and treatment with 5 or more days of intravenous antibiotics was administered after the above cultures were obtained. If the infant died, was discharged, or transferred before the completion of 5 days of intravenous antibiotics, this condition would still be met if the intention were to treat for 5 or more days.
Results
Data on 716 VLBW babies in Ireland were submitted in 2004, increasing to 796 in 2007, with Irish centres caring for from a minimum of 10 to a maximum of 120 VLBW infants per year. Of note, seven of the 13 participating centres in Ireland admit less than 50 VLBW infants per annum, ie, less than one per week.
This report from 2004 to 2007 compares survival and morbidity from 2888 VLBW infants throughout Ireland and benchmarks these results against 191 422 infants in the VON database over the same period. There were significantly greater proportions of extremely premature infants delivered at less than 26 weeks’ gestation in the VON group with a similar significantly greater proportion of infants with birthweight below 750 g in the VON group than in the NICORE Ireland group (see table 1).
Proportions of infants admitted to neonatal units born weighing 501–1500 g and gestational age in the NICORE Ireland group and VON from 2004 to 2007
The Irish population is less racially diverse, with slightly greater proportions of infants being inborn, delivered to mothers who had received some prenatal care and a course of antenatal corticosteroids before their preterm delivery than those VLBW infants in the wider VON database (see table 2). Fewer VLBW infants in Ireland were delivered by Caesarean section compared with infants in the VON group (65.2% vs 70%, respectively). There was a slightly higher proportion of small-for-gestational-age infants in the Irish population compared with VON (23% vs 20%). An infant is considered small for gestational age if the birth weight is in the 10th percentile of all US infants, based on the infant’s gestational age and gender and based on maternal race and multiple gestation. The 2001 and 2002 natality datasets provided the database of all US births for determining the 10th percentile values. There was no significant difference between the proportion of infants with congenital malformations between the Irish population and the wider VON (5.7% vs 5.0%, respectively, see table 2).
Characteristics of infants with birth weights between 501 and 1500 g who were born from 2004 to 2007
In 2007, crude mortality rates in VLBW infants across the 13 participating neonatal units varied from 4% to 19%, with the SMR ranging from 0.96 to 1.22. All 13 centres had an SMR in which the lower and upper bounds included 1, indicating that the number of deaths observed was not significantly different from expected, based on the characteristics of infants treated (see table 3). Mortality by birthweight bands was similar when comparing Irish and VON data in 2007 apart from the smallest infants (500–800 g) in which NICORE Ireland and VON mortality rates were 61% and 51%, respectively (fig 1).

Mortality for NICORE Ireland and VON by 100 g birthweight category, 2007. NICORE, Neonatal Intensive Care Outcomes Research and Evaluation; VON, Vermont Oxford Neonatal Network.
Mortality, shrunken SMR (95% CI in parentheses), severe IVH, CLD and CONS sepsis rates, NICORE Ireland, 2007
VLBW survival increased each year between 2004 and 2006, with an Irish VLBW survival rate of 85% compared with a survival rate of 86% for the VON in 2006 and 2007 (table 4). Survival without morbidity (severe IVH, CLD, necrotising enterocolitis, pneumothorax, any late infection or periventricular leucomalacia) also increased over the 4 years from 42% to 48% in the NICORE Ireland group compared with 49% to 51% in the VON group (table 4).
Percentage survival and morbidities for NICORE centres compared with VON centres for VLBW infants 2004–7
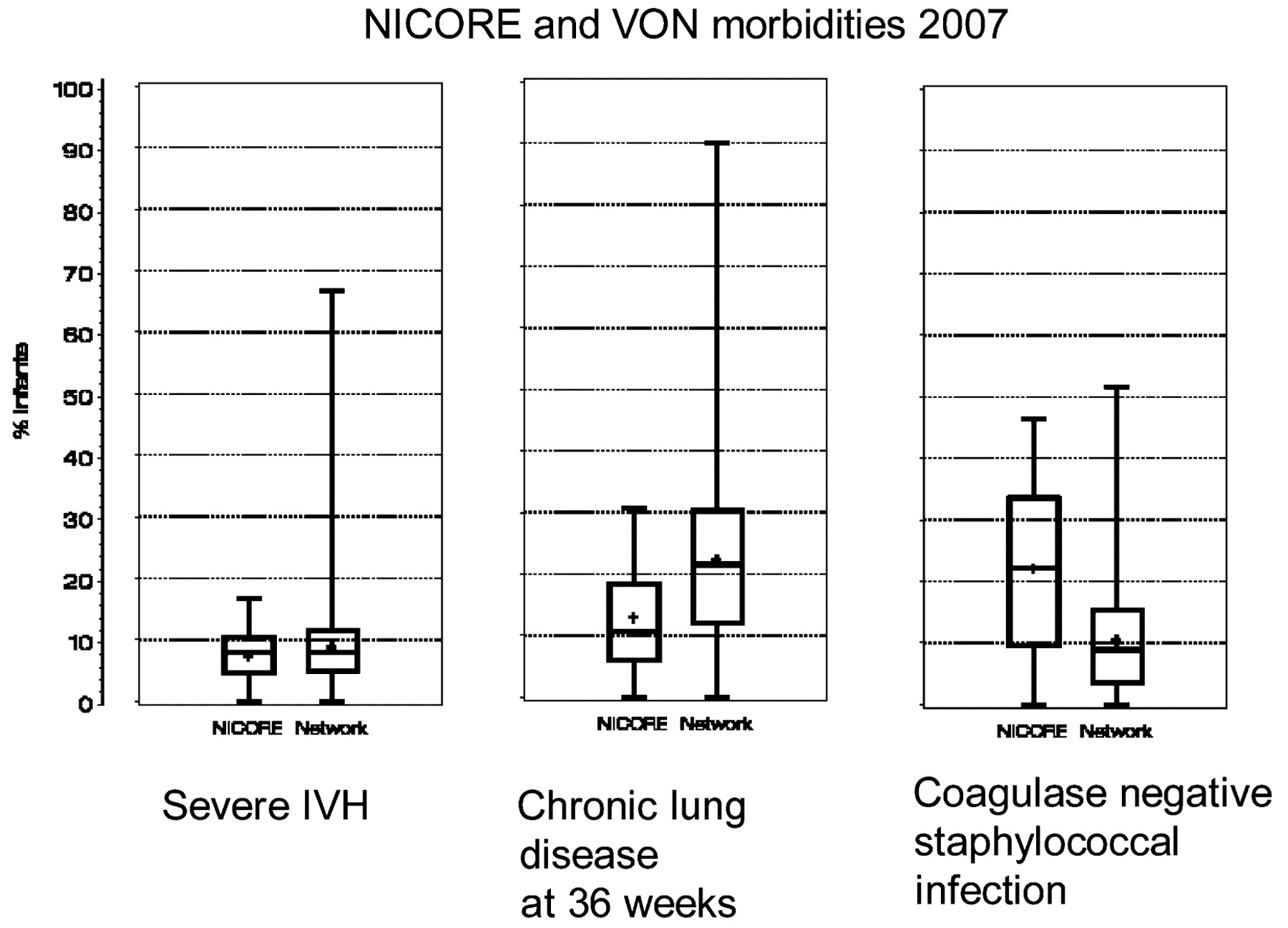
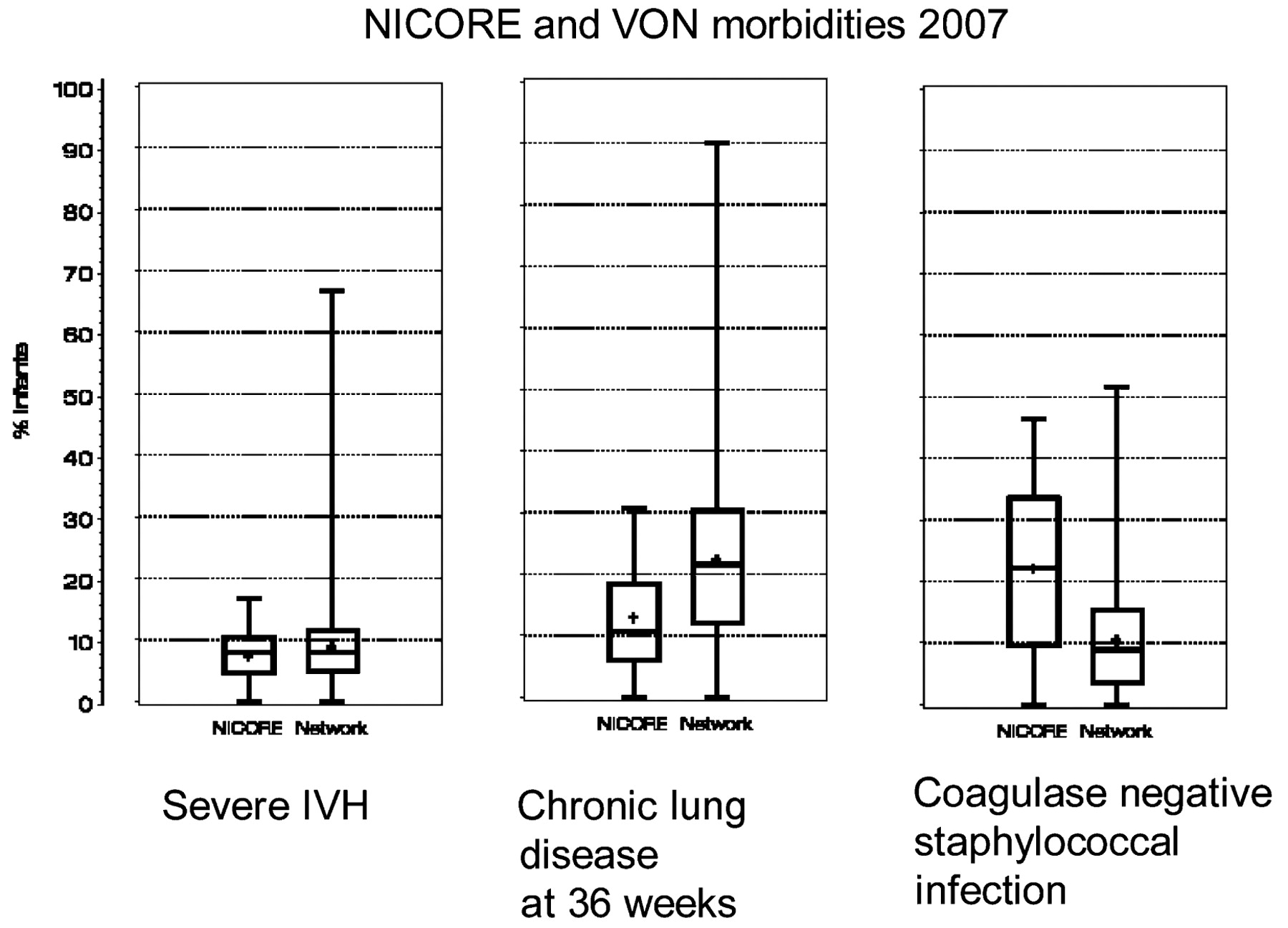
There was no difference in the incidence of severe IVH between the NICORE Ireland and VON groups (5% vs 6%, respectively) in 2007 (table 4, fig 2). The rate of severe IVH has fallen in both groups over the study period. There is variation in the rate of severe IVH across the centres in Ireland ranging from 0% to 18%. Rates of severe IVH below 10% was observed in eight of 13 centres, with the rate ranging between 10% and 18% in the remaining five Irish centres (see table 3).
{kind=link}
{kind=link}
Each box plot presents a rectangular box with a pair of whiskers extending from its ends. The “whiskers” represent the extremes of the data (minimum and maximum), while the box represents the central portion of the distribution. The top edge of the box represents the 75th percentile of the distribution and the bottom edge of the box represents the 25th percentile of the distribution. The line across the middle of the box represents the median. The cross represents the mean value of all of the hospitals. IVH, intraventricular haemorrhage; NICORE, Neonatal Intensive Care Outcomes Research and Evaluation; VON, Vermont Oxford Neonatal Network.
The NICORE Ireland rates for CLD of 15–21% have been consistently lower than rates seen in the VON group (24–28%; table 4, fig 2). There is wide variation between Irish centres, with rates of CLD ranging from 0% to 31%, with rates below 10% in four centres, 10–20% in seven centres and greater than 20% in two centres (see table 3).
The rate of CONS sepsis at 25–26% across all 4 years in the NICORE Ireland group is consistently double the corresponding incidence (12–13%) observed in the wider VON network (table 4, fig 2). In 2007, three centres had a CONS sepsis rate below 10%, three centres had CONS sepsis rates between 10% and 20%, but seven centres had CONS sepsis rates above 20%, with four centres above 30% and one centre with 46% (see table 3).
The three morbidities, severe IVH, neonatal CLD and CONS infection for NICORE Ireland centres and VON are illustrated as box plots (see fig 2). Each graph provides information about the overall distribution of the observations, one representing the NICORE Ireland group and the other the VON.
There was no difference comparing any of the other morbidities studied (necrotising enterocolitis, pneumothorax and periventricular leucomalacia) between NICORE Ireland and VON.
Discussion
This is the first all-Ireland international benchmarking report in any medical specialty. This report utilising data submitted by NICORE Ireland to the VON permits us to benchmark neonatal care and infant outcomes for VLBW infants in Ireland and Northern Ireland both nationally and internationally. There were significantly greater proportions of extremely premature infants at less than 26 weeks’ gestation with birthweight below 750 g in the VON group than in the NICORE Ireland group yet survival and survival without morbidity has been consistently better in the VON group than in the NICORE Ireland group throughout this period. Over the 4-year period in the NICORE Ireland group survival increased from 81% to 85%, bringing it in line with survival for the overall VON. In both groups survival without morbidity remained relatively constant at approximately 50%.
There is marked variability across the centres in Ireland and Northern Ireland when looking at crude survival data, but as seen from the SMR, survival in all centres in NICORE Ireland compares favourably both nationally and internationally when the case mix and illness severity of infants cared for in each unit are taken into consideration.
The levels of severe IVH are reducing and are comparable across NICORE Ireland and VON, with an incidence of approximately 5–6% across both in 2007. This reduction in rates of severe IVH may reflect both improvements in prenatal care and an increase in the use of antenatal corticosteroids, which when given to mothers at risk of preterm delivery have been demonstrated to protect against IVH in premature VLBW infants.6 Significantly more mothers in the NICORE Ireland group delivering between 24 and 34 weeks’ gestation appropriately received antenatal corticosteroids and received prenatal care compared with mothers of VLBW infants in the VON.
Neonatal CLD is a condition with multifactorial causes related to prematurity and vulnerability of VLBW infants to lung injury from a host of factors including ventilator-induced lung injury, infection and inflammation.7 8 The lower rates of CLD reported by NICORE Ireland compared with VON could reflect differences in the delivery of respiratory, nutritional and other supports to these infants. The risk of CLD is also influenced by growth restriction in a population and some of the observed differences seen between NICORE Ireland and VON could be related to the significantly increased rate of SGA infants in the NICORE Ireland group compared with VON (23% vs 20%). The definition of neonatal CLD used by VON (requirement for oxygen at 36 weeks postmenstrual age) takes no account of the variation in oxygen saturation limits, which may differ between units affecting decisions related to the use of oxygen and measures of respiratory morbidity.9 10 An objective definition of neonatal CLD would permit more accurate benchmarking, as the current definition utilised by VON and other international networks does not quantify disease severity. The predominant gas exchange impairment in neonatal CLD is a reduced ventilation/perfusion ratio, which can be described by the right shift of the oxygen saturation versus inspired oxygen pressure relationship.11 This provides a simpler method for defining neonatal CLD and grading disease severity, permitting more accurate comparison across networks. Although rates of 15–20% for CLD compare favourably with VON rates of 24–28%, these rates are still higher than the lowest rate of 4% consistently reported by one tertiary centre in the USA.12 By comparison of outcomes such as CLD and sharing information about the processes around the delivery of care, multidisciplinary teams in our neonatal units can learn from each other, promoting best practice across all centres in our network.
CONS sepsis, as strictly defined by the VON, is the commonest late-onset nosocomial infection seen in neonatal units. CONS infection remained significantly higher in NICORE Ireland units than in the VON, with wide variability across units from 4% to 46% in 2007. Although most infants survive CONS infection, increasing evidence is emerging that such infection may be associated with prolonged hospital stay, brain injury and adverse neurodevelopmental outcome, mediated by white matter abnormalities on magnetic resonance brain imaging.13 14 In 2008, the National Hygiene Services Quality Review carried out by the Health Information and Quality Authority outlined that collection and reporting data for hygiene services, evidence-based practice, new interventions in hygiene services, assessment and strategies for improving performance and enhancing staff performance were all areas that needed more focus across all Irish hospitals.15 The high CONS infection rates in VLBW infants in Ireland suggest that much greater cooperation between neonatal units is needed to examine practices and strategies that may reduce such infection rates. Such cooperation should be encouraged and supported as undoubtedly care practices within units contribute greatly to these infection rates.
The VON uses a variety of risk adjustment methods to compensate for the differences in case mix among centres, but it is important to realise that these methods are imperfect. Even the best statistical risk models cannot adjust for all of the differences in case mix among neonatal intensive care units, nor can they filter all of the random variation. Given these caveats, however, we believe it is appropriate to use these data to target specific clinical practices and patient outcomes for further indepth analysis with the goal of identifying potential quality improvement opportunities.
Whereas the average survival and morbidity outcomes in Ireland are similar to the VON, there are wide variations within the all-Ireland reports that need to be addressed. Although some centres are close to the mean, several centres are outliers with respect to key clinical morbidities, in particular late-onset nosocomial infection. It has been demonstrated that there is a distinct relationship between registered nurse staffing levels and healthcare-associated bloodstream infections in infants in neonatal intensive care units.16 No neonatal unit in Ireland is currently staffed as recommended by the British Association of Perinatal Medicine standards for hospitals providing neonatal intensive and high dependency care.17
We believe that the wide variability in outcomes seen between centres in Ireland lends support to the creation of more formalised perinatal (maternity and neonatal) clinical networks as developed in some parts of the UK since 200418 and outlined in the recent report on “The future of maternity and gynaecology services in Ireland” produced by the Irish Institute of Obstetrics and Gynaecology.19
Ongoing collection and benchmarking of data is critical for implementation and evaluation of quality improvement initiatives both locally and nationally. Locally, it is important to present results back to each unit and it is incumbent on clinicians to understand and address their outcomes. Regionally and nationally, the development of quality improvement programmes could include the provision of support (eg, newsletters, visits, toolkits, care bundles for potentially better practices, website) to all centres via perinatal clinical networks with regular meetings of steering groups representing all participating units. The reports generated by VON for the NICORE Ireland project are intended for use as one component of a continuous programme for ongoing collaborative quality improvement.20 21
Auditing and benchmarking of clinical outcomes should be mandatory for all maternity centres in Ireland in the 21st century. Due to a lack of standardised records, most of which are paper based, NICORE Ireland captures data on 82% of VLBW infants born in the Republic of Ireland compared with 97% of VLBW infants captured by the computerised child health system utilised in Northern Ireland. An internationally agreed standardised electronic perinatal database across Ireland, the UK and Europe in conjunction with VON would facilitate local, regional, national and international benchmarking against VON, European comparators such as EuroNeoStat, or indeed perinatal networks within Ireland, the UK or Europe. The information obtained from analysis of such audit and benchmarking is important for research, clinical governance activities and collaborative quality improvement. We believe such information is essential for informing decision making regarding neonatal critical care service provision in Ireland.
Acknowledgments
The authors wish to thank all the data collectors in all of the participating hospitals for their continuing efforts at quality improvement for VLBW infants across Ireland. They also wish to thank Dr Jeffery Horbar and all their colleagues at the Vermont Oxford Network who continue to offer collective advice and support to this collaborative project.
REFERENCES
Footnotes
Funding In Northern Ireland, the Department of Health, Social Services and Public Safety provided full funding for the Northern Ireland part of the project. The southern part of this project was initially funded by the Department of Health and Children for a pilot period of 3 years. It now works in partnership with the National Perinatal Epidemiology Centre at Cork University Maternity Hospital.
Competing interests None.
Provenance and Peer review Not commissioned; externally peer reviewed.
Linked Articles
- Fantoms